

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Attention-deficit/hyperactivity disorder (ADHD) is the most common childhood disorder in psychiatric outpatient clinics and affects 3%-8% of the pediatric population worldwide (1). On contrary to previous notion as a condition of childhood, it has been known that ADHD continues and causes significant psychosocial impairment across life span (2). It has been reported that children and adolescents with ADHD have increased risks for challenging behaviors, school drop-out, earlier substance use associated with conduct problem, and problem gambling, as well as mood and anxiety disorders (3456). Adults with ADHD had high risk for a wide range of adverse psychosocial outcomes including low academic achievement, low socioeconomic status, low rates of professional employment, and difficulty in maintaining occupational status and social relationships as well as increased rates of psychopathology including antisocial, addictive, mood and anxiety disorders (7).
Considering the chronic nature and adverse outcome of ADHD, earlier detection and better adherence to treatment seem to be important throughout treatment period. Along with behavioral treatment and educational intervention, medication leads to not only the reduction of core symptoms but also the improvement of academic difficulties, behaviors problems, and psychiatric comorbidities in children and adolescents with ADHD (8910). Stimulants were considered as the first-line therapy for children with ADHD. While shorter half-life of immediate-release methylphenidate hindered children and adolescents with ADHD from adhering to their medication, the extended-release or osmotic-controlled release oral delivery system methylphenidate improved adherence and efficacy (1112). In addition, nonstimulants including atomoxetine have been used alternatively for the treatment of ADHD in children and adolescents (13). However, suboptimal treatment and poor medication compliance were not uncommon even for 12 months of treatment (1415). In addition, the debates on the overdiagnosis of ADHD and misuse of medications have been continued, which seemed to affect the compliance to medications negatively (16).
A better understanding of the utilization patterns of ADHD medication would be beneficial for clinicians and public health care professionals to determine treatments which can provide effective care with minimal adjustment of health care resources. In order to measure the adherence to long-term drug therapy retrospectively, analysis of prescription claims data has been used as a fairly reliable method. However, until now, the adherence to ADHD medication in several countries has been reported using the prescription claims data from either only selected populations or national representative samples with 1 year of less observation period (1517181920).
In Korea, the National Health Insurance (NHI) system exists, which is mandatory by Korean law since 1989 (21). The Korean Health Insurance Review and Assessment (HIRA) claims database of NHI system had information regarding prescription patterns and diagnosis in the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10). Therefore, it can be used as a nationwide source of information regarding the use of health care resources during ADHD treatment.
In the current study, we evaluated the associations between ADHD medication groups and the measures of utilization patterns including persistence and adherence in children and adolescents with ADHD using information on the Korean HIRA database. The null hypothesis in the current study was that there are no differences among 4 different ADHD medications available in Korea for children and adolescents in persistence and adherence.
MATERIALS AND METHODS
Study population
The current study was performed using data from the Korean HIRA claims database from January 1, 2009 to December 31, 2013. We selected the information from children and adolescents between 6 and 18 years of age who had the diagnosis of ADHD (ICD-10 code F90.0) and newly received their medication at least twice from between January 1, 2010 and December 31, 2010. To be eligible for the current study, subjects were considered as new to ADHD medication if no ADHD medications had been dispensed for at least 360 days before the index date that was defined as the date of the first fill.
Procedures and assessment
The socio-demographic factors including age, sex, the type of insurance, and the hospital level were obtained from the Korean HIRA database. According to their initial ADHD medications, we categorized the data of children and adolescents with the ADHD into 4 groups as follows: 1) immediate-release methylphenidate (IR-MPH), 2) extended-release methylphenidate (ER-MPH), 3) osmotic-controlled release oral delivery system methylphenidate (OROS-MPH), and 4) atomoxetine (ATX). If different medications were used in their initial 2 visits in 2010, the medication prescribed more frequently and/or at a higher dosage in the first 2 visits was selected as an initial one. In addition, the change of initial drug was regarded as a discontinuation. In 2010, clonidine was withdrawn from market and not available in Korea. Atomoxetine was only covered from the Korean NHI system when specific comorbid conditions, such as a severe anxiety and Tourette syndrome, were present in children and adolescents with ADHD. The combination of these medications was typically not covered by Korean National Insurance. Data of the subjects were followed up from the initiation of treatment with ADHD medications in 2010 (index event) to December 31, 2013.
