

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chemical synthesis of penicillin in the 1950s led to the use of ampicillin, which was replaced by amoxicillin in 1974 with a higher and more prolonged serum concentration (1). All of the above are members of the same family of β-lactam antibiotics, which act by inhibiting the synthesis of cell wall of Gram-positive and of Gram-negative bacteria. Further members of this class include piperacillin, ticarcillin, and various others. Amoxicillin is frequently used for respiratory tract infections and is the first line treatment for middle ear infection. The common adverse drug reactions (ADR) of amoxicillin observed in clinical using were diarrhea, rash, vomiting, and nausea (2).
However, apart from the personal risks of ADR, there is much bigger influence on society due to the extensive use of antibiotics. The indiscriminate use of antibiotics has contributed to the occurrence of bacterial resistance, both in hospitals and in community settings (34). In a study conducted in Italy, 31% of H. pylori isolates were resistant to amoxicillin, resulting in only 17% cure rate (5). In Korea, prevalence of resistance in H. pylori isolates increased over time from 7.1% to 18.5% during 2003 to 2012 (6). In Japan, amoxicillin resistance rate for H. pylori was reported as 13.6% (7), and a study in Brazil reported that 29% of patients were harboring strains resistant to this antibiotic (8). Furthermore, a higher rate of antibiotic resistance was significantly correlated with higher consumption of antibiotics (91011). Korea is one of the countries with the highest antibiotic resistance rates, and ranked was the top seventh antibiotic-consuming country among 25 Organization for Economic Cooperation and Development (OECD) countries from 2005 to 2009 (1213). Even though Korea started the legislative separation of drug prescription and dispensing to reduce the misuse or overuse of antibiotics in 2000 (14), antibiotics are still commonly prescribed in real clinical setting.
The importance of post-marketing surveillance is emphasized because ADRs cannot be fully detected during the premarketing developing process. According to the World Health Organization (WHO), an ADR is defined as response to a drug that is noxious and unintended and occurs at doses normally used in man for prophylaxis, diagnosis, or therapy of disease or modification of physiological function. However, a signal is defined as reported information on a possible causal relationship between an adverse event (AE) and a drug, the relationship being unknown or incompletely documented, which is considered necessary to evaluate further. We used a data mining approach for detecting signals of amoxicillin in order to search for neglected or unknown ADRs using a nationwide AE database.
MATERIALS AND METHODS
Database and study drug
We mined reported cases related to amoxicillin from the Korea Adverse Event Reporting System (KAERS) database. The KAERS database was developed by the Korea Institute of Drug Safety and Risk Management (KIDS) to manage adverse event (AE) reports effectively in 2012. The AE Reporting System was first launched in 1988 by the Korea Food and Drug Administration (KFDA), and since then nationwide spontaneous AE reports have been collected. This computerized AE reporting system includes voluntary reporting by health care workers, general public, and mandatory reporting by manufacturers for serious and unexpected events using a standardized form. The names of the drugs were coded according to the Anatomical Therapeutic Chemical Classification System (ATC Code) and AEs were coded according to the Preferred Terms (PTs) among WHO Adverse Reaction Terminology (WHO-ART). A total of 807,582 reports were accumulated from December 1988 until June 2014 in the KAERS database. In the present study, we chose the amoxicillin as the study drug and all the other antibiotics as the comparison drugs.
Statistical analysis
Disproportionality analysis is regarded as a fundamental tool of analytic methods using for pharmacovigilance, which compares the proportion of occurring AEs between a specific study drug and all other drugs. When a specific drug is more likely to induce a specific AE than all other drugs, it would typically receive a higher score due to higher disproportionality (15).
Frequentist and Bayesian methods were used to calculate disproportionality by using proportional reporting ratio (PRR), reporting odds ratio (ROR), and information component (IC). For the frequentist approach, we can produce a 2x2 contingency table by defining as row with amoxicillin and all other antibiotics, column with Specific AE and all other AE. The PRR is the ratio of reporting rate of one specific AE among all events for a given drug, the comparator being this reporting rate for all drugs in the database including the drug of interest. We defined signals of PRR were at least 2, at least 4 chi-squared value and three or more cases (16). ROR is applied by the Netherlands Pharmacovigilance Centre, Lareb, while the PRR was first used by Evans et al. (17). We defined the ROR as the ratio of the odds of reporting one specific AE versus all other events for a given drug compared to this reporting odds for all other drugs in the database (18). A signal is considered when the lower limit of the 95% confidence interval (CI) of the ROR is greater than one (19). IC is the signal metric used in the Bayesian Confidence Propagation Neural Network (BCPNN) (20). If drug and event are statistically independent, the ratio of the joint probability of drug and event [P(AE,Drug)] to the product of the individual probabilities [P(AE)P(Drug)] will equal 1 and the IC will equal zero. The use of the logarithm of the ratio is derived from information theory. The AE which was detected by all the three indices PRR, ROR, and IC was defined as a signal in this study. The signals detected in the KAERS database were compared with drug label information of Korea and 8 other countries; USA, UK, Japan, Germany, Swiss, Italy, France, and Laos. All statistical analyses were performed by SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and Microsoft EXCEL 2010.
RESULTS
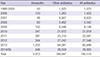
More than one AE can be included in one AE report of a specific drug reported by one case patient, therefore resulting in more than one drug-AE pair for each AE report. The total number of drug-AE pairs associated with amoxicillin was 2,913, while the total number of AE reports of amoxicillin was 1,722, and among 241 types of AEs resulting from amoxicillin, 52 met the criteria of a signal. Among 192,510 antibiotics-AE pairs in the KAERS database, the number of amoxicillin pair was 2,913 (1.5%) and 189,597 were pairs by all the other antibiotics from December 1988 to June 2014. It is clear that the total number of AE reports by antibiotics has increased year by year (Table 1). The characteristics of reports of amoxicillin are presented in Table 2. Among the 1,722 reports attributed to amoxicillin, 660 (38.3%) were from male, and 853 (49.5%) were from female. The most frequent report by type was spontaneous reports (647, 37.6%). The most frequent report source by person was doctors (505, 29.3%), and the most frequent report source by affiliation was regional pharmacovigilance center (1,009, 58.6%), followed by pharmaceutical companies (599, 34.8%).
Table 1
Number of AE reports by amoxicillin and other antibiotics from December 1988 to June 2014
![]()
Table 2
Characteristics of AE reports of amoxicillin from December 1988 to June 2014

