

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Steroids are powerful anti-inflammatory agents, and effectively reduce nerve root inflammation produced by disc herniation or a disc pathology near the epidural space. An initial observational study reported transforaminal epidural steroid injection (TFESI) offered a treatment option for radicular pain due to lumbar disc herniation and that it provided > 50% pain reduction in 75% of treated patients (12). A randomized prospective study also showed that TFESI had a success rate of 84% after a follow-up of 1.4 years (3).
Epidural steroid injections are widely and conventionally used to alleviate and control radicular pain effectively. However, sometimes, single and/or repeat steroid injections cause adverse effects, such as, spinal cord infarct, epidural fat hypertrophy, menstrual changes, and adrenal suppression (45). In particular, care should be taken to control blood sugar levels in patients with diabetes mellitus after an epidural steroid injection (6).
Radiofrequency (RF) treatment involves continuous stimulation and ablates nerves and tissues by increasing temperature around the RF needle tip (7), and thus, RF treatment involves nerve ablation. However, pulsed radiofrequency (PRF) uses a brief stimulation period followed by a long resting phase, which exposes target nerves and tissues to an electric field without producing sufficient heat to cause structural damage (89). Several studies have reported PRF stimulation modulates susceptibility to radicular pain without causing tissue damage, and observational studies on PRF application to dorsal root ganglia (DRGs) also concluded the technique appears both effective and relatively safe for the treatment of cervical and lumbar radicular pain (10). However, few systemic studies have been conducted to compare the effectiveness of PRF and TFESI for radicular pain. Because PRF procedure does not need require the injection of any material, it is certain to be free of the adverse effects associated with TFESI, and thus, offers the possibility of providing a method of treating radicular pain in a safer manner.
For these reasons the present randomized controlled study was aimed at determining the effectiveness of PRF for treating radicular pain due to disc herniation and comparing its outcomes with those of TFESI.
MATERIALS AND METHODS
Materials
During the period from March 2013 to February 2015, 193 patients were underwent TFESI for the treatment of spinal radicular pain. Patients received TFESI initially, which was conducted using 2 mL of 0.125% bupivacaine mixed with 5 mg dexamethasone. If, after first TFESI, patients still presented with a Visual Analogue Scale (VAS; 0-10 mm) of > 4 and an Oswestry Disability Index (ODI) or Neck Disability Index (NDI) of > 30%, then PRF and additional TFESI after initial TFESI were randomly allocated and conducted within from 2 to 6 weeks later after 1st TFESI (1011). Each procedure was conducted by the physician who had experience spine interventions over more than 25 years. Subjects with cervical and lumbar radicular pain was proved by physical examination and imaging studies corresponding with clinical manifestations. Exclusion criteria of instability is defined as > 10 degrees sagittal-plane angulation a > 3 mm sagittal-plane displacement on flexion-extension radiograph (12).
Inclusion criteria
Age between 20 and 70 years
Presentation with symptomatic cervical or lumbar radicular pain
Imaging findings of a cervical or lumbar intervertebral disc pathology compatible with pain symptoms
Severe cervical or lumbar radicular pain than cervical or lumbar axial pain
Presentation with a VAS of > 4 and an ODI or Neck Disability Index NDI of > 30% after first TFESI
TFESI procedures
Strict aseptic technique was adopted for TFESI procedure (13). Patients were supine for cervical procedure and prone position for lumbar under C-arm fluoroscopy (Siemens, Erlangen, Germany). To focus the target, C-arm was rotated toward the region and controlled the cranial-caudal angle for focusing the intervertebral foramen. A 26-gauge with 90 mm spinal needle with a bend at the tip was inserted into the skin and advanced to the anterior half of superior articular process at cervical spine and to the 6 o'clock position below pedicle at lumbar spine. Then, the depth of needle tip checked by anterior posterior view and lateral view of C-arm. Test dose of contrast medium (0.2-0.3 mL) was injected to figure out whether needle tip was placed at proper position. Then, the further injection of contrast medium was performed under real-time fluoroscopic monitoring. Finally, patients received 2 mL of 0.125% bupivacaine mixed with 5 mg dexamethasone as 1st TFESI was conducted.
PRF procedures
Aseptic techniques were adopted for PRF therapy. For cervical procedures, the patient was laid in a supine position for C-arm fluoroscopy (Siemens), and a 22-gauge curved-tip cannula (SMK Pole needle 54 mm with a 4 mm active tip, Cotop International BV, Amsterdam, the Netherlands) was placed around the DRG (10). For lumbar procedures, the patient was laid in a prone position for C-arm fluoroscopy (Siemens), and an 18-gauge curved-tip cannula (SMK Pole needle 100 mm with a 10 mm active tip, Cotop International BV) was placed around the DRG.
The catheter needle (active tip electrode) was inserted and a sensory stimulation test was carried out using an RF generator (Cosman G4, Burlington, MA, USA). The catheter needle was then advanced toward the DRG until the patient reported a tingling sensation and/or dysesthesia at less than 0.3V. PRF treatment was administered at 5 Hz and a 5 ms pulsed width for 240 seconds at 45V under the constraint that the electrode tip temperature not exceed 42°C (14).
