

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Suicide is a leading cause of death among adolescents and has become a significant public health issue globally (1). Statistics Korea report 2014 showed that suicide is the cause of 28.4% of adolescent deaths in 2013, and it was the number one cause of death among adolescents (2). Furthermore, suicide is the second to third cause of mortality among adolescents in the Western world and is an important concern in developing countries (3). Numerous causes of suicidal behavior during adolescence have been reported, including mental disorders, peer affiliations, and level of achievement in school (4). Additionally, weight-related concerns are a common cause of suicidal behaviors (56).
Adolescents experience rapid changes as they develop from children into adults. This transition often leads to confusion about personal identity, especially in the context of enduring developments in identity and cognition as well as physical growth (7). Adolescents typically enter a period of a high level of self-consciousness about their body shape and size (8). They have a greater tendency to consider how they look to others at this life stage than during any other period of life (9). These weight-related issues are influenced by many factors including friends, peers, social norms, and media (10). The media is a particularly strong influence because it has become a general source of information and adolescents are easily exposed to it (11). The media encourages as "ideal" slim and thin body shapes for girls and muscular bodies for boys (1213), and provides abundant information on the newest diet methods and quick fixes for weight control (14). This may induce adolescents, who have a particularly keen interest in their figure, to distort their body image and to engage in unneeded or inappropriate weight control behaviors (WCB) (15).
Many adolescents engage in inappropriate WCB such as vomiting, taking nonprescription diet pills, and taking laxatives or diuretics. Among Korean adolescents engaging in WCB, 13.4% of boys and 18.8% of girls took inappropriate methods to control their weight (16). According to a study using data from national surveys, similar rates were also observed in the United States, with 10% of boys and 21.3% of girls conducting at least one inappropriate WCB (17).
Inappropriate WCB are a harmful influence on adolescents' physical and psychological development (12). For instance, a 5-year longitudinal study reported that engagement in inappropriate WCB can be a predictor of obesity and eating disorders (18). Moreover, adverse outcomes of inappropriate WCB also include the onset of depression (19) and suicide ideation (20). Due to the high prevalence of and the possible negative side effects associated with inappropriate WCB, it is a growing serious public health concern. Therefore, the prevention of inappropriate WCB among adolescents is imperative to protect them from negative physical and psychosocial consequences.
To date, studies about inappropriate WCB merely suggest the association between inappropriate WCB and negative psychosocial consequences (212223). In the present study, we investigate not only the association between inappropriate WCB and suicide ideation and attempt, but also the difference in this association with body mass index, body weight perception, and body shape misperception. Moreover, we investigate the top five WCB combinations used by Korean adolescents and examine the association between these five WCB combinations and suicide ideation and attempt. We used a cross-sectional design; thus, the results should be interpreted with caution due to possibility of a bi-directional effect.
MATERIALS AND METHODS
Data and participants
We used data from the 2014 Korea Youth Risk Behavior Web-based Survey (KYRBS). The KYRBS has been conducted annually since 2005 by the Korean Centers for Disease Control and Prevention (KCDC), the Korea Ministry of Education, Science and Technology, and The Korea Health and Human Services. The data were collected via an ongoing, anonymous web-based survey in a self-reporting format that was conducted on a nationally representative sample of middle- and high-school students. It aimed to plan and assess the Korean adolescent health promotion policies by investigating health-related behaviors and status. In the 2014 survey, 799 middle and high schools were selected, including 72,060 students in grades 7 to 12 (stratified) on a national scale. However, we excluded 2,334 individuals due to missing data for variables used in this study; therefore, our cohort ultimately comprised 69,726 adolescents (35,224 boys and 34,361 girls).
Variables
The dependent variables used in this study include suicide ideation and suicide attempt. Suicide ideation and attempt were measured via responses to the following questions: "Have you seriously considered suicide during the past 12 months?" and "Have you tried suicide during the past 12 months?" The possible responses to both questions were "yes" or "no."
