

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The uterus, which is associated with sex and childbirth, has been socioculturally recognized as a symbolic organ of mature women (1). According to the 2011 in-depth analysis of the results of a patient survey in South Korea, 329.6 in every 100,000 women had undergone hysterectomy, the highest rate among the OECD countries (2). Fibroids and adenomyosis are the most common indications of hysterectomy, accounting for approximately 30% and 20% of the total, respectively (3). According to the National Health Insurance Service of South Korea, 237,000 patients were diagnosed with fibroids in 2009, and the number increased to 293,000 in 2013 for a mean annual increase of 5.5%. The number increased in all age groups except the 20s or younger (4).
The fundamental method of benign uterine tumor treatment is hysterectomy or myomectomy, but it requires general anesthesia, hospitalization, and a long recovery period. Furthermore, women who want pregnancies or want to preserve their uterus require non-invasive treatments (5). High-intensity-focused ultrasound (HIFU) is a non-invasive and non-hazardous method of preserving organs. It can be used repeatedly and is not affected by the lesion size. The treatment process can be monitored in real time for evaluation of its performance. Physical trauma can be minimal because no incision or resection of tumors is performed. The normal functions of the uterus could be maintained (67). However, few fundamental studies on HIFU treatments have been conducted in South Korea.
In this study, the effects of HIFU on fibroids and adenomyosis patients treated in a Hospital in South Korea were analyzed.
MATERIALS AND METHODS
Study subjects
Of the 1,168 patients diagnosed with fibroid or adenomyosis (546 fibroids patients and 622 adenomyosis patients) 333 patients (141 fibroid patients and 192 adenomyosis patients) who underwent HIFU treatment between February 4, 2010 and December 29, 2014, and followed for three- and six-month follow-ups were selected for this study. To enhance the accuracy of the volume measurements, the subjects were followed up for up to six months.
HIFU treatments and the tumor volume measurement method
Before HIFU treatment, the size and location of the fibroids and adenomyosis were confirmed using transvaginal ultrasound, and the feasibility of the HIFU procedure was assessed through simulation. The strength of the ultrasound was adjusted from 300 W to 400 W considering the subject's pain level and the transmutation level of the fibroid and adenomyosis shown in the ultrasound. The clinician determined the treatment duration. The median room time was 102 minutes, and mean time for sonication was 20 minutes 11 seconds.
ACCUVIX V10 (Samsung Medison, Seoul, Korea) was used to measure the tumor volume. A single gynecologist measured the horizontal, vertical, and longitudinal lengths of the fibroids and adenomyosis using the transvaginal ultrasound method before the HIFU procedure was performed, and the process was repeated three and six months later (Fig. 1). In patients with two or more fibroids or adenomyosis, the largest one was measured, and their volume was calculated using the following ellipsoid volume equation. H: Horizontal Length, V: Vertical Length, L: Longitudinal Length
Fig. 1
Measurement of the adenomyosis by ultrasound scanning. (A) Horizontal & vertical length. (B) Longitudinal length. (C) Horizontal and vertical length. (D) Longitudinal length.

SPSS ver. 18.0 was used for the statistical analyses. ANOVA was used for the analyses according to the subject's age, fertility, and treatment duration, and the independent T test was used for the analysis by disease. The significance test was used to verify the significance of the volume reduction and the reduction rate of the fibroids and adenomyosis. Statistical significance was accepted at P < 0.05.
RESULTS
Treatment effects according to the subject's age
In all age groups of the subjects who underwent the HIFU procedure, decreases in the benign tumor volume were measured. The 30s group showed the greatest reduction of 158.36 cm3, but the differences among all age groups were statistically insignificant. In terms of the reduction rate of the benign uterine tumor volume, all age groups showed changes three and six months after HIFU treatment. The 20s groups showed the highest reduction rate of 64.9% six months later, but the difference was statistically insignificant (Table 1).
Table 1
Changes in the benign uterine tumor volume according to the subject's age

Treatment effects according to the subject's disease
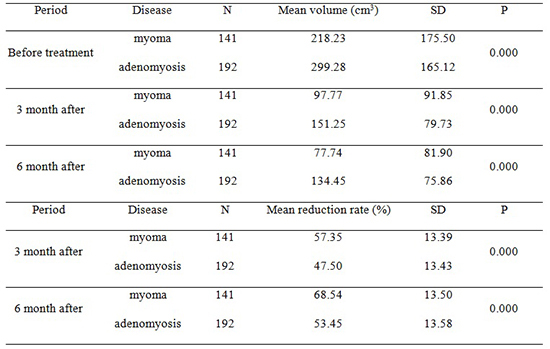
The adenomyosis volume decreased by 164.83 cm3 six months later, which was the most statistically significant treatment effect. The myoma showed a statistically significant 68.5% volume reduction rate (Table 2).
Table 2
Changes in the reduction rate of the benign uterine tumor volume according to the subject's disease