In the current study, persistence was defined as the number of days of continuous treatment with medication during the post-index period (from the index date to the last date of medication prescription). Considering frequent drug holiday during either vacation or weekend in the treatment of children and adolescents with ADHD, we defined the refill gap longer than 60 days (GAP60) as well as the conventional 30 days or more refill gap (GAP30) as discontinuation of a treatment. In addition, for sensitivity analysis, 15 days or more refill gap was used in order to check the robustness of the results. Adherence was calculated using the Medication Possession Ratio (MPR) which reflects the proportion of days that patients were in possession of their prescribed medication. In the current study, the MPR was calculated by summing days being supplied and dividing by days being treated (i.e., the day intervals between the last date of medication prescription and index date). We evaluated the adherence using the MPR with the conventional 70% and 80% cut-offs. Sensitivity analysis was also conducted at 90% cut-off. Utilization parameters during post-index period including persistence and adherence were measured for 36 months or more.
Along with sex, children and adolescents with ADHD were divided into 2 age groups as follows: 6–12 and 13–18 years of age. The insurance type was classified into two categories: National Health Insurance and Medical Aid. The hospital level was stratified into two groups: general hospitals and private clinics.
Statistical analysis
Differences among ADHD medications in the number of those who discontinued and remained adherence were analyzed using chi-square test. Mean days before discontinuation were compared using ANOVA with post-hoc comparison. To assess the association between medications and persistence and adherence, a multivariate logistic regression analysis was employed, controlling for age, sex, and hospital level. SAS 9.3 (SAS Institute, Inc., Cary, NC, USA) was used to analyze the data. An a priori significance level of P < 0.05 was used throughout all statistical analyses.
RESULTS
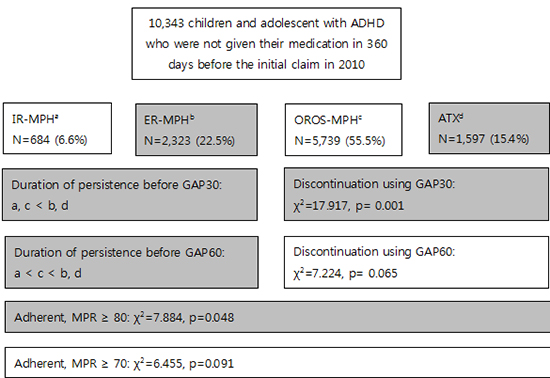
In 2010 Korean HIRA claims database, the total number of newly diagnosed children and adolescents with ADHD was 28,436. Our study sample consisted of 10,343 children and adolescents with ADHD who were not given their newly prescribed medication in 360 days before the initial claim in 2010.They were largely 6-12 years of age (n = 7,592, 73.4%), boys (n = 8,223, 79.5%), those who had Korean National Health Insurance (n = 10,272, 99.3%), and those who were treated in private clinics (n = 7,382, 72.4%). The most frequently prescribed drug was OROS-MPH (n = 5,739, 55.5%), followed by ER-MPH (n = 2,323, 22.5%), ATX (n = 1,597, 15.4%), and IR-MPH (n = 684, 6.6%) (Table 1).
Table 1
Characteristics of 10,343 eligible children and adolescents in the current study

ADHD, attention-deficit/hyperactivity disorder; IR-MPH, immediate-release methylphenidate; ER-MPH, extended-release methylphenidate; OROS-MPH, osmotic-controlled release oral delivery system methylphenidate; ATX, atomoxetine.
![]()
Comparisons of persistence and adherence among 4 ADHD medication groups are presented in Tables 2 and 3. Among 4 ADHD medication groups, significant difference was found in number of children and adolescents who had more than GAP30 (χ2 = 17.917, P < 0.001) during their individual follow-up period. The lowest mean days before GAP30 were 175.2 ± 202.1 in OROS-MPH group, followed by 181.1 ± 225.0 in IR-MPH group, 187.2 ± 221.1 in ER-MPH group, and 192.3 ± 227.3 in ATX group (ANOVA: F = 3.604, P = 0.013, IR-MPH, OROS-MPH < ER-MPH, ATX in post hoc Tukey test). There were a trend toward significance when we used GAP60 (Chi-square test: χ2 = 7.224, P = .065). The mean days before GAP60 was 367.0 ± 274.1 in IR-MPH group, 403.1 ± 291.2 in ER-MPH group, 394.0 ± 292.1 in OROS-MPH group, 405.2 ± 274.0 in ATX group, respectively (F = 3.418, P = 0.017, IR-MPH < OROS-MPH < ER-MPH, ATX in post hoc Tukey test) (Table 2).
