

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Tobacco use is increasing in the world, and the health effects of secondhand smoke (SHS) are a public health issue. Exposure to SHS is associated with respiratory disease, cardiovascular disease, and cancer (12). SHS caused 603,000 deaths and 10.9 million disability-adjusted life years (DALYs) worldwide, corresponding to 1.0% of all deaths and 0.7% of the worldwide burden of disease in DALYs (3).
Controlling tobacco and SHS prevalence is an important global public health challenge. In response to this issue, many countries are actively implementing a smoking ban policy in public and workplaces. However, exposure to SHS remains unacceptably high. In Korea, 36.1% of non-smokers are exposed to environmental tobacco smoke at work or at home (4).To address this problem, clarification of factors contributing to SHS exposure is important. While the socioeconomic and psychosocial determinants of smoking have been extensively researched, studies focusing on SHS determinants are lacking. Suggested factors related to SHS exposure include cultural and sex differences, socioeconomic factors, and health risk behaviors (567). Lower socioeconomic status (SES) increases the risk of SHS exposure (48910).
However, factors contributing to SHS exposure in Korea are unclear. Active smoking is a voluntary behavior; however, exposure to SHS occurs passively and can affect nonsmokers. Therefore, specific contextual factors contributing to nonsmoker exposure to SHS depend on location and geographical region. To determine the factors affecting SHS, analyses conducted in different SHS exposure locations and at regional levels are needed. Understanding the contextual factors of SHS with respect to these parameters can help in the development of effective smoke-free policies in specific locations and areas. However, such studies are limited. Some studies have examined the home or workplace, with public spaces relatively neglected. Additionally, comparison of these three locations has not been widely performed. A study in Bangladesh indicated that the SHS exposure levels at home, in the workplace, and in public places vary markedly across socioeconomic and demographic subgroups (11). In the United States, a county-level study was conducted to account for individual and county-level differences of exposure to SHS in the workplace (12). However, to our knowledge, no studies have assessed the associations between these variables and SHS exposure based on different locations in Korea.
The present study was conducted to identify regional and individual factors contributing to SHS exposure according to location and gender and to identify variables most strongly associated with SHS exposure at each location.
MATERIALS AND METHODS
Data source and study population
Data in this study were obtained from the 2013 Korean Community Health Survey (KCHS) (13), the report of Development of Health Indicators for Community Health Ranking (DICR) (14), and the Korea No Smoking Guide website (15). This website introduces smoke-free policies and anti-smoking programs. It provides a wide variety of information on smoking in order to prevent and control smoking.
The KCHS was a nationwide survey that collected data from 253 local communities including 228,781 adults ≥ 19 years of age. The community health indicator study used a theoretically and empirically supported community health model. Health factors were measured in five domains of health behaviors including clinical care, social and economic factors, physical environment, and health policies. Both studies examined 253 communities, with Sejong city exempt from the community health indicator study and Yeongi county from the KCHS.
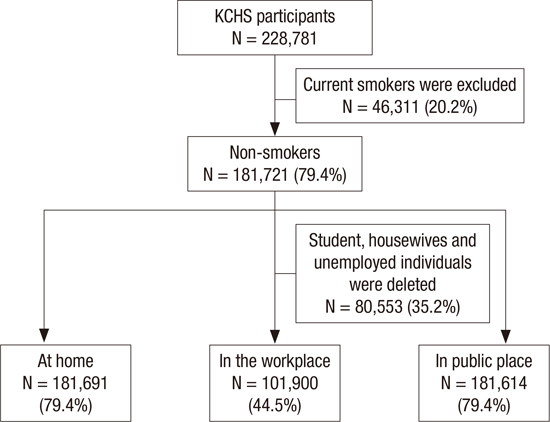
The 2013 KCHS included 228,781 adults ≥ 19 years of age who completed the interviews. Even though SHS is effective on both smokers and non-smokers, we assumed the effect on non-smoker is more harmful and important in public health, we only included non-smoker in our analysis. Among the participants, 46,311 (20.2%) active smokers were removed from the data in the present study. Finally, 181,721 (79.4%) non-smokers (including never smokers and ex-smokers) were used for analysis. Moreover, regarding SHS exposure in the workplaces, the data of students, housewives, and unemployed individuals (80,553, 35.2%) were excluded from the present study (Fig. 1).