![]()
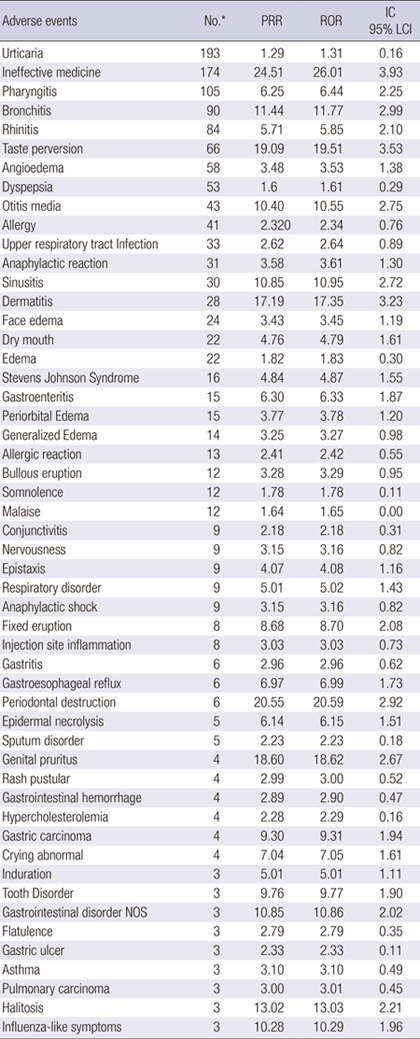
The frequent AEs associated with amoxicillin included rash, urticaria, ineffective medicine, diarrhea, pruritus, pharyngitis, and bronchitis (Table 3). The detected signals for amoxicillin by fulfilling the criteria for signal by three data mining indices were 52 AEs, among which the frequent AEs were urticaria, ineffective medicine, pharyngitis, bronchitis, rhinitis, taste perversion, angioedema, dyspepsia, otitis media, and allergy (Table 4). A total of 12 AEs including ineffective medicine, bronchitis, rhinitis, sinusitis, dry mouth, gastroesophageal reflux, hypercholesterolemia, gastric carcinoma, crying abnormal, induration, pulmonary carcinoma, and influenza-like symptoms were not listed on any of the drug labels of 9 countries (Table 5).
Table 3
Frequently reported AEs associated with amoxicillin

![]()
Table 4
Detected 52 signals of amoxicillin fulfilling the criteria for signal by three data mining indices