Table 2
Persistence of ADHD medications

ADHD, attention-deficit/hyperactivity disorder; GAP30, 30 days refill gap; GAP60, 60 days refill gap; IR-MPH, immediate-release methylphenidate; ER-MPH, extended-release methylphenidate; OROS-MPH, osmotic-controlled release oral delivery system methylphenidate; ATX, atomoxetine.
![]()
Table 3
Adherence of ADHD medications
ADHD, attention-deficit/hyperactivity disorder; MPR, medication possession ratio; IR-MPH, immediate-release methylphenidate; ER-MPH, extended-release methylphenidate; OROS-MPH, osmotic-controlled release oral delivery system methylphenidate; ATX, atomoxetine.
![]()
Using 80% cut-off of the MPR, 188 (27.5%) in IR-MPH group, 708 (30.5%) in ER-MPH group, 1,610 (28.1%) in OROS-MPH group, and 349 (26.7%) in ATX group achieved the adherence, which was significantly different (χ2 = 7.884, P = 0.048).There was a trend of significance in the MPR using 70% cut-off (χ2 = 6.455, P = 0.091) (Table 3).
Results from the multivariate logistic regression analyses of persistence (30 and 60 days refill gap), adherence (MPR 70% and 80%), and 4 ADHD medications controlling for age, sex, and the hospital level were presented in Tables 4 and 5. When we used GAP30, ER-MPH, OROS-MPH, and ATX groups showed less discontinuation compared to IR-MPH group [odds ratio (OR) = 0.528, 95% CI: 0.279-0.996, P = 0.049; OR = 0.360, 95% CI: 0.203-0.639, P < 0.001; OR = 0.270, 95% CI: 0.118-0.618, P = 0.002]. Using GAP60, multivariate logistic regression showed OROS-MPH group had a statistical tendency toward more persistent than IR-MPH (OR = 0.859, 95% CI: 0.731–1.011, P = 0.068). In addition, no significant differences were observed with other 2 ADHD medications compared to IR-MPH. Regarding covariates, general hospitals had a tendency toward more persistence compared to private clinics when we used GAP30 (OR = 0.597, 95% CI: 0.357–1.000, P = 0.050). In addition, when we used GAP60, children (6-12 years of age) discontinued less than adolescents (13-18 years of age) (OR = 0.693; 95% CI: 0.632–0.759, P < 0.001), while general hospitals were associated with less discontinuation compared to private clinics (OR = 0.526; 95% CI: 0.479–0.577, P < 0.001), respectively. In sensitivity analysis, results were similar those for GAP30 in the association between persistence and ADHD medications. However, sex was rather significant covariate than hospital level in that case (OR = 1.602, 95% CI: 1.021-2.513, P = 0.040) (Table 4).
Table 4
Logistic regression analysis of ADHD medication types and likelihood of discontinuation*

ADHD, attention-deficit/hyperactivity disorder; GAP30, 30 days refill gap; GAP60, 60 days refill gap; IR-MPH, immediate-release methylphenidate; ER-MPH, extended-release methylphenidate; OROS-MPH, osmotic-controlled release oral delivery system methylphenidate; ATX, atomoxetine.
*Reference categories: IR-MPH, adolescents, boys, and private clinics.
![]()
Table 5
Logistic regression analysis of ADHD medication types and likelihood of adherence*
ADHD, attention-deficit/hyperactivity disorder; IR-MPH, immediate-release methylphenidate; ER-MPH, extended-release methylphenidate; OROS-MPH, osmotic-controlled release oral delivery system methylphenidate; ATX, atomoxetine.
*Reference categories: IR-MPH, adolescents, boys, and private clinics.
![]()
Logistic regression analysis of adherence showed no differences among 4 medication types. Regarding covariates, girls were more adherent compared to boys(80% cut-off applied, OR = 1.165, 95% CI: 1.048–1.294, P = 0.005; 70% cut-off applied, OR = 1.198; 95% CI: 1.084–1.324, P < 0.001) and general hospitals were significantly more adherent than private clinics (80% cut-off applied, OR = 1.573; 95% CI: 1.434–1.725, P < 0.001; 70% cut-off applied, OR = 1.608; 95% CI: 1.472–1.757, P < 0.001), respectively. In sensitivity analyses using 90% cut-off, similar results were found for both 70% and 80% adherence cut-off level (Table 5).
