

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anesthesia is a practice that regulates the level of consciousness, analgesia, hemodynamic and oxygen transport and calls for sufficient knowledge regarding physiology, pharmacology and pathophysiology of comorbid conditions and also needs enough experience to realize for a safe clinical application (12). Therefore, the anesthetic practice without the knowledge and experience can lead to death or serious morbid sequels (345). In fact, the incidence of anesthesia-related complications is rising amid growing demand for surgical operation (6). Although demand for anesthetic services is increasing, the standards that can apply to all anesthetic practices to ensure the adequate quality and patient safety have not been established in Korea.
The National Health Insurance (NHI) of Korea covers almost all Korean citizens except medical aids recipients which constitute 3% of total population. The NHI and government subsidies account for 55.5% of total health spending in 2008 (7). Currently, the NHI data serves as a major source of data on the nationwide health care utilization. Under the NHI, providers are reimbursed on a fee-for-service (FFS) basis according to the uniform fee schedule and all the insurance claims are submitted by each institution. Although all the anesthetic services are insured by NHI, the information about who performs the procedure is not required for the insurance claims in Korea. The payment system for anesthetic service is based on the class of institutions which are clinics, hospitals under 100 beds, general hospitals and tertiary referral hospitals. The institutions in the class above general hospital should hire their own anesthesiologist working exclusively for that institution. When the hospitals or clinics invite an outsourced anesthesiologist for their operation, they can claim refund for the invitation fee under the NHI.
Anesthesiologists generally maintain a low profile largely due to the nature of their work performed behind a curtain, resulting in a poor recognition by patients. Also, many of them are self-employed as a contractor or freelancer. It is hard to figure out who actually practice anesthesia in operating room unless you check medical records closely. However, their roles have a vital impact on the outcome of patients who undergo surgery (4589), signifying the need for more active involvement of anesthesiologists in perioperative management of patients. The Korean law allows all physicians to perform anesthesia regardless of their experience, which means it is legal for surgeons to perform anesthesia and surgery simultaneously. However, in those cases, nurse or nurse assistant is often involved as an anesthesia provider. Although the law prohibits nurse anesthetists working independently, they anesthetize the patients with connivance of surgeon in the field.
The aim of the present study was to investigate the states of anesthetic services in Korea by identifying anesthesia providers and to describe the possible risks associated with anesthesia performed by non-anesthesiologists.
MATERIALS AND METHODS
We collected insurance claims data filed with the National Health Insurance Review and Assessment Service from January 1, 2011 to December 31, 2013. The information related to patient, treatment, disease, and prescription was reviewed to identify the all anesthesia procedures and related payment during that period, in addition to the information of medical institutions. The institutions were classified as follows according to the medical law; clinic operates under 30 beds, hospital operates 30 to 100 beds, general hospitals operates more than 100 beds and government designates tertiary referral hospital for specializing medical care of serious disease. Clinics and hospitals under 100 beds were classified to primary care institution.
We assumed that the anesthesia was performed by the anesthesiologist when the claim included the invitation fee for anesthesiologist. All cases of anesthesia in the institutions which hire their own anesthesiologist working exclusively for that institution were assumed to be performed by the anesthesiologist. All the anesthesiologists are board certified regardless of their employment position. Although the residents in the training hospitals were not board certified, their practices were assumed to be done by supervisor anesthesiologists who are board certified.
All the anesthesia procedures except topical infiltration of local anesthetics were included and categorized into general, regional, or intravenous anesthesia. General anesthesia was subdivided into endotracheal intubation and mask inhalation. Regional anesthesia was subdivided into spinal, epidural and brachial plexus block. We adopted the term "intravenous anesthesia" for procedural sedation with intravenous anesthetics because it was commonly used in NHI. To analyze the regional distribution and interdepartmental difference of anesthesia performed by non-anesthesiologists, 2013 data was sorted by area and medical fields.
From July 2013, the mandatory diagnosis-related-group (DRG) based payments for the seven most common operations were extended to all medical institutions including tertiary referral hospitals. The surgeries under DRG system are lens procedures, tonsillectomy and/or adenoidectomy, anal procedures, inguinal and/or femoral hernia procedures, appendectomy, and uterine and/or adnexal procedures. Under the DRG system, treatment costs are not itemized in the insurance claim form, making it difficult to identify whether the anesthesia was performed by an anesthesiologist or not. To analyze the effect of DRG system on our study, we counted the claims associated with DRG and categorized them by the class of institutions. Also, we analyzed the cases of anesthesia performed by non-anesthesiologist in Cesarean section and appendectomy which are main representative surgeries for DRG from the data of 2011 when FFS was applied.