Outcome measurements
Pain intensities were assessed by VAS for arm and leg radiating pain, before treatment, and 2, 4, 8 and 12 after treatment. ODI and NDI were obtained to evaluate functional disabilities associated with lumbar and cervical radicular pain, respectively, at the same times.
Adverse events
Adverse effects were carefully evaluated at each visit to detect pain flare-up and newly developed neurologic deficits after the procedures.
Statistical analysis
Statistical analysis was conducted using SPSS ver. 23 for window and clinical course was analyzed using two-way factor repeated measures analysis of variance. Statistical significance was accepted for P values < 0.05.
Ethics statement
This prospective randomized study was conducted at a spine specialist clinic in a university hospital after obtaining institutional review board approved for the study protocol (YUMC 2010-01-023), which also complied with the tenets of the Helsinki declaration. All study subjects provided written informed consent before study commencement.
RESULTS
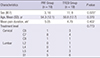
Among 193 patients underwent TFESI for the treatment of spinal radicular pain, Forty-four patients (mean age: 52.4 ± 12.3, range 23-70) that met the study inclusion criteria and were enrolled (Fig. 1). However, five patients were lost to follow up and one patient in the PRF group experienced a pain flare up and dropped out. Accordingly, 38 of the 44 screened patients were followed up for 3 months after PRF or TFESI (PRF group, n = 19; TFESI group n = 19). The demographic characteristics of the subjects were shown in Table 1. Although subjects of our study were randomly allocated, PRF and TFESI group had statistical differences in sex ratios.
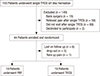
Table 1
Demographic characteristics
Changes in VAS and NDI in cervical radicular patients
Mean VAS and NDI decreased over the 3-month follow up period after TFESI and PRF. Mean VAS and NDI for cervical radicular pain were significantly improved at 2, 4, 8, and 12 weeks after TFESI and PRF (P < 0.001) (Table 2, Fig. 2). However, no significant intergroup difference was observed, although mean VAS and NDI showed marginally greater improvement after PRF at 3 months after treatment.
Table 2
Statistical results of cervical procedures by two-factor repeated measures analysis


Changes in VAS and ODI in lumbar radicular patients
Mean VAS and ODI for lumbar radicular pain also declined after TFESI and PRF, and were significantly improved at 2, 4, 8, and 12 weeks after TFESI and PRF (P < 0.001) (Table 3, Fig. 3). However, no significant intergroup difference was observed at any time point.
Table 3
Statistical results of lumbar procedures by two-factor repeated measures analysis


DISCUSSION
In this study, we evaluated the comparative effectivenesses of TFESI and PRF after 1st TFESI for the treatment of radicular pain due to disc herniation. Mean VAS, NDI, and ODI scores continuously declined after both procedures. However, the effectivenesses of the two modalities were similar over the first 3 post-procedural months.
Herniated nucleus pulposus have been reported to cause inflammation and ectopic firing in affected DRGs and spinal nerves, such as, glial activity in the spinal cord and the release of pain-modulating substances by activated glia (1516), which are involved in the development and maintenance of chronic neuropathic pain associated with central sensitization (1718). Accordingly, activated glia are considered modulators of nociception and neuropathic pain.
The rationale behind epidural steroid injection for disc herniation stems from the observation that inflammatory and nociceptive mediators concentrate around herniated discs in the epidural space (192021). Steroid treatment is well known to have excellent anti-inflammatory effects that ca decrease inflammation in DRGs, spinal nerves, and in the epidural space. Accordingly, steroid treatment probably inhibits neuroglial activation in spinal cords with acute disc herniation and/or attenuate glial activation, and for these reasons, TFESI is widely used as a conventional means of controlling and alleviating radicular pain (22). One study showed steroid injection effectively reduces the gadolinium enhancement (an indicator of nerve inflammation) of spinal nerves associated with herniated discs (23). Accordingly, TFESI was chosen in the present study as an initial treatment option for severe radicular pain after disc herniation.
The transforaminal approach, unlike the interlaminar and caudal approaches, enables steroid to be administered to target sites (21242526). In a systemic review of the effectiveness of TFESI, it was reported the effectiveness of lumbar TFESI achieved the II-1 level of evidence in the short term and level II-2 in the long term (22), and in a systemic review of the effectiveness of cervical TFESI, it was found approximately 50% of patients achieved 50% pain relief for at least 4 weeks (27). In another study, fluoroscopically guided TFESI was found to be effective at alleviating radicular pain and reducing need for surgery (282930).
We are advocates of TFESI because we believe it is an effective modality for the management of spinal radicular pain. However, despite its effectiveness, the adverse effects of TFESI raise safety issues. The majority of these adverse effects concern the administration of steroid and contrast media (527). The side effects of steroid administration include facial flushing, high blood sugar, and transient headaches, and the major complications of repeated steroid injection include suppression of pituitary adrenal axis, hypocorticism, Cushing's syndrome, osteoporosis, steroid myopathy, and epidural lipomatosis.