DISCUSSION
The aim of the current study was to investigate differences in ADHD medication utilization patterns across a follow-up period. In the present study, we retrospectively explored the associations between 4 available medications in Korea and persistence and adherence in children and adolescents with ADHD. To our best of knowledge, this is the first study comparing both persistence and adherence among ADHD medications directly in children and adolescents in Korea. In addition, the follow-up period in the current study, at least 36 months, was the longest observation period for adherence in treatment of ADHD until now. In previous studies, most had observation period up to 1 year (22). Until the current study, the longest treatment duration was 6 years for treatment discontinuation and 2 years for adherence (2324).
Discontinuation rates for 4 ADHD medications in our sample ranged from 97.7% for IR-MPH to 99.4% for ATX using GAP30 and from 56.7% for IR-MPH to 62.3% for ER-MPH using GAP60. In the number of discontinued, we found significant differences among medications using GAP30. Among 4 ADHD medications, ER-MPH and ATX had more days before both GAP30 and GAP60 than IR-MPH and OROS-MPH. In logistic regression analyses, ER-MPH, OROS-MPH, and ATX showed less discontinuation compared to IR-MPH group when GAP30 was used. Our results partially concurred with findings from previous studies, which suggested that there would be differences in ADHD medication discontinuation rates according to medication classes and action time in children and adolescents (15171819202526). The present results suggested that children and adolescents, who were treated by IR-MPH that has shorter action time and needs multiple daily doses, discontinued earlier and more than those treated by other 3 ADHD medications available in Korea.
In previous studies, the discontinuation rates within 1 year for stimulants ranged from 19.1% for long-acting stimulants in 15,838 subjects of all age in Quebec, Canada to 99% for short-acting MPH in 10,153 newly diagnosed children and adolescents with ADHD under 18 years of age in Taiwan (1825). In addition, in Italian sample of children and adolescents, the discontinuation rate for ATX was 26.0% for 1 year (26).Similar to the current study, Barner et al. (15) enrolled 62,789 children and adolescents (3-18 years of age) in Texas Medicaid and compared differences in persistence using GAP30 among medication types including ATX. In their 1-year follow-up, ATX users persisted most, followed by ER-MPH, prodrug stimulant. In IR-MPH users, there was the lowest persistence. In the current study, we followed up data from the Korean HIRA claims database up to 3 years or more, which might explain partly higher discontinuation rate in our sample than previous results in other countries.
Although the effectiveness of ADHD medications has been demonstrated, treatment discontinuation is fairly common phenomenon. In previous studies, the discontinuation of ADHD medications has been associated with suboptimal control of symptoms, increasing the likelihood of harmful and serious behaviors including social adversity, academic difficulties, behavioral problems, and poor economic, social, and emotional well-being (282930). In addition, family and associated community members can be influenced by these adverse consequences as well (3132), which could not be measured in the current study because the data from the Korean HIRA claims database were not allowed to link with any information of their family members. In previous studies, changes in parenting stress and parental quality of life were measured during the 8-week treatment with OROS-MPH in children and adolescents with ADHD. Hwang et al. (31) found significant decreases in score of the Parenting Stress Index, Short Form from baseline to week 4 and from week 4 to 8, respectively in 495 parents whose children or adolescents with ADHD were treated. In addition, a significant improvement in parental World Health Organization Quality of Life, Brief Scale (WHOQOL-BREF) score was observed in 75 parents of children and adolescents with ADHD during treatment.
As was the case in persistence, there was a significant difference among medications in the number of those who were adherent when we used 80% cut-off of the MPR. The rate of subjects who had a MPR greater than 80%ranged from 26.7% for ATX to 30.5% for ER-MPH. In previous studies, it has been suggested that adherence to ADHD medications would be comparable with estimates for psychiatric disorders in adults including schizophrenia and bipolar disorder as well as chronic medical conditions with low adherence including hyperlipidemia, diabetes, hypertension, etc. (333435). In previous studies using an 80% cut-off of the MPR, the rate of adherence for 12 months ranged from 9.8% for short-acting stimulants to 64% for long-acting stimulants including dexmethylphenidate, methylphenidate, and mixed amphetamine salts and 67% for nonstimulants (1536). According to a recent meta-analysis (22), the pooled MPR in 12 months for children and adolescents ranged from 0.56 for long-acting stimulants to 0.67 for a nonstimulant (ATX). The rate of adherence in the current study was lower than those in previous studies. As the adherence levels can be changed due to study periods as well as medication classes and action time (22), results from previous studies should be interpreted cautiously.