The key independent variable of interest was weight control behavior (WCB). We characterized WCB via responses to the following multi-part question: "Have you experienced the following weight control methods during the past 30 days, with the following activities listed: 1) did regular exercise, 2) fasted at least 24 hours, 3) ate less, 4) took prescription diet pills, 5) took nonprescription diet pills, 6) took laxatives or diuretics, 7) vomited, 8) ate only one food, 9) took oriental medicine, and 10) ate diet food." The possible responses to all questions were "yes" or "no." If participants responded 'yes' to at least one of 2), 5), 6), 7), and 8), we classified them into the "inappropriate WCB" group (16). If participants responded 'no' at all of 2), 5)-8), we classified them into the "appropriate WCB" group. If participants responded 'no' to all activity choices, we classified them into the "nothing" group. Body mass index (BMI) was calculated by self-reported height and weight. BMI percentiles for age and gender were calculated according to the 2007 standard growth charts for Korean children and adolescents by the Korean Pediatric Society (24), and four categories were created: underweight (≤ 15th percentile), normal weight (16th to 84th percentile), overweight (85th to 95th percentile), and obese (≥ 95th percentile or BMI ≥ 25). We further grouped overweight and obese groups into a single overweight group, thus using three BMI categories Body weight perception (BWP) was split into five categories: very underweight, underweight, normal weight, overweight, and very overweight. We further grouped these categories into three groups: thin, normal, and obese. Body shape misperception (BSM) was determined by an agreement between BMI and BWP categories. Participants perceiving their weight at least one category below their actual BMI categories were designated part of the "underestimate" group, while those perceiving their weight at least one category above their actual BMI were designated part of the "overestimate" group (i.e., if participants whose BMI was a normal weight perceived their body weight as obese, they were placed in the "overestimate" group) (25).
Control variables included age, household economic status, parents' presence, residential area, school level, academic achievement in school, subjective health status, sleep satisfaction, physical activity, current alcohol consumption, current smoker, stress level, and depression.
Statistical analyses
We performed statistical analyses of the survey data using SAS version 9.4 (SAS Inc., Cary, NC, USA). The relevant primary sampling units, sample weights, and stratification were considered in the analysis given that the KYRBS was designed as a complex sample. A Pearson's χ2 test was used to determine significant differences in the distribution of each variable. Next, a logistic regression analysis was conducted to determine the association between WCB and suicide ideation and attempt. Separate analyses were conducted by gender to address differences in association with gender. Additionally, we performed a set of subgroup analyses using BWP, BMI, and BSM to determine whether body related variables led to differences in the association between WCB and suicide ideation and attempt. Results were presented as adjusted odds ratios (ORs) with 95% confidence intervals (95% CIs).
Ethics statement
The ethics approval for the publicly open KYRBS data was waived by the institutional review board (IRB). After the purpose of the survey was fully explained to the students, written informed consent was provided. Students were assured that they could refuse or withdraw from the research at any stage (16). The KYRBS did not collect any personal identifiable information and guaranteed anonymity and confidentiality.
RESULTS
The demographics of the 35,224 boys and 34,361 girls in this study are listed in Table 1. Of the participants, 10.6% (n = 3,709) of boys and 15.0% (n = 5,172) of girls reported that they experienced suicide ideation, while 2.1% (n = 722) of boys and 3.4% (n = 1,151) of girls reported attempting suicide. Of the participants, 33.5% (n = 11,827) of boys and 45.2% (n = 15,489) of girls reported that they engaged in appropriate WCB, and 4.2% of boys (n = 1,466) and 9.6% of girls (n = 3,324) reported that they engaged in inappropriate WCB.
Table 1
General characteristics of the study population

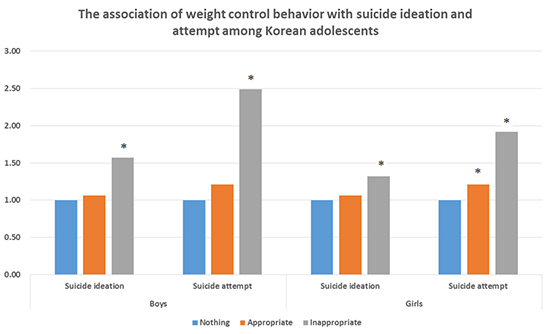
The odds ratios of factors associated with suicide behaviors are listed in Table 2. Boys who had engaged in inappropriate WCB were more likely to report suicide ideation than those not engaging in WCB group (OR, 1.57, P < 0.001). Girls engaging in inappropriate WCB also had a high suicide ideation rate (OR, 1.32, P < 0.001). Boys engaging in inappropriate WCB were also more likely to attempt suicide than those not engaging in WCB (OR, 2.49, P < 0.001). Girls engaging in appropriate WCB (OR, 1.21, P = 0.02) or inappropriate WCB (OR, 1.92, P < 0.001) were more likely to attempt suicide than girls not engaging in WCB at all, and the association was stronger among the latter comparison group.
