

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Use of magnetic resonance imaging (MRI) is rapidly increasing for diagnostic purposes in many fields (e.g., the brain, spinal cord, and musculoskeletal system). About 50%-70% of the patients with cardiac implantable electronic device (CIED) will be estimated to have an indication for a MRI over the lifetime of the device (1). However, MRI has been traditionally contraindicated in patients with CIED owing to potential risk to the patient or device (23).
Recently, MRI conditional pacemaker system (EnRhythm MRI SureScan implantable pulse generator and CapSureFix MRI lead [5086 lead], Medtronic, Inc., Minneapolis, MN, USA) showed no adverse effect on either the patient or the pacemaker system in a magnetic resonance environment (4). Based on these results, this Medtronic pacing system became the first MRI conditional pacing system in the United States approved by the Food and Drug Administration (FDA) (5).
The 5086 MRI lead was modified to reduce radiofrequency lead tip heating. These modifications resulted in the larger diameter and greater stiffness of the leads compared to the conventional Medtronic CapSureFix Novus 5076 non-MRI pacing lead (5076 lead). As a result, the 5086 lead has been reported to be associated with increased cardiac perforation and lead dislodgement (678). However, these results were not consistent with previous results (4910). Moreover, to our knowledge, there was no Asian data on the safety of the 5086 lead. Therefore, this study aimed to compare cardiac perforation and lead dislodgement between the 5086 lead and the previous 5076 lead.
MATERIALS AND METHODS
Patient population
This was a multicenter retrospective study, which included 482 consecutive patients who underwent permanent pacemaker implantation with the 5086 lead (277 patients, 57.5%) or the 5076 lead (205 patients, 42.5%) between March 2009 and September 2014. The choice of the pacing lead depended on the operator's discretion. All patients received dual atrial and ventricular pacing leads for atrioventricular block (n = 241, 50.0%), sick sinus syndrome (n = 230, 47.7%), and both (n = 11, 2.3%). The study populations meet inclusion criteria. Inclusion criteria were; 1) patients older than 18 years of age, 2) patients without known pericardial effusion and an additional pacing lead implanted within 30 days prior to implant, and 3) patients who participated in follow-up for 30 days after implant. Clinical data was retrospectively analyzed.
Lead characteristics
Both 5086 and 5076 leads are steroid-eluting with screw-in active fixation. Lead polarity (bipolar), standard length (52 cm and 58 cm), lead tip surface (4.2 mm2), ring electrode (22 mm2), tip-ring spacing (10 mm), and inner and outer insulation (silicone) are identical in both leads. The differences between two leads are inner coil (2 filars in 5086 lead vs. 4 filars in 5076 lead) and lead body diameter (2.3 mm in 5086 lead vs. 2.0 mm in 5076 lead).
Endpoint
The primary endpoint was the incidence of cardiac perforation within 30 days after pacemaker implantation. Cardiac perforation was defined as a radiographic evidence of excursion of the pacing lead into the pericardial sac, and abnormal echocardiography indicative of a perforation, the accumulation of fluid in the pericardium with cardiac tamponade. The second endpoint was lead dislodgement within 30 days of implantation. Definition of the lead dislodgement was the movement of the pacing lead from its originally implanted position resulting in elevated pacing thresholds or a decrease in sensing (11).
Chest radiography was performed immediately after pacemaker implantation, and was followed daily before hospital discharge and first follow-up visit within 30 days. The post-procedural echocardiography was performed by physician's discretion depending on patient's symptom (chest pain/discomfort or dyspnea) and hemodynamic instability, newly developed cardiomegaly on chest radiography, and so on.
Statistical analysis
Statistical analysis was performed using SPSS version 21 (SPSS Inc., Chicago, IL, USA). Baseline characteristics are expressed as mean ± standard deviation (SD) for continuous variables and as frequencies with percentages for categorical variables. Continuous variables were compared using Student's t tests, and categorical variables were compared using χ2 test or Fisher's exact tests. Comparisons of the primary and secondary endpoints between two groups were analyzed by χ2 test or Fisher's exact tests. A logistic regression analysis was conducted to identify potential predictors for lead complications. All variables with P values < 0.10 in univariate analysis were subjected to multivariate analysis. A P value < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the institutional review board of the Asan Medical Center (IRB approval number; S2014-1463-0002). Requirement of informed consent was waived because de-identified information was retrieved retrospectively and the research involved no more than minimal risk to the participants.
RESULTS
Baseline characteristics
A total of 482 patients (mean age, 66.6 ± 12.9 years; 209 men [43.4%]) were enrolled. Baseline characteristics of the study patients according to the type of pacing lead are summarized in Table 1. Procedure time was significantly longer when using the 5086 lead than that for the 5076 lead. The procedure time (113.4 ± 43.4 minutes) for the 5086 lead was still longer than that (99.6 ± 46.5 minutes) for the 5076 lead (P = 0.003) after excluding two patients (mean time = 183 minutes) who developed cardiac tamponade during procedure.