In logistic regression analysis of adherence, we could not find any differences among 4 medication types in both 80% and 70% cut-off, which suggest that the adherence in long-term follow-up would be associated with other factors than medication. In logistic regression analyses of our samples, instead of medications, covariates including girls and general hospitals were associated with increased adherence. In addition, older age and private clinics would predict medication discontinuation. Recently, Charach and Fernandez (37) suggested that the adherence of ADHD medications could be decreased by several factors. Medication factors including medication ineffectiveness, adverse effects, multiple daily doses, and difficulties in adjusting the dose regimen could decrease the adherence. In addition, for the parent and family factors, older parents, increased parent-child conflict, bad belief or stigma (e.g., “ADHD symptoms are not a disorder”, “drugs are not safe”, “I cannot believe medical system”, and so on), and burden of the medication regimen were associated with decreased adherence. The Healthcare system and professional factors included the cost of medication and the lack of providers in the community. For the child factors, older age at diagnosis, family history of ADHD, severe behavior problems at home, and unwillingness were listed. At last, for the adolescent factors, negative attitudes toward medication, stigma, concerns about treatment dependence, and experience of social withdrawal seemed to decrease the adherence.
In the current study, while there was no difference in discontinuation between sex, girls with ADHD were more adherent than boys, as was contrary to the previousnotion of low medication adherence in female sex (38). Generally, as comorbidities were associated with low medication adherence (38), we speculated that the result of higher adherence in girls with ADHD may result from differences in comorbidity pattern. Girls with ADHD tend to have lower self-efficacy and internalize their symptoms while they show less hyperactivity-impulsivity symptoms and externalizing behaviors including physical aggression which may cause an increase of parent-child conflict and severe behavior problems at home, and unwillingness toward medication (3739).
The current study has several strengths. First, the use of HIRA data enabled us to evaluate the patterns of medication use in nearly entire population of children and adolescent in Korea. Second, we were able to assess persistence and adherence with data of 36 consecutive months or more according to the types of medications used to treat ADHD. Third, using the prescription claims data, we could analyze the utilization pattern of atomoxetine which has relatively limited data compared to stimulants.
However, the current study also has several limitations. First, although Korean NHI system covers almost all population, some individuals worry about their privacy and will pay all the cost without the coverage of national insurance. This phenomenon is common in psychiatric field in Korea, which may cause the omission of some data. Second, in Korea, atomoxetine was introduced in 2009 and had indications only when specific comorbid conditions, such as a severe anxiety and Tourette syndrome, were present in children and adolescents with ADHD. Therefore, it was possible for atomoxetine users to have distinct utilization pattern compare to stimulants users. Third, because the change of initial drug was regarded as a discontinuation, mainly used medication could be different from the initial one. Fourth, the Korean HIRA claims database of NHI system permits only 5-year data because of the administrative reasons. Therefore we could not report the utilization patterns beyond 36 months. Finally, the influences of other factors that have been known to be associated with the utilization of ADHD medication (e.g., ADHD symptom level, general adaptation, stigma, concerns, and family factors) could not be considered in the current study. It has been known that patients as well as and their family members have negative attitudes to psychiatry as they fear of being mentally ill because of a stigma (40). They concern about negative outcomes of the unwanted revelation of their medical record. Some patients may pay in full without making claims to HIRA. Patients also choose other treatment including cognitive behavioral therapy (CBT), play therapy, or learning therapy, rather than pharmacological treatment. In addition, because the diagnosis related group system has been applied in all psychiatric patients with Korean Medical Care, there was a possibility that detailed diagnostic information might be omitted in the Korean HIRA database.
Better understanding of the influences of ADHD medication on the utilization pattern may lead to effective clinical intervention strategies for children and adolescents with ADHD and their parents. The results of the current study may contribute to add some evidence for effective adjustment of health care resources. Among Korean NHI system, persistence and adherence varied depending on medication types, with IR-MPH having the lowest values. Overall adherence and persistence of ADHD medications in Korea are suboptimal. We suggest therapeutic strategy that should be assessed regularly in order to improve future outcomes in children and adolescents with ADHD.
 XML Download
XML Download