Table 2
Factors associated with suicide ideation and attempt by gender

The association between suicidal behavior and WCB stratified by BMI, BWP, and BSM is shown in Table 3. Boys with an underweight BMI and that engaged in inappropriate WCB experienced the highest rate of suicide ideation (OR, 2.22, P < 0.05) compared to other BMI groups. Girls with an underweight BMI and that engaged in inappropriate WCB were 4.53 times more likely to attempt suicide than girls who did not engage in WCB. Girls who perceived their weight as normal and engaged in inappropriate WCB were more likely to experience suicide ideation (OR, 1.50, P < 0.001) and attempt (OR, 2.31, P < 0.001) than girls who did not engage in WCB. Considering BSM, boys who distorted their body shape and who engaged in inappropriate WCB were more likely to experience suicide ideation (underestimate: OR, 1.44, P < 0.01, overestimate: OR, 1.91, P < 0.01) and attempt (underestimate: OR, 1.96, P < 0.01, overestimate: OR, 2.94, P < 0.01) than boys who do not engaged in WCB. Girls who underestimated or overestimated their body shape and engaged in inappropriate WCB showed significant association with suicide attempt (underestimate: OR, 1.89, P < 0.001, overestimate: OR, 1.73, P < 0.001) compared to girls who do not engaged in WCB.
Table 3
Subgroup analysis of the association between weight control behavior and suicide behaviors stratified by body mass index, body weight perception, and body shape misperception
Adjusted for age, sex, household economic status, parents presence, residential area, school level, academic achievement, subjective health status, sleep satisfaction, physical activity, current alcohol consumption, current smoker, stress status, and depression.
OR, odds ratio.
*Cannot be calculated due to the lack of number.
Table 4 lists the odds ratios of the top five WCB combinations engaged in by Korean adolescents and their association with suicide behaviors. Conducting regular exercise and eating less together with fasting was significantly associated with suicidal ideation (Boys: OR, 1.70, P < 0.01, Girls: OR, 1.33, P < 0.05) and attempt (Boys: OR, 1.84, P < 0.05, Girls: OR, 2.24, P < 0.001) among both boys and girls, and girls had higher rates of attempted suicide.
Table 4
Odds ratios of combinations of weight control behaviors with suicide behaviors by gender
Adjusted for age, sex, household economic status, parents presence, residential area, school level, academic achievement, subjective health status, sleep satisfaction, physical activity, current alcohol consumption, current smoker, stress status, and depression.
OR, odds ratio.
*Weighted percentage among weight controller.
DISCUSSION
In the present study, we investigated association between inappropriate WCB and suicide ideation and attempt by Korean adolescent by using nationally represented data. Inappropriate WCB was significantly associated with suicidal behaviors in both boys and girls, and with a higher rate in boys.
Our study findings of a higher likelihood of suicidal behaviors among adolescents engaging in WCB (especially inappropriate WCB), confirm results described in previous studies. Adolescents using inappropriate methods to control weight are highly likely to experience psychological symptoms including anxiety, fatigue, and impaired concentration (26). Additionally, there is a prospective association between WCB and depression (27). Depression in adolescence is a serious public health concern due to the increased risk of suicide among depressed youth (28). Moreover, WCB can cause eating disorders, with fasting an especially high risk factor for development of eating disorders (29). Another study among adolescents and with a 5 year follow up reported that unhealthy WCB were the most powerful predictors of eating disorders (18). Eating disorders have adverse consequences on adolescents' physical and mental health (30), and can cause suicide ideation and attempt (31). Therefore, one possible interpretation of this finding is that WCB represent a risk factor for suicide ideation and attempt by causing depression or eating disorders, both of which have serious consequences on adolescents' mental health. Furthermore, our study demonstrated stronger associations among boys than girls, which is corroborated by other studies (623). Girls are more sensitive to their weight and easily engage in inappropriate WCB (32), whereas boys are not as sensitive about their weight and have a lower likelihood of engaging in inappropriate WCB (7). Therefore, it is possible that boys who consider controlling their weight in inappropriate ways may already be suffering from severe psychological distress due to experiencing immense trauma from teasing or other adverse events.