PRR, proportional reporting ratio; ROR, reporting odds ratio; IC, information component; NOS, not otherwise specified.
*Number of countries containing adverse events on drug labels among Korea, USA, UK, France, Italy, Japan, Switzerland, and Germany.
![]()
Table 5
Existence of the information of 52 detected signals on the drug labels of 9 countries

![]()
DISCUSSION
We identified 12 AEs as new signals associated with amoxicillin which were not listed on drug labels of 9 countries. Among them, ineffective medicine was the most frequent report, and one of the possible explanations for this might be due to partial adherence of patients for taking amoxicillin. Some patients may not follow the advice of medical professionals about the required duration needed to take the drug. Poor adherence to medication is known to induce substantial worsening of morbidity and mortality and increased financial costs (212223). In addition, poor medication adherence is a major cause of medication-related hospital admission from 33% to 69% (2425). It is clear that if patients adhere and follow the prescription of their doctors correctly, the result of treatment will be most effective (25). Therefore, it is important to educate and inform patients to keep high adherence to physician’s prescription.
Adverse events such as bronchitis, sinusitis and rhinitis are those of the indications of amoxicillin (26). This might be the result of being unaware of the indication of the medication from the patients. Sometimes patients use antibiotics incorrectly in terms of time, either early or later than their physician’s expected use. One previous study suggests that amoxicillin provides little symptomatic benefit for patients visiting primary care clinics for acute lower-respiratory-tract infection (27). Moreover, since H. pylori infection is a common chronic gastric infection in worldwide, H.pylori resistance for amoxicillin could be one of the reasons for treatment failures of amoxicillin (5). In line with the literature (28293031), it was found that chronic atrophic gastritis associated with H. pylori infection increases risk of gastric carcinoma. In case of hypercholesterolemia, some case report found H. pylori associated protein-losing hypertrophic gastropathy with hypercholesterolemia (32).
Even though the adverse events such as gastric carcinoma, abnormal crying, gastroesophageal reflux and pulmonary carcinoma are not listed in the drug label, the symptoms of these diseases do appear in the label. For example, in case of gastric carcinoma, its symptoms such as abdominal pain, vomiting, and bloody stool are indicated as the adverse effects of amoxicillin. Besides that, several symptoms of pulmonary carcinoma such as difficult breathing, coughing, and chest pain were included in the drug label of amoxicillin. Particularly, asthma is not labeled in Asian countries but is on all drug labels of western countries. This might explain the unknown ethnic effect of amoxicillin.
Differently from other countries in our study, Laos had fewer adverse effects listed on the drug label. This might be due to the absence of AE reporting system in Laos. Even though drug safety monitoring and evaluation was one of the thirteen elements of Lao National Drug Policy since 1992 (33), spontaneous AE reports have not been collected until now, and regulatory actions responding drug safety issues were passively done in response to other developed countries’ safety alert and communications. Drug safety monitoring including AE reporting and product surveillance is an essential component of safe drug use by the people in Laos, therefore sufficient budget should be provided to activate spontaneous AE reporting system in Laos like the one in Korea.
The most crucial limitation of this study derives from the fact that KAERS database is a result of spontaneous AE reporting system. AEs are usually underreported in any spontaneous AE reporting system in the world. The reporting rate can vary with the particular adverse event, but average is approximated about 6% (34). Since the knowledge and opinion of health professionals are significant determinants of spontaneous reporting (35), it is less likely for the unknown AEs to be reported. Under-reporting of AEs could reduce sensitivity because it underestimates the frequency and thereby the impact of a given ADR. Also, the absence of an unexposed control group, lack of information on denominator of a suspected drug exposure do not allow the quantification of risk and a definite association cannot be provided, which requires complementary post-marketing safety assessment method such as cohort or case-control study (36). Although data mining is being applied for detecting signals early and effectively for fulfilling the purpose of pharmacovigilance, early signals may be equivocal. Nevertheless, this study was the first attempt to detect amoxicillin signals using the KAERS database, a nationwide source of information for hypothesis generation in drug safety. Early detection of serious and unexpected signals is significantly meaningful in pharmacovigilance, which can help to protect people from the hazard of drugs.
In conclusion, we detected signals of amoxicillin and compared those information among the labels of 9 countries, and found that 12 AEs were not listed on the drug labels of any of the 9 countries. Therefore, it should be followed by signal evaluation including causal association, clinical significance and preventability.
 XML Download
XML Download