Catastrophic adverse events have also been reported, even when TFESI is conducted by well trained physicians, the injection of particulate steroid into an artery around the spinal canal can occlude capillaries and arterioles and cause spinal cord and cerebellar infarction resulting in permanent motor and sensory deficits (31). Recently, the non-particulate steroid, dexamethasone, was used to minimize or eliminate embolic events after TFESI (3233). Nevertheless, meticulous studies are required to confirm the safety of dexamethasone for TFESI.
On the other hand, PRF does not require the injection of steroid, contrast material, or local anesthetic, and thus, is not liable to the catastrophic adverse effects associated with vascular occlusion. Instead, PRF uses pulses of high voltage that produces an electric field around a needle tip and then allows heat to dissipate, and thus, stimulates the targeted dorsal root ganglion and the dorsal horn. Resultantly, PRF causes changes in C and Aδ fibers that transmit nociceptive and neuropathic pain (34). It has been shown application of PRF at a DRG, but not at the sciatic nerve, caused the up- regulation of activating transcription factor 3 (an indicator of cellular stress) in DRG neurons (35). In another study, pulsed RF stimulation caused neuronal changes at targeted dorsal root ganglia and in neurons of the superficial dorsal horn, which could be associated with pain processing (36).
In a rat model of lumbar disc herniation, DRG stimulation using PRF attenuated microglial activation in the ipsilateral dorsal horn and reduced pain-related behavior as evidence by reduced mechanical withdrawal thresholds. Therefore, it appears DRG stimulation by PRF influences neural systems involving in pain processing by modulating glial activities closely associated with progression and maintenance of central sensitization, and thus, DRGs are frequently chosen as targets to modulate electrophysiological change and modulate central sensitization after disc herniation. Although observed histochemical changes and increases in neural markers after DRG stimulation by PRF do not constitute a mechanism for PRF, these observations do show that PRT-induced electric fields induce neural system and gene expressional changes in DRGs and the dorsal horn (37).
Several studies that addressed chronic radicular pain have reported DRG stimulation by PRF appears to offer an effective and safe intervention for cervical and lumbar radicular pain. Choi et al. (10) reported that 71% patients with chronic cervical radicular pain refractory to repeated TFESI were satisfied with the effectiveness DRG targeted PRF. Similarly, Bozem et al. (38) reported that 55% patients with chronic intractable lumbosacral radicular showed substantial pain improvements at 6 months after PRF, and Koh et al. (39) reported that the combined application of PRF and TFESI achieved higher treatment efficacies than TFESI alone in patients with chronic refractory radicular pain. These encouraging outcomes for the treatment of chronic radicular pain might suggest central sensitization can be modulated by suppressing glia activity in the dorsal horn. However, the above-mentioned studies did not include comparable controls or validate the benefits of DRG stimulation by PRF in subacute radicular limb pain.
Our study shows the clinical outcomes of patients treated with PRF for radicular pain was not inferior to those treated by TFESI at 3 months after treatment, and that TFESI and PRF both have significant treatment effects. Patients included in the present study had sustained radicular pain of > 4 by VAS and of > 30% by ODI or NDI, despite receiving TFESI for severe radicular pain. Thus, our study subjects might have exhibited incomplete suppression of inflammation around DRGs and spinal nerves after 1st TFESI, which we believe may have produced similar outcomes in the two groups. Disc herniation increases potential for generating ectopic discharges at dorsal root ganglion, which produces central sensitization. As 1st TFESI partially suppressed inflammation around the nerve and epidural space, central sensitization at DRG and dorsal horn of spinal cord was processing, which could explain no inferior effectiveness of PRF at DRG comparing to additional TFESI.
There were randomized double-blind comparative studies for effectiveness of PRF at occipital neuralgia and adjuvant PRF with TFESI at chronic lumbosacral radicular pain (3940). However, this is the first randomized, controlled study directly to compare the effectivenesses of DRG stimulation by PRF and TFESI and validate the alternatives for the treatment of subacute radicular pain.
The majority of studies conducted on the effectiveness of PRF for the treatment of radicular pain have reported no serious adverse events, but several authors have reported flare up of pain or temporary pain aggravation (103940). In the present study, one patient experienced temporary aggravated radicular pain, which subsided after several days. Although PRF is a less destructive procedure than conventional radiofrequency treatment and does not cause neurologic deficits, PRF can cause microscopic neuronal damage, endoneural edema, and pathologic changes in myelin, possibly due to the heat generated at the electrode tip. We presume that these effects could explain the temporary aggravation of radicular pain experienced on occasion.
In conclusion, this study showed that effectiveness of PRF at DRG stimulation with respect to the treatment of recalcitrant radicular pain after first TFESI was not inferior to TFESI but was not enough to alleviate pain. Although PRF is also minimally invasive procedure that has a possibility to destruct structure, we suggest if repeated TFESI is needed or a patient has a medical condition requiring consideration with respect to the administration of steroid, such as, uncontrolled diabetic mellitus, PRF be considered a useful clinical option for the control of subacute radicular pain that helps reduce or avoid the possible catastrophic adverse effects of TFESI.
 XML Download
XML Download