We investigated differences in association between suicide ideation and attempt and WCB by conducting subgroup analyses using BMI, BWP, and BSM. In the context of BMI, underweight boys engaged in inappropriate WCB experienced the highest rate of suicide ideation and attempt than other BMI groups, and underweight girls were considerably more likely to attempt suicide. Additionally, suicidal behavior was also associated with boys and girls of a normal weight engaged in inappropriate WCB. This suggests that adolescents who do not need to control their weight but engage in unnecessary WCB nonetheless are at higher risk for experienced adverse consequences (12). With regards to BSM, the results of this study showed that misperception of body shape is also associated with suicide ideation and attempt. The media continues to portray slender bodies for girls and muscular bodies for boys as ideal body shapes, and this could have an effect on body shape misperception among adolescents (33). This mismatch contributes to adolescent depression, which in turn increases the risk of suicide among youth (34). Moreover, this mismatch could be related to adolescents' unnecessary weight control behaviors to obtain the ideal body shape. Eventually, the effect of inappropriate WCB aggravates adverse effects from a distorted body image, and it seems that this psychological burden causes adolescents to think about or attempt suicide.
We also extracted the five most common combinations of weight control methods used by Korean adolescents and investigated the association between these WCB and suicidal behaviors. Only conducting regular exercise was the most frequent WCB among boys and the third most common among girls. However, this combination was not significantly associated with suicidal behaviors in boys or girls. The most common WCB engaged in by girls was 'regular exercise and eating less', and it also did not show any significant association with suicidal behaviors. Interestingly, both boys and girls engaging in 'regular exercise, fasting, and eating less' were more likely to experience suicidal behaviors compared to those who did not conduct any WCB. Although regular exercise and eating less are both appropriate WCBs, when fasting, which is classified as an inappropriate WCB, is added, this combination could contribute to adolescents' suicidal behaviors. According to a previous study, fasting for weight control showed an association with depression when compared with other WCBs (35). In practice, fasting causes the blood glucose concentration to fall below normal, and this status releases the hormone cortisol, which is associated with anxiety and negative feelings (36). Therefore, it seems that this combination influences suicidal behaviors due to the strong influence of fasting on depressive symptoms.
The results of this study should be interpreted with caution due to several limitations. This study was designed as cross-sectional study; therefore, we could not exclude the potential bi-directional effect. In addition, the time frames of WCB (within the past 30 days) and suicide ideation and attempt (within the past 12 months) differed. Therefore, a reverse-time order could not be clearly excluded (6). Moreover, responses from the KYRBS represent self-reported data, and therefore may be inaccurate. Additionally, we could not obtain detailed descriptions of each WCB including frequency or amount. However, despite the limitations, this study can be generalized by using nationally representative data. Additionally, compared to previous studies that only reported associations between WCB and suicidal behavior, we further investigated differences in this association in the context of BMI, BWP, and BSM. Moreover, this is the first study to investigate common WCB combinations and to determine the association between the top five such combinations and suicide ideation and attempt. Considering that the high incidence of suicide and the severe negative impact of adolescents' inappropriate WCB on their health, our findings represent an important motivation for health policy makers to identify solutions for controlling adolescents' suicide problem.
Inappropriate WCB among adolescents is a serious public health concern considering its widespread prevalence and harmful influence on growth, physical health, and psychosocial growth. Additionally, as shown here, WCB can be associated with health compromising behaviors including suicide ideation and attempt. Therefore, to protect adolescents' healthy psychological status in the context of weight concerns, policy makers and health professionals must endeavor to correct the distorted body perception experienced by adolescents. Additionally, they should help adolescents develop skills for avoiding inappropriate WCB, and encourage appropriate methods of weight control such as physical activity, fruit and vegetable consumption, and the avoidance of fatty and sweet foods. Future studies should be designed regardless of gender or weight status because boys and normal or underweight adolescents are currently low priority even though they are also at risk for adverse effects due to WCB according to the present study. Therefore, broader viewpoints and approaches are needed when considering adolescents' weight-related behaviors.
 XML Download
XML Download