

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Stroke occurs in approximately 15 million people every year throughout the world, 5 million of whom die and 5 million of whom live with a permanent disability (1). In the United States, 795,000 stroke patients are newly diagnosed each year, and according to a survey in 2009, 1 in 19 people died due to stroke (2). In Korea, mortality from cerebrovascular disease in 2013 was 50.3 per 100,000 population, which was lower compared with 51.1 per 100,000 in 2012, but it still accounted for the second most common cause of death after cancer.
Treatment guidelines for stroke patients recommend administration of recombinant tissue plasminogen activator (rtPA) within a therapeutic time window and direct transportation to a specialized stroke center (345). However, the therapeutic rate of cerebral infarct patients is only 1.6% to 18%. Prehospital delay is a major factor associated with a low therapeutic rate (678910). In previous studies, patients who arrived at the hospital within a therapeutic window of time more frequently arrived by ambulance (11). It has been reported that the rate of treatment with rtPA increased from 10% for patients with standard priority to 24% for patients who were transported directly to a specialized stroke center with level 1 priority care (12). Several studies of inter-hospital transfer of stroke patients demonstrated factors associated with prehospital delay, such as specialized neuroimaging at the referring hospital (131415). Emergency medical service (EMS) use and inter-hospital transfer are important factors in prehospital delay, although with opposite direction of association, in ischemic stroke patients. In-depth studies of the interactive effect of EMS use and inter-hospital transfer are rare, and we found no studies considering whether patients were transferred to the referred hospital via EMS.
We analyzed the effects of EMS use on prehospital delay, including tracking the mode of transport to the referred hospital. Interaction between visit routes (direct visit or transferred from another hospital) and EMS use on prehospital delay was also analyzed using a nationwide, multicenter registry.
MATERIALS AND METHODS
Study setting
The EMS is a public transportation system operated by a single call number, 1-1-9, and provides services for free to anyone in Korea. They offer single-tiered basic life support service (16). The 1-1-9 prehospital emergency care protocols for presumed stroke patients were established in 2012 by the National Emergency Management Agency. These protocols included a prehospital stroke screening tool and direct transport to hospitals that had the capacity to manage ischemic stroke, including intravenous thrombolysis. Administration of intravenous thrombolysis before hospital arrival is not allowed in Korea (17).
The Ministry of Health and Welfare in Korea has created programs for developing regional centers for cardiovascular disease and successfully established 11 regional cardiovascular centers between 2008 and 2012.
Study subjects
The Cardiovascular Disease Surveillance (CAVAS) project was a nationwide prospective stroke registry sponsored by the Korea Centers for Disease Control and Prevention. The objectives of the program were to identify the epidemiologic patterns, including the risk factors, for cardiovascular disease and to collect data on the characteristics and quality of medical care before and after hospitalization for such patients. These data were collected from detailed hospital medical records of 29 emergency departments (EDs) across the country. During the study period (November 1, 2007, to December 31, 2012), patients diagnosed with acute stroke were enrolled. Ischemic stroke was diagnosed based on brain imaging and clinical assessment in the ED, and for final analysis, we included adult (age over 18 yr) ischemic stroke patients with ICD-10 code I63.0-I63.9 when they were discharged from the ED. Only patients who arrived at the first ED within 24 hr of onset were included (18). Patients were excluded if there was no information about the time of stroke onset or arrival at the final hospital, EMS use, and route of visit (direct or transferred). We also excluded patients who were administered thrombolysis before inter-hospital transfer.
Data collection and variables
Trained study coordinators collected basic information for each variable using a structured case report registry. The monthly data quality management process provided feedback to each participating hospital. For patient information, demographic data (age and sex), socioeconomic data (insurance status and level of urbanization), and clinical information (chief complaints at presentation and past medical history) were collected. Time data such as time of symptom onset and arrival at referred or final hospital were collected. Mode of visit (EMS use or not) and route of visit (direct or transferred) were also collected. We also presented death and neurologic outcomes at discharge. Neurologic outcomes were divided as favorable or poor according to the Modified Rankin Score (MRS). Favorable is equivalent to MRS 0 to 3, and poor is equivalent to MRS 4 to 6. The first medical contact time was defined as the time that the 1-1-9 call was accepted for patients who used EMS and the time that the patient arrived at the first or final hospital for patients who did not use EMS.
Patients were categorized into 4 groups according to EMS use and inter-hospital transfer: directly transported to the final ED by EMS (EMS direct), transferred to the final ED after being transported to a referred hospital by EMS (EMS indirect), directly visited final ED without using EMS (non-EMS direct), and transferred to final ED after visit to referred hospital without using EMS (non-EMS indirect).