Dependent variables
Dependent variables were SHS exposure at home, in the workplace, and in public places. Participants were asked questions regarding SHS exposure (hours per day) in these three locations. The questions were: “How many hours in a day exposure to SHS at home?”, “How many hours in a day exposure to SHS in work place?”, and “In recent 12 months, do you have exposure to SHS in public place?” The answers were recoded to yes (if participants were exposed) or no (if participants were not exposed, in other words, 0 hours exposure).
Independent variables
In previous studies, SHS exposure was analyzed in terms of socioeconomic factors including education, household income, employment, health-related factors, and place of exposure (567). In comparison to previous studies conducted in Korea (410), we selected home, workplace, and public place as SHS exposure locations and constructed a common individual variable model to evaluate SHS exposure in the three location types. The model assessed smoking status, individual socioeconomic differences (education, household income, location of residence), and health-related characteristics. In the location-specific model, housing and family type were used to estimate SHS exposure at home, and employment and occupation were used to estimate SHS exposure in the work place. Regional variables including health behavior and socioeconomic and health policy dimensions were evaluated for relationship with SHS exposure in public places.
A smoking status dummy was created with a score of 1 for never smoking and 2 for smoking. Average monthly household income variables were converted into a quartile index (scale 1–4, where 4 = above the third quartile). Locations of the residence dummy were scored as 1 for rural and 2 for urban. To assess the health status dimension, dummies of drinking and physical activity were used (1 for no and 2 for yes, respectively). Housing type dummies were constructed for detached house apartment, row house, multiplex house, commercial building house, and other dwelling types. Nineteen family type dummies were reconstructed into10 types (Table 1).
Table 1
Characteristics of the participants in 2013

![]()
Occupation dummies were constructed for officials or managers, professionals, service workers, sales people, skilled agricultural/forestry/fishery workers, craft and trade workers, plant or machine operators and assemblers, manual laborers, and professional soldiers. Employment dummies were constructed for employer or owner-operator, paid worker, and unpaid family worker.
Regional data collected in the DICR and included health behaviors (prevalence of active smoking, drinking rate, cancer screening rate) and socioeconomic characteristics such as high school graduation rate, unemployment rate, household income, and proportion of families with single parents or grandparents. Health policy data included health budget, financial autonomy, and smoke-free ordinance implementation. Smoke-free ordinance implementation in each region was obtained from Korea No Smoking Guide website. No ordinance implementing regions were categorized as 0, the regions with smoke-free ordinances implementation before December 31, 2011, between January 1 to December 31 in 2012, and between January 1 to December 31 in 2013, were categorized as 3, 2, 1, respectively. The definitions and units of regional variables are shown in Table 2. All regional variables were converted into a quartile index.
Table 2
The definitions and distribution of regional variables

![]()
Statistical analyses
Descriptive analyses and multivariate regression analysis models were used. Logistic regression analysis was applied to estimate the relationships between common individual variables and SHS exposure in the three locations and to analyze the special variables of exposure to SHS at home and in the workplace. Multilevel analysis was used to detect factors affecting SHS exposure in public places because multilevel analysis is a suitable approach to take into account the social contexts as well as the individual factors in one model. Multilevel analysis allows several levels of analysis to be accounted for simultaneously and more effectively than in conventional multivariate analysis (16). The importance of a multilevel statistical approach for social epidemiology is discussed in other previous articles (17).
In multilevel analysis, individual characteristics, such as social and demographic factors (age, education, household income yearly, location of residence), Health-related factors (smoking status, drinking, physical activity) were set as the first level, and regional characteristics (Health behavior factors, Socioeconomic status, and Health policy dimensions) as the second level.