Table 1
Baseline characteristics of the study patients
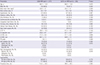
Data are expressed as mean ± SD or as a number (percentage or interquartile).
LA, left atrium; LV EDD, left ventricle end-diastolic dimension; LV ESD, left ventricle end-systolic dimension; LV EF, left ventricle ejection fraction; MRI, magnetic resonance imaging; RA, right atrium; RAA, right atrial appendage; RV, right ventricle; RVA, right ventricular apex; TR, tricuspid regurgitation.
Endpoints
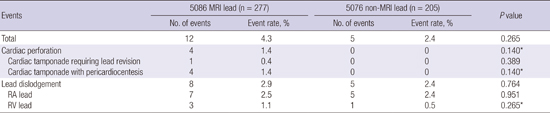
Four patients (0.8%) showed evidence of cardiac perforation as pericardial effusion with cardiac tamponade, necessitating only pericardiocentesis in 3 patients, and both pericardiocentesis and lead revision in one patient (Table 2). There was no one who showed a radiographic evidence of excursion of the pacing lead into the pericardial sac. All patients with cardiac perforation received the 5086 lead. Mean age of patients with cardiac perforation was 84 ± 3.5 years. Fellow trainee operated procedure in 122 cases (59.5%) of 5076 lead and in 193 cases (69.7%) of 5086 lead. In four cases of cardiac perforation, three patients were operated by fellow trainee and one patient by staff.
Table 2
Comparisons of cardiac perforation and lead dislodgement in the first 30 days between 5086 MRI lead and 5076 non-MRI lead
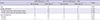
Characteristics of patients with cardiac perforation were described in Table 3. Two cases of cardiac perforation developed during the procedure of device implantation, and received pericardiocentesis promptly. One of them underwent lead revision the next day. One patient showed evidence of cardiac perforation on the day after device implantation. Cardiac perforation in the last patient was found two days after implantation. Any patient with cardiac perforation did not receive either antiplatelet or anticoagulant earlier.
Table 3
Characteristics of patients with cardiac perforation

Lead dislodgement developed in 13 (2.7%) of all patients with device implantation. The incidence of lead dislodgement was not significantly different between the 5086 and 5076 leads (Table 2). The incidence of lead dislodgment by fellow trainee was similar between 5076 lead (5 cases, 4.0%) and 5086 lead (8 cases, 4.1%). The right atrial (RA) lead dislodged in 10 patients, the right ventricular (RV) lead in 1, and both RA and RV leads in 2. Almost all (11 patients) dislodgement was noticed within 24 hours of implantation. In the remaining two cases, dislodgement was noticed on post-implantation day 3 and 4. All patients with lead dislodgement underwent lead revision. The rate of lead revision within 30 days of implantation was not significantly different between the 5086 (9 patients [3.2%]) and 5076 leads (5 patients [2.4%]) (P = 0.601).
Predictors for lead complications
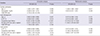
We performed logistic regression analysis to identify significant predictors of lead complications (Table 4). Age was only significant predictor for cardiac perforation in multivariate analysis. Congestive heart failure and implantation of RA lead at RA free wall or septum were significant predictors of lead dislodgement and lead revision. Left ventricular ejection fraction was significantly different between the patients with lead dislodgement and those without (lead dislodgement: 53.3% ± 10.2% vs. no lead dislodgement: 60.7% ± 10.2%, P = 0.011). However, left ventricular systolic function was not significant predictor for lead dislodgement after adjusting congestive heart failure. The 5086 lead was not associated with lead complications.
Table 4
Univariate and multivariate logistic regression analysis for the incidence of cardiac perforation, lead dislodgement, and lead revision in the first 30 days after pacemaker implantation
DISCUSSION
We compared the incidence of acute complications related to pacemaker lead between the 5086 and 5076 leads. The major findings of the present study are as follows: 1) all cardiac perforation occurred when using the 5086 lead (4 patients, 1.4%), but there was no statistically significant difference with the 5076 lead; 2) the incidences of lead dislodgement (2.9% vs. 2.4%, P = 0.764) and lead revision (3.2% vs. 2.4%, P = 0.601) were not significantly different between the 5086 and 5076 leads; 3) age was only significant predictor of cardiac perforation, and congestive heart failure and implantation of RA lead at the outside of RA appendage were significant predictors of lead dislodgement and revision.
Lead dislodgement and cardiac perforation/pericardial effusion were most common lead related complications of pacemaker implantation. The published incidence of lead dislodgement varies from 0.5% to 4.0% (1213141516). Atrial lead dislodgement is more common than ventricular lead dislodgement. The incidence of cardiac perforation and/or pericardial effusion after pacemaker implantation is reported between 0.5% and 2.0%, but nowadays it is usually lower than 1% (1718192021). In the present study, the incidence of lead dislodgement and cardiac perforation was 2.7% and 0.8%, respectively, which was consistent with previous results.