Outcomes
Our primary outcome was symptom onset (S) to definitive care hospital (D) within 2 hr (S2D ≤2 hr), and our secondary outcome was symptom onset to definitive care hospital within 1 hr (S2D ≤1 hr). Symptom onset time was defined as the time of symptom recognition or the last time that the patient felt normal. The American Heart Association/American College of Cardiology guidelines for the treatment of ischemic stroke recommend intravenous thrombolysis for patients who arrive at the hospital within 3 hr of symptom onset and for this treatment to be administered within 90 min of arrival at the hospital (19). We chose our outcome variables based on practical considerations and recommended guidelines.
Statistical analysis
The continuous variables, including times, are presented as medians with interquartile ranges and were compared using the Kruskal-Wallis or Wilcoxon rank-sum test. The categorical variables are presented as numbers with proportions and were compared using the chi-square test. A multivariate logistic regression analysis was carried out between the 4 patient groups and S2D ≤2 hr. We considered demographic variables, socioeconomic variables, past medical history, and chief complaints at arrival as covariates. We also calculated adjusted odds ratios (AORs) and 95% confidence intervals (95% CIs) with the same covariates and S2D ≤1 hr. A P value <0.05 was defined as statistically significant.
RESULTS
Of 31,443 adult ischemic stroke patients, 9,002 patients were excluded because their symptom onset to hospital arrival time was over 24 hr. The 836 patients with unknown symptom onset to hospital arrival time were also excluded as were patients whose information about EMS use or route of visit was not recorded. In addition, 302 patients with thrombolysis before transfer were excluded. Therefore, 20,780 patients were included in the final analysis. Only 34% (7,011) had used the EMS; 26.9% (5,595) underwent inter-hospital transfer, and among the transferred patients, 13.5% (754) were transported via EMS to a referred hospital (Fig. 1).
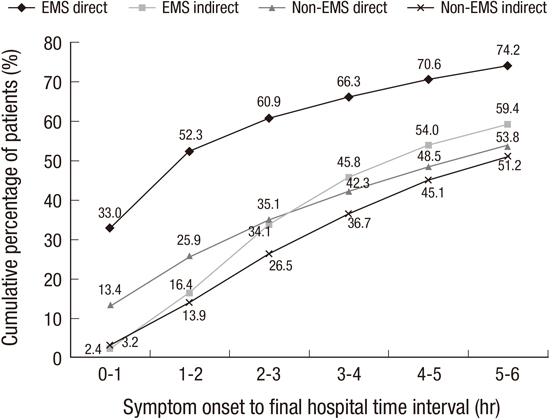
Table 1 shows the characteristics of the patients in the study. A majority of patients (63.3%) were over 65 yr old, and 41.5% were women. The highest proportion of patients (61.5%) presented with motor weakness as their primary symptom. In the S2D ≤2 hr group, the highest proportion of patients presented with unconsciousness (42.5%). In the EMS direct group, 52.3% of patients arrived within 2 hr, whereas in the non-EMS direct, EMS indirect, and non-EMS indirect groups, only 25.9%, 16.4%, and 13.9%, respectively, arrived within 2 hr (Fig. 2).
The patients who used EMS were significantly older than those who did not. The symptoms at presentation also differed significantly among the 4 groups; in particular, there was a higher proportion presenting with unconsciousness in the EMS group, especially in the EMS indirect group (36.2% vs. 24.5% in the EMS direct group, 19.1% in the non-EMS indirect group, and 7.2% in the non-EMS direct group) (Table 2).
Multivariate analysis was conducted between the 4 groups and S2D ≤2 hr and S2D ≤1 hr (Tables 3 and 4). The adjusted covariates for multivariate logistic regression were the variables that showed significant differences among the 4 groups (P<0.01). AORs (95% CIs) for arrival within the therapeutic time window (S2D ≤2 hr and S2D ≤1 hr) were 6.56 (5.94-7.24) for the EMS direct group compared with the non-EMS indirect group (reference). AORs (95% CIs) for S2D ≤2 hr were 1.07 (0.87-1.33) for the EMS indirect group and 2.27 (2.06-2.50) for the non-EMS direct group (Table 3).
DISCUSSION
This was a multicenter nationwide prospective study to characterize in detail ischemic stroke patients who arrive at the final hospital within the therapeutic time window according to visit mode and route of visit. Only 40% of patients in Korea arrived at the final hospital within 2 hr of symptom onset. EMS use was associated with arrival within the time window, but inter-hospital transfer showed a negative effect. Specifically, even with EMS use, the proportion of transferred patients who arrived at the final hospital within 2 hr was approximately 16%.