RESULTS
Institutions with directly employed anesthesiologists
The number of institutions hiring anesthesiologists slightly increased during the 3-yr research period. Although Department of Anesthesiology is mandatory to operate general hospitals, there were 4-5 general hospitals without their own anesthesiologists. Half of the hospitals did not hire anesthesiologists. For the hospitals, proportion of institutions without their own anesthesiologists was 56% in 2011, 52% in 2012, and 48% in 2013. Ninety-five percent of clinics did not have anesthesiologists.
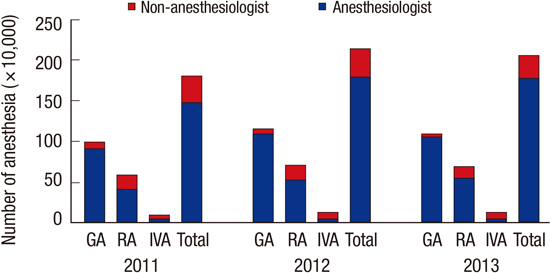
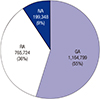
About two million cases of anesthesia were performed in a year; and general anesthesia, regional anesthesia and intravenous anesthesia were 55%-56%, 35%-36%, and 9% respectively, and the proportions were similar through the years (Fig. 1). Annual numbers (% of class total, year) of general anesthesia performed by non-anesthesiologists were 66,480 (6%, 2011), 63,271 (4%, 2012), and 36,008 (3%, 2013). For regional anesthesia, annual numbers (% of class total, year) performed by non-anesthesiologists were 170,687 (26%, 2011), 182,755 (23%, 2012), and 143,134 (19%, 2013). In case of intravenous anesthesia, annual numbers (% of class total, year) performed by non-anesthesiologists were 89,401 (54%, 2011), 98,823 (50%, 2012), and 93,864 (47%, 2013). Overall, anesthesia cases performed by non-anesthesiologists accounted for 13%-17% of total (Fig. 2).
Annual numbers (% of total, year) of anesthesia performed in the institutions without directly employed anesthesiologists were 420,488 (22%, 2011), 444,529 (20%, 2012), and 357,663 (17%, 2013). Among them, non-anesthesiologists performed 326,568 cases (78%, 2011), 344,849 cases (78%, 2012), and 273,006 cases (76%, 2013). The overall counts of anesthetic service in NHI declined in 2013, as the DRG based payment system was implemented in the year.
General anesthesia with endotracheal intubation (GAT)
About one million cases of GAT were performed in a year and 3%-6% of them were performed by non-anesthesiologists. About 77%-80% of total cases of GAT were performed in the general hospitals and tertiary referral hospitals, 17%-18% in hospitals and 3%-5% in clinics. Annual numbers (% of total, year) of GAT performed in the primary institutions were 223,272 (23%, 2011), 246,757 (22%, 2012), and 206,906 (20%, 2013) (Table 1).
The number of GAT performed in the institution without a directly employed anesthesiologist were 9%, 7%, and 5% of total GAT in the year of 2011, 2012, and 2013, respectively. Among them, non-anesthesiologists performed 63% in 2011 and 2012, and 57% in 2013. The proportion of non-anesthesiologist's practice was much higher in the hospital group than in the clinics (Fig. 3).
1) In the distribution of GAT performed by non-anesthesiologists across Korea in 2013, a total of 10,920 cases were observed in Seoul/Gyeonggi-do, accounting for 48% of 22,687 cases of GAT provided in the institutions without a directly employed anesthesiologist in that area. Seoul and Gyeonggi-do was followed by Busan/Gyeongnam showing 7,701 cases, which accounted for 93% of 8,304 cases of GAT in the institutions without directly employed anesthesiologist in that area.
2) In their distribution of GAT performed by non-anesthesiologists across medical fields in 2013, 9,714 cases occurred in the orthopedic surgery, which was followed by 5,112 cases of general surgery and 3,871 cases of obstetrics & gynecology. In particular, 100% of GAT for oral and maxillofacial surgery (235 cases) and pediatric dental treatment (125 cases) was performed by non-anesthesiologists in the dental institutions without directly employed anesthesiologist.