The associations between variables and SHS exposure were expressed in terms of odds ratio (OR) and 95% confidence interval (CI). All statistical significance decisions were based on two-tailed p-values. All analyses excluded observations with missing information and were conducted using SAS software version 9.4 (SAS Institute, Cary, NC, USA). To account for differential probabilities of selection, sampling weight was calculated for each respondent. These weights were used in the analysis to ensure regional representation. Cronbach's alpha was used to test the consistency in SHS exposure in the home/workplace/public locations.
RESULTS
Variable characteristics
Characteristics of participants in 2013 are presented in Table 1, and χ
2 tests of all variables were statistically significant. Among the participants (non-smokers including never smokers and ex-smokers in 2013) 60,051 (26.2%) were male and 121,670 (53.2%) were female.
Cronbach's alpha coefficient for SHS exposure in the three different locations was 0.223, indicating inconsistency in SHS exposure in the three locations (data not shown). Prevalence of SHS ranged from 1.8% to 20.6% at home, 3.1% to 36.7% in the workplace, and 21.6% to 96.8% in public places.
Results of SHS exposure at home, in the workplace, and in public places based on sex
Multivariate analysis results were shown in Table 3, 4, and 5. Univariate analysis results showed no meaningful difference from multivariate analysis, only multivariate analysis results were shown in this article. In all three locals, younger age, drinking, and physical activity were positively associated with SHS exposure both in male and female non-smokers separately.
Table 3
OR and 95% CI of logistic regression analysis of SHS exposure at home

OR, odds ratio; 95% CI, 95% confidence interval; SHS, secondhand smoke.
*
P value less than 0.05; †
P value less than 0.01.
![]()
Table 4
OR and 95% CI of logistic regression analysis of SHS exposure in the work place

OR, odds ratio; 95% CI, 95% confidence interval; SHS, secondhand smoke.
*
P value less than 0.05; †
P value less than 0.01.
![]()
Table 5
OR and 95% CI of multilevel regression analysis of SHS exposure in a public place

OR, odds ratio; 95% CI, 95% confidence interval; SHS, secondhand smoke; SE: standard error.
*
P value less than 0.05; †
P value less than 0.01.
![]()
At home, male never-smokers were more likely to be exposed to SHS than ex-smokers while females showed opposite relation. High educational level in males and females was negatively associated with SHS exposure, and middle-level household income in females was positively related with SHS exposure. The results of home-related variables adjusted for common individual variables showed that single father and unmarried children family types were significantly associated with SHS exposure at home in males and females. Commercial building type of housing was positively associated with home SHS exposure, while apartment type was negatively associated.
In the workplace, living in an urban area, household income in males, and education in females were positively associated with SHS exposure, while only female ex-smokers had a positive relation with SHS exposure. In work-related factors, male paid workers demonstrated a positive association with SHS exposure, while female paid workers had a negative relation. Sales and service workers, blue-collar workers, and manual laborers were most significantly associated with SHS exposure in males and females.
In public places, living in an urban area, high educational level, and high income showed a positive relationship with SHS exposure in males and females. Male ex-smokers showed a positive relationship with SHS exposure. The model results indicated that drinking rate was positively associated with SHS exposure among male and female non-smokers, and cancer screening rate and single-parent family were positively associated with SHS exposure only in females. Year of smoke-free ordinance implementation did not show any significant relationship with SHS exposure.
DISCUSSION
SHS exposure has been linked to cultural and socioeconomic factors, as well as health risk behaviors (567). Our results regarding common individual variables indicate that exposure to SHS is associated also with socioeconomic status, with variations according to location. We observed substantial differences on SHS prevalence ranged from 1.8% to 20.6% at home, 3.1% to 36.7% in the workplace, and 21.6% to 96.8% in the public place. This means that the SHS effects on individuals are not homogeneous in each region. SHS is non-voluntary behavior and dependent on its contextual environments. Therefore, we included regional variables in this analysis and used more sophisticated analysis, multilevel analysis to consider regional effects at the same time.