After analyzing data from the Get With the Guidelines-Stroke database, a data-collecting system including 905 hospitals in the United States, Saver et al. (11) reported in 2010 that 60% of direct visit patients arrived at the hospital within 3 hr of onset and 28% arrived within 1 hr, which is higher than what we found in our study. In our study, the proportion of direct visit patients in the S2D≤2 hr group was 40.0% (8,319) regardless of EMS use. Differences in the rate of EMS use may explain the difference. In our study, only 33.7% (7,011) of the study subjects activated the EMS, which is lower than the 47.6% in the Paul Coverdell National Acute Stroke Registry Surveillance covering 4 states from 2005 to 2007 in the United States (20) and other countries (21222324). In a previous nationwide survey about stroke awareness in Korea, only 33% had some knowledge of the proper action (to call EMS) (25). Also, time intervals from symptom onset to a call for EMS were significantly different between patients who arrived within 2 hr or not. Therefore, we need to adopt a new strategy to educate the public in recognition of symptoms suggestive of stroke and early medical contact.
The cumulative percentage of patients who arrived within 2 hr after symptom onset was highest in the groups who used EMS and were directly transported to the destination hospital. However, slightly higher proportions of patients in the non-EMS direct group arrived within 2 hr compared with those in the EMS indirect group (25.9% vs. 16.4%; Table 2). Approximately 23% of patients who did not use EMS arrived at the final hospital via other hospitals, but only 3.6% of those who used EMS arrived via other hospitals. This result suggests that even when patients recognize symptoms early, there is a greater chance of choosing the wrong hospital if the patient decides to not use EMS. Thus, using EMS if someone has symptoms suggestive of stroke should be emphasized in public education.
In the transferred groups, only 16.4% (EMS group) and 13.9% (non-EMS group) of the patients arrived at the final ED within 2 hr after onset (Fig. 2). Delivering the acute ischemic stroke patient to a comprehensive stroke center is important to increase the rate of intravenous rtPA administration. Symptom onset to definitive care after the treatment window due to transfer delay is also a common cause of exclusion for intra-arterial thrombolysis (26). For direct transportation to a comprehensive stroke center, EMS providers should be trained to screen for presumed stroke in the field. Prehospital stroke screening (PHSS) tools have been developed and are widely used in many EMS agencies in developed countries (272829). In Korea, results of a study to validate the PHSS performed by 1-1-9 EMS providers were comparable with previous studies (30). Another consideration to encourage direct transportation to a comprehensive stroke center is that information for a hospital's capacity for thrombolysis for ischemic stroke patients should be provided to EMS providers. Through an emergency information center in Korea, real-time monitoring of the thrombolysis capacity of emergency centers is available to citizens via the internet (30). Improving the quality of this information and encouraging active use of this information by EMS providers might increase the rate of direct transportation to comprehensive stroke centers.
Inter-hospital transportation is sometimes unavoidable, especially in geographically vulnerable areas, but efforts for reducing unnecessary delay during inter-hospital transport are essential for regionalization of the process of care for stroke patients. Several studies have focused on factors associated with delays during inter-hospital transfer of stroke patients (313233). Brain imaging studies, especially magnetic resonance imaging or perfusion computed tomography, at the referring hospitals were pointed out as one reason for delay. Regional cardiovascular centers established by the Ministry of Health and Welfare in Korea were comparable with comprehensive stroke centers in the United States, but primary stroke care centers that refer patients to comprehensive stroke centers have not been established in Korea. This weak point of regionalization in Korea is one possible explanation for our result that inter-hospital transfer attenuated the effects on arrival within the therapeutic time window through EMS use. For regionalization and reducing delay during inter-hospital transfer, a supporting program for referring hospitals, including development of a protocol for transfer and quality control, is needed.
Our study has several limitations. First, all hospitals in our study were academic teaching hospitals. The CAVAS program was an observational study that involved hospitals that volunteered to participate in the program, and these tended to be larger and more specialized than nonparticipating hospitals. Second, our analysis did not include the severity of the strokes at presentation, for example, as assessed by the National Institutes of Health Stroke Scale (NIHSS), because this was not recorded in the CAVAS registry. Severity of symptoms is one of the factors associated with prehospital delay and an important determinant of EMS use (34353637). Instead of NIHSS, we used symptoms at arrival such as loss of consciousness and motor weakness as surrogates of severity for adjustment in multivariate logistic regression (Tables 3 and 4).
In conclusion, the patients who are directly transported to the destination hospitals by the EMS show the highest proportion of arriving within the therapeutic time window for optimal care for ischemic stroke. Owing to the time-dependent properties of stroke treatment, a system of stroke care comprising the community, the EMS, and hospitals should be strengthened.





 XML Download
XML Download