The rates of cardiac perforation (1.4%) and lead dislodgement (2.9%) using the 5086 lead in our study were consistent with those in previous two large prospective randomized studies using the 5086 lead. In EnRhythm MRI study, cardiac perforation and/or pericardial effusion developed in 5 of 467 patients (1.0%), and lead dislodgement occurred in 17 of 467 patients (3.6%) (4). In the Advisa MRI study, the number patients with cardiac perforation and/or pericardial effusion and lead dislodgement was 5 (1.9%) and 11 (4.1%) out of total 266 patients, respectively (10). However, recent two studies reported that the incidence of cardiac perforation and/or pericardial effusion, and lead dislodgement was significantly higher with the 5086 lead. Elmouchi et al. (6) reported that 5 (7.7%) of 65 patients developed cardiac perforation and/or pericardial effusion, and 4 (6.2%) patients showed lead dislodgement. Acha et al. (8) showed that there were 4 (5.5%) cases of cardiac perforation and 2 (2.8%) of lead dislodgement among the 72 patients. The reason for these different results is not clear, but might be explained by the differences of study populations, implant techniques, and learning curve period of the 5086 lead between the centers.
The two abovementioned studies showed that the incidence of cardiac perforation and/or pericardial effusion was significantly higher with the 5086 lead than that with the previous 5076 lead (68). In the present study, all cardiac perforation was developed using the 5086 lead, but there was no statistical difference with the 5076 lead. On the other hand, a recent retrospective cohort analysis revealed that a cardiac perforation was similar between the 5086 (0.6%) and the 5076 (0.6%) leads; however, there were more lead dislodgements in the 5086 lead (2.6%) than in the 5076 lead (0.6%) (P = 0.054) over the first 30 days (7). Moreover, there was a discrepancy in the difference in cardiac perforation between the 5086 and 5076 leads, in that the 5086 lead may have greater risk of cardiac perforation than the 5076 lead. The 5086 lead was generated from multiple system design modifications of the previous 5076 lead. These modifications include decreasing the number of lead filars, increasing the filar diameter, and increasing the thickness of the inner coil with its number of turns (4). As a result of these modifications, 5086 lead is stiffer and heavier with a larger outer lead diameter (2.3 mm vs. 2.0 mm) and has unusual horizontal pitch of the bipolar conductor compared to that of the 5076 lead. Consequently, the 5086 lead has been required to increase the maximum number of helix rotations for atrial and ventricular lead implantation (10). The increased stiffness and the heaviness of the 5086 lead were suggested as a possibly responsible for the increased cardiac perforation (6).
The predictors of cardiac perforation have not been well defined. Previous studies reported female sex, active fixation leads, use of temporary pacemaker, steroids as significant predictors of cardiac perforation and/or pericardial effusion (16171921). However, the present study revealed that old age is the only significant predictor of cardiac perforation. The influence of aging on acute complication is debated. Old age was reported to be associated with an increased incidence of pneumothorax (12). However, large cohort studies did not show a relation between age and acute complications (2223). In addition, congestive heart failure and implantation of RA lead at the areas (free wall or septum) other than the RA appendage are significant predictors of lead dislodgement and revision. Therefore, careful attention for cardiac perforation and/or lead dislodgement is required regardless of type of pacemaker lead when performing this procedure in old patients with congestive heart failure.
The management of cardiac perforation and/or pericardial effusion includes close monitoring, pericardiocentesis, lead revision, and surgery. Surgery requirement has been reported between 0% and 75% (1718192021). However, Laborderie et al. (20) reported that perforated leads can safely be removed under fluoroscopic guidance, with surgical backup support and close monitoring. In the present study, no patient required surgical intervention, but all patients received percutaneous pericardial drainage, and one patient required lead revision. Therefore, if pericardial effusion shows tamponade physiology, pericardiocentesis can be preferred over surgical intervention. In addition, if capture and sensing values of perforated leads are stable, close monitoring also can be preferred over lead revision or surgery.
The present study was a retrospective multicenter observational, and thus, had inherent limitations. Especially, the implant period was different between the 5086 and 5076 leads because the 5086 lead was introduced into the market more recently. All physicians had years of experience implanting the previous 5076 lead, and thus, might have experienced a learning curve with the handling of the new 5086 lead. However, cardiac perforation and lead dislodgement rates were spread out through the study period. Even the present study had numerous limitations, such as lack of data on the incidence of acute complications including lead dislodgement and cardiac perforation with the 5086 and 5076 leads in an Asian population.
In conclusion, the incidence of cardiac perforation and lead dislodgement within 30 days after pacemaker implantation were not statistically different between the 5086 and 5076 leads. However, because all cardiac perforation occurred when using the 5086 lead, meticulous attention is required when using the 5086 lead, especially in elderly patients.
 XML Download
XML Download