General anesthesia with mask inhalation of anesthetics (GAM)
About 70,000-100,000 cases of GAM were performed in a year and 9%-14% of them were performed by non-anesthesiologists (Table 2). Annual numbers (% of total, year) of GAM performed in the primary institutions were 40,467 (57%, 2011), 54,771 (61%, 2012), and 61,832 (59%, 2013) (Table 2). Annual numbers (% of total, year) of GAM performed in the institution without directly employed anesthesiologist were 12,458 (18%, 2011), 15,340 (17%, 2012), and 12,331 (12%, 2013). Among them, non-anesthesiologists performed 9,984 cases (80%, 2011), 12,390 cases (81%, 2012), and 9,283 cases (75%, 2013).
Regional anesthesia (RA)
Spinal anesthesia
About 390,000-450,000 cases of spinal anesthesia were performed in a year and 16%-22% of them were performed by non-anesthesiologists. Sixty percent of spinal anesthesia was performed in the primary institutions. Annual numbers (% of total, year) of spinal anesthesia performed in the institution without directly employed anesthesiologist were 119,169 (30%, 2011), 124,039 (27%, 2012), and 95,099 (21%, 2013), and 74% of them was performed by non-anesthesiologists (Table 3).
Epidural anesthesia
About 160,000-180,000 cases of epidural anesthesia were performed in a year and 23%-34% of them were performed by non-anesthesiologists. Eighty-six percent of spinal anesthesia was performed in the primary institutions (Table 4). Annual numbers (% of total, year) of epidural anesthesia performed in the institution without directly employed anesthesiologist were 71,950 (46%, 2011), 79,733 (43%, 2012), and 62,559 (37%, 2013). Among them, non-anesthesiologists performed 74%, 70%, and 62% in the year of 2011, 2012, and 2013, respectively.
Brachial plexus block
The number of brachial plexus block rapidly increased during the study period. About 100,000-150,000 cases of brachial plexus block were performed in a year and 23% of them were performed by non-anesthesiologists. Seventy-three percent of brachial plexus block was performed in the primary institutions (Table 5). Annual numbers (% of total, year) of brachial plexus block performed in the institution without directly employed anesthesiologist were 37,680 (36%, 2011), 45,577 (35%, 2012), and 46,419 (33%, 2013). Among them, non-anesthesiologists performed 79%, 77%, and 74% in the year of 2011, 2012, and 2013, respectively.
Intravenous anesthesia (IVA)
About 170,000-200,000 cases of intravenous anesthesia were performed in 2013 and 47.1% of them were performed by non-anesthesiologists. Seventy-six percent of intravenous anesthesia was performed in the primary institutions, mainly in the clinics (Table 6). Annual numbers (% of total, year) of intravenous anesthesia performed in the institution without directly employed anesthesiologist were 89,464 (54%, 2011), 99,185 (51%, 2012), and 94,083 (47%, 2013), and all of them were performed by non-anesthesiologists.
The effect of the diagnosis-related- group (DRG) based payment system
The numbers of DRG claims requested by clinics, hospitals, general hospitals, and tertiary referral hospitals in 2013 were 583,546, 225,546, 92,470, and 44,450, respectively. Considering the number of DRG claims of tertiary referral hospitals was the half of annual count, about 80% percent of operations that are subject to the DRG-based payment system were performed in primary care institutions. Analyzing the treatment costs claimed for C-section and appendectomy under the FFS system in 2011, 18,388 (29% of total) and 5,249 (7% of total) cases were performed by non-anesthesiologists respectively.
DISCUSSION
The result of this study shows that 13%-17% of anesthetic cases are performed by non-anesthesiologists in Korea. Annually, about two million cases of anesthesia were performed with the proportion of general anesthesia, regional anesthesia and procedural sedation with intravenous anesthetics of 55%, 36%, and 9% respectively. In England where the public health insurance is subsidized by the government which is similar to NHI in Korea, general anesthesia accounted for 76.9% of total anesthetic cases in 2013, followed by RA (14.5%), and about 87% of total anesthetic cases were provided by anesthesiologists (10). The proportion of GA in Korea is much lower than that in England, and it is because RA is commonly performed by surgeons, implying a possibility that RA is preferred over GA by convenience rather than clinical reasons. This phenomenon is spurred by the current payment system of NHI which is not based on the individual practitioner, and the fact that surgeons are the key decision makers when it comes to anesthesia.