In all three types of location, a trend of lower exposure with increasing age was observed in males and females. High SHS exposure among younger adults was previously reported in the United States, Canada, and some European countries (41819). The smoking prevalence is reportedly higher in young Koreans than for the older population (20). Additionally, social environment has been linked to SHS behaviors in young Koreans. Young adults are likely to spend more time in smoky pubs and restaurants (21). Koreans are traditionally brought up to show respect for their parents, older persons, and persons of higher status (22); therefore, expressing a desire to avoid contact with a smoker is considered impolite or rude. As a result, young people are possibly more tolerant of smoking in all locations. This was also observed in a previous study in Korea (23).
Regarding drinking behavior, a positive association was found with SHS exposure in the three locations. In traditional Korean culture, smoking and drinking are considered normal means of facilitating social relationships (24). In addition, physical activity showed a positive association with SHS exposure in the three locations. People who participate in physical activity appear to have more opportunities to be exposed to SHS. Non-smokers might exercise or participate in a physical activity with their partners who are smokers, which could expose them to SHS.
At home, education was negatively associated with SHS exposure in males and females, indicating that people with a high educational level are less exposed to SHS. In general, highly educated males are rarely smokers. Additionally, it might be that females with a husband or boyfriend having a high educational level are rarely exposed to SHS at home.
We found that male ex-smokers were negatively associated with SHS exposure, but female ex-smokers showed a positive association. Exposure to SHS has been reported for ex-smokers in Korea and elsewhere (4182526). However, these previous studies did not estimate this variable based on exposure location. To the best of our knowledge, active smoking prevalence is higher among males than females, and most smokers are male. It is likely that, once the male in the household quits smoking, no smoker will remain in the family. For females, although they may quit smoking, their husband or boyfriend may be a smoker, creating a greater risk of exposure to SHS at home.
In home-related variables, our results showed that a single father with unmarried children had a strong positive association with SHS exposure at home in males and females. Usually, this type of family is most likely a broken family or has a low household income. Especially in a single-father family, the father’s smoking behavior is not regulated by a spouse, which may result in increased SHS exposure for the children. Paternal educational level was reportedly a decisive factor of SHS exposure. Fathers with a low educational level tend to smoke relatively more in the presence of their children (10), and children living with a father who smokes are more than three times likely to start smoking (27).
Additionally, people living in a commercial building type of housing had higher SHS exposure among both male and female non-smokers than those living in other housing types. Households with a higher SES can afford to buy or rent larger houses or flats and are more likely to be nonsmokers. Bad housing locations, crowded living conditions, low quality of housing, and aging public facilities have been associated with high SHS exposure at home (2829), and our results are consistent with these findings. In addition, in Korea, the first and second floors in commercial building often house restaurants or bars, with people living above the businesses. People who live in this type of housing are more likely to be exposed to SHS.
In the workplace, our results showed a positive association between female ex-smokers and SHS exposure in the workplace, possibly because female ex-smokers work with other male or female colleagues who are current smokers, thus exposing them to SHS. In the work-related dimension, male paid workers demonstrated a positive relation with SHS in the workplace, while female paid workers showed a negative association. In Korea, male paid workers gather during breaks, and those who smoke may expose non-smokers to SHS. However, females might not smoke in the presence of their colleagues but smoke alone or only with other smokers.
Both male and female service workers, sale workers, blue-collar workers, and manual laborers showed a strong positive association with SHS exposure in the workplace. Service workers are mostly females and work in restaurants, coffee shops, and bistros, where nonsmokers experience the same level of exposure to SHS as do smokers (30). A previous article indicated that workers with lower social status are more likely to be exposed to SHS at work (3132), which is consistent with our results. Individuals who are engaged in skilled manual work, sales, service, and simple labor jobs have much higher rates of SHS exposure at work than do other professions (431), and blue-collar and service workers are more likely to be employed at work sites that permit smoking (33). Previous studies have found that, compared with other workers, blue-collar workers smoke more heavily and are less successful at quitting smoking (34). Interestingly, in females, the ORs of professional and service workers were relatively higher than those of sale workers, blue-collar workers, and manual laborers. Professional females usually have high socioeconomic status and position. Similar to female employers, professional females may be at greater risk of exposure to SHS due to various reasons such as business meetings with others who are smokers.