About 80% of total cases of GAT were performed in general hospitals and tertiary referral hospitals, while the remaining cases were done by hospitals and clinics. Although general hospitals should hire their own anesthesiologist, clinics and hospitals are the primary care institutions and hiring an anesthesiologist is not mandatory. According to 2013 data, almost half of primary care hospitals do not hire anesthesiologists. In these hospitals, 76% of anesthesia including GA, RA, and IVA were performed by non-anesthesiologists, and 67% of GAT were performed by non-anesthesiologists. Interestingly, the incidence of non-anesthesiologist-performed GAT in the hospitals was higher than in the clinics. This finding suggests that the hospitals hire a non-physician substitute for anesthesiologist to cover more anesthetic cases than in the clinics.
By region, the distribution of non-anesthesiologist-performed GAT was higher in large cities, including Seoul and Busan. The clinics and hospitals performing surgeries not covered under the NHI e.g. cosmetic surgeries are concentrated in the cities. If surgical procedures subject to the DRG-based system and those not covered by the NHI added, the number of non-anesthesiologist performed GAT would sharply soar.
By medical specialty, non-anesthesiologist-performed GAT was higher in the orthopedic field in 2013. However, if surgical procedures subject to the DRG-based system added, general surgery, obstetrics & gynecology and ear-nose-throat clinics would also exhibit significantly many non-anesthesiologist administration cases. In addition, oral and maxillofacial surgery in dental institutions and pediatric dental treatment dominantly rely on non-anesthesiologists. Anesthesia for these two sub-specialties requires expertise because airway management in those surgeries is quite complicated. The prevailing anesthetic cases by non-anesthesiologists pose a serious concern.
Given the nature of GAT, surgeons cannot operate the surgery and GAT simultaneously. Instead, other personnel to be inferred as nurse or nurse assistant perform anesthetic management. Nurses can monitor the vital signs of patients and assist physicians in performing anesthesia practice, but they are not allowed to practice by themselves in Korea. When surgeons or nurses performed anesthesia in resource-deficient clinical settings, anesthesia-related mortality increased markedly (11121314). In Korea, there was a period when the supply of anesthesiologists was scarce, nurses or nurse assistants filled them to administer GA under the supervision of surgeon. The current widespread reliance on non-anesthesiologists in major cities of Korea is not due to undersupply of qualified anesthesiologists but is a matter of choice. A lack of knowledge on anesthesia safety is likely coupled with the desire to cut costs to boost the phenomenon favoring non-anesthesiologists. The shift to the DRG-based payment system also resulted in accelerating the phenomenon.
Freelance anesthesia is a Korea-specific medical culture and sought by hospitals without directly employed anesthesiologists whenever they need an anesthesiologist. Under the NHI, the hospitals can claim back the money spent on freelance anesthesia by providing the information on the outsourced anesthesiologist. The preference for freelance anesthesia stems from the perception of anesthesia as a simple medical technique. If surgeons consider anesthesia a supplementary means for surgery, they may request a nurse or even a nurse assistant for easy cooperation. Patients' poor recognition of the role of anesthesiologists also partly explains the heavy reliance on freelance anesthesia. According to the results of a study on Korean people's perception of anesthesia, 75% of respondents were aware that anesthesia is provided by anesthesiologists, but less than 20% had correct knowledge on the activities of anesthesiologists (15).
A lack of recognition of RA is more prominent because the incidence of non-anesthesiologist-performed RA ranged from 19% to 26%. While GA is performed illegally in many hospitals, RA tends to be performed by surgeons themselves because RA can be performed in the preoperative phase of surgery and because patients remain conscious during the administration of RA. That is, it is easy for surgeons to take care of the patients while they are doing operation. It is however possible that RA is also performed by non-physician in real clinical settings. RA should be performed by anesthesiologists to prevent contingent complications that can be caused by local anesthetics and changing hemodynamic status in response to extended block or surgical manipulations. For example, although surgeries to repair femur facture or C-sections can be performed under RA, intraoperative anesthetic management is important because the target level is high and hemodynamic fluctuation is significant during the operation. Epidural anesthesia requires a higher dose of local anesthetic agent, compared with spinal anesthesia, calling on anesthesiologist's expertise to prevent complications such as systemic toxicity and total spinal anesthesia.
Almost all procedural sedation with intravenous anesthetics are performed by surgeons in hospitals without directly employed anesthesiologist. Although intravenous injection does not require complicated techniques like intubation and ventilation assist, adequate proficiency is a very important element for anesthesia providers to avoid adverse consequences such as respiratory suppression, laryngospasm and pulmonary aspiration. IVA can vary doses of anesthetic agents to achieve different levels of sedation, depending on the degree of pain desired during surgery. However, the NHI does not discern the differences in IVA. According to a study analyzing the anesthesia related medical disputes filed in the Korean Society of Anesthesiologists (KSA), 50 cases of total were associated with GAT and 39 cases were associated with IVA (3). Of 36 cases of IVA mentioned above were performed by non-anesthesiologists to produce deep sedation using propofol. The regulations are therefore necessary to guarantee safe IVA practices. Researchers have claimed that most IVA-induced death were preventable through adequate guidance and training (36). Unlike a light sedation with short acting intravenous anesthetics, deep sedation for prolonged procedures include all the risks of general anesthesia. Deep sedation should be differentiated from simple IVA, and the equipments for monitoring and managing suitable to general anesthesia and also expertise anesthetic personnel should be guaranteed (16).
Freelancer anesthesiologists are working for many different hospitals and clinics that have no directly employed anesthesiologists. It means that they are not familiar with anesthesia work stations, and they may be under a time constraint when their work schedules are delayed at a hospital or a clinic. Although preanesthetic assessment of patient is an important procedure to improve the safety of anesthesia (581718), there is not enough time for freelancer anesthesiologist to interview the patients and evaluate them. Preoperative assessment is usually performed by surgeon, and therefore it is not always appropriate. All of these factors can affect patient safety. Anesthesiologists are required to offer perioperative services aimed to help patients have a safe hospital experience beyond their basic duty of administrating anesthesia (125). Their role should encompass not only preoperative assessment but also acute phase of recovery progress because postanesthetic management is important. According to the data released by KSA, 25% of anesthesia related medical disputes occurred in the recovery period (19). Despite the importance of preanesthetic assessment and postanesthetic management, these procedures cannot be properly performed in hospitals when they rely on outsourced anesthesiologists. Further actions should be therefore taken to impose active role of anesthesiologists in pre- and post-anesthesia management. According to the international standards, at least one proficient anesthesiologist is required for hospital with more than 100 beds to perform minor surgeries (e.g. laparotomy and surgeries to repair fracture and hernia), and then the anesthetist is allowed to perform GAT and neuromuscular blocking agents. The hospital should be equipped with necessary equipment for resuscitation, defibrillation, end-tidal carbon dioxide, pulse oxygen saturation(SpO2) and electrocardiography (20).
The limitation of the study is that we assumed all the anesthesia including GA, RA, and IVA were provided by anesthesiologists in hospitals employing anesthesiologists directly. Those hospitals may not be properly armed with anesthesia providers in operating rooms because their anesthesiologists may be involved only in outpatient care such as pain clinics. It is also debatable to define IVA performed by surgeons, which are common even in tertiary referral hospitals, and anesthetic services provided by residents in night shift as anesthesiologist-performed services. As mentioned earlier, the information on anesthesia providers are not disclosed when an insurance claim is made, meaning that we cannot obtain actual information on anesthesia providers from the public health database. We therefore assumed that all the anesthetic cases are supervised by anesthesiologists in hospitals employing anesthesiologists directly. The anesthetic cases for which an outsourced anesthesiologist was not requested in the institutions without directly employed anesthesiologist meet the minimum criteria to define non-anesthesiologist's practice. Therefore, the actual cases of non-anesthesiologist's anesthesia must be greater than that estimated in this study.
Despite the rising demand for anesthetic care, the overall counts of anesthetic service and GAT performed by non-anesthesiologists declined in the wake of the implementation of the DRG-based payment system in 2013. Surgical procedures that are subject to the DRG-based system were usually conducted in primary care institutions and half of them were performed by non-anesthesiologists. Therefore many GAT performed by non-anesthesiologists were masked by DRG-based system. Because the NHI data represent only 55.5% of total health market, we do not know about the remaining 44.5%. Because the surgeries not covered by NHI are usually performed in primary care institutions, more cases could be performed by non-anesthesiologist in the field. In fact, medical disasters associated with anesthesia usually occurred in the surgeries not covered by NHI and those were performed by non-anesthesiologists (36).
To promote anesthetic services that prioritize the safety of patients, surgeons and patients need to enhance their perception of anesthesia. Information on the role of anesthesiologists can be provided to the public, and the payment system can be revised in a way that advocates anesthesiologist-performed anesthetic services. Also, GAT and IVA aimed for deep sedation can be performed by only anesthesiologists as a requirement. Poor recognition of anesthesiologists should be also improved by interacting with patients before and after operation and establishing adequate rapport with them. Patients have the right to know about their anesthesiologists before undergoing surgery. They must want to know who will monitor their vital signs and help them get through difficult times in operation room.








 XML Download
XML Download