When studied with regard to public places, living in an urban area, high individual education, and high income had a positive association with SHS exposure both in males and females. People with higher educational and income levels might be more aware of and sensitive to SHS exposure and perceive exposure to SHS as a health hazard. Furthermore, in high socioeconomic development regions where population density is increased, people are crowded into narrow places and are potentially more exposed to SHS.
Heavy drinking rate both in males and females is associated with a higher risk of exposure to SHS in public places. It means that not only individual drinking behavior but also regional contextual factor regarding drinking are associated with SHS exposure. Therefore, to reduce nonsmoker exposure to SHS, it is important to control the contextual and cultural factors regarding drinking also.
Moreover, we observed that the proportion of single-parent families both in males and females had a positive relationship with SHS exposure in public places, indicating again that single-parent families play an important role not only on the individual level, but also on the regional level.
Our study shows that smoke-free ordinance has no significant relation with SHS prevalence in public place. It might be indicated that impact of smoking and SHS control policy are limited. A previous study in Korea indicated that the effects of regional smoke-free ordinances revealed clear difference in rate of current smoking among males (35). The result is inconsistent with ours may be because that, this previous study focused on active smoking prevalence only among males, while our study focused on SHS prevalence and research objects were nonsmokers (most were female). In addition, as our study results shows, other contextual factors played more important roles in affecting SHS exposure among nonsmokers.
In summary, people with similar socioeconomic characteristics tend to be significantly exposed to SHS in different locations and regions. The affecting factors differ according to location and gender plays a different role regarding SHS exposure suggesting different gender culture regarding smoking behavior.
The present study had several limitations. First, as the survey was conducted annually, regional differences at the time of survey implementation could affect SHS prevalence calculations. Second, previous studies have shown that individual factors related to SHS exposure such as a family member smoking, friends or peer smoking, parental knowledge of anti-SHS, SHS attitude, and avoidance behavior were significantly associated with SHS exposure (3637). Due to the limitation of this population-based survey, these factors could not be estimated; in addition, it is possible that some factors not be examined in the present study affect SHS exposure. We suggest that a qualitative study should be conducted with further exploration of factors affecting SHS exposure. Third, because each survey respondent had a different sensitivity to the SHS questionnaire, uneven recall bias might have occurred in the results.
Despite these limitations, our study is unique in several ways. Unlike previous studies, we focused on three exposure locations and indicated affecting factors in exposure to SHS based on location and gender. Furthermore, this study involved a substantial population sample and comprehensive data on several dimensions of socioeconomic position. Finally, this is the first study to assess contextual factors and SHS exposure in three types of location and on the regional level in Korea.
In conclusion, to implement effective policy strategies for reducing SHS exposure, the contextual factors of specific location and regional context should be considered. For example, not only should the ban on family smoking activities be actively advocated, but more SHS education and social support should be provided to single-father families. In dwellings with high SHS exposure, such as the densely populated commercial building type of housing, special supervision measures banning smoking should be implemented. In the workplace, a smoking ban could be linked to tax concessions, especially to small companies or family businesses. More social attention and enhanced anti-SHS education should be given to blue-collar and service workers. Social welfare and medical insurance treatment should also be improved. We recommend that special smoking regulations, surveillance, and legislation be established in public places, especially in places with high prevalence of smoking.
The SHS problem appears to be a social phenomenon. However, it embodies social policy and interactions between individuals and social contextual factors. Policy reforms and arduous and long-term efforts to improve contextual characteristics of SHS exposure in all locations are needed.
 XML Download
XML Download