Treatment effects according to the subject's fertility
The reduction of the benign uterine tumor volume was statistically significant up to six months after treatment in all fertilities. The volume reduction rates were sustained for up to six months after treatment, but the difference was statistically insignificant (Table 3).
Table 3
Changes in the reduction rate of the benign uterine tumor volume according to the subject's fertility

Benign uterine tumor change according to the treatment duration
In all treatment durations, the benign uterine tumor volume decreased with statistical significance up to six months post-operatively. The volume reduction rate were unchanged up to six months after treatment, so the difference was statistically insignificant (Table 4).
Table 4
Changes in the reduction rate of the benign uterine tumor volume according to the subject's treatment duration

DISCUSSION
Most recently, HIFU has been widely applied in clinical cases, and an increasing number of hospitals are using HIFU equipment. HIFU is recognized as a more conservative and safe method with a faster recovery time than surgical methods, thereby drawing the attention of patients with benign uterine disease. However, its treatment effects and safety have not yet been adequately studied.
In previous studies, only the reduction rates of fibroids and adenomyosis--no other factor of the benign uterine tumor size--were investigated (89). In addition, the factors of the treatment effects according to the patient's age, disease, fertility, and HIFU treatment duration were not investigated. In this study, the effects of HIFU treatments according to the patient's age, disease, fertility, and treatment duration were examined.
During HIFU treatment, the necrotized benign tumor is absorbed via the nearby micro-blood flow. Thus, this study was conducted to prove the hypothesis that younger patients with an active blood flow experience better treatment effects. In our results, the treatment effects in the 20s age group were the greatest, and those in the 30s age group were the lowest, but the benign uterine tumor volume reduction and its reduction rates did not show a statistically significant difference among the age groups.
In this study, the volume reduction and the volume reduction rate of fibroids and adenomyosis were statistically significant. In a previous study on the changes in fibroids and three, six, and 12 months after completion of HIFU treatment, the volume was reduced by 58.1%, 66.2%, and 77.6%, respectively. Regarding adenomyosis, reduction rates of 44.0%, 47.0%, and 54.0% were observed, respectively (10). Ren et al. (11) reported the reduction rates of 27.2%, 47.9%, and 50.3% at 3, 6, and 12 months, respectively (11), and Wang et al. (8) showed 46.7%, 68.2%, 78.9%, and 90.1% at 3, 6, 12, and 24 months, respectively.
Since pregnancy and childbirth cause hormonal changes, fertility was thought to have affected the changes in the fibroid and adenomyosis. In this study, the subjects who had given birth three times experienced the greatest treatment effects, and those who had given birth only once experienced the least treatment effects. The volume reductions according to fertility were statistically significant, but no statistically significant reduction rate result was obtained. The volume reductions according to the treatment duration were statistically insignificant; but as a result of ANOVA on the volume reduction rate, statistically significant results were obtained. What was unique about the treatment duration was that the subjects with 31-60 minutes and 121-150 minutes experienced lesser treatment effects three months later, but at six months post-operatively, they showed a greater reduction than the subjects with any other treatment duration. This study had the following limitations. Although some patients were followed up to 12 months after HIFU treatment, this study contains only short-term treatment (6months) effect. The discrimination based on the contrast-enhancement ultrasound using microbubbles might be more meaningful than the method used in this study. In the case of two or more fibroid or adenomyosis, only the largest one was used for the analysis of treatment effect. In addition, patients who underwent HIFU treatment only at a Hospital were targeted. In future studies, patients from various hospitals may be targeted. Considering the size of the benign uterine tumor, would be decreased up to 24 months after completion of HIFU treatment, a longer follow-up period might be needed. Next, HIFU can also cause complications but data related to HIFU complications were not collected in this study. For HIFU treatment, however, it is known that the general complications are as follows: subcutaneous edema can occur on the patient's skin. In addition, pain similar to that experienced due to a slight burn can occur. Although HIFU treatment does not cause bleeding because it is an extracorporeal treatment, it can cause damage to the surrounding organs (i.e., heart, stomach, and intestine). In cases of liver cancer, there is a low possibility of nerve damage. However, if nerves exist in adjacent regions like uterine myoma, some transitional disabilities have been reported. There is also the possibility of infection in the tissues with coagulation necrosis (12). In cases of uterine myoma, the follow-up observation of 7 pregnant women who experienced unplanned pregnancies showed that all women had a full term delivery and did not have any specific complications related to the pregnancy within 1 year (range: 5–32 weeks, average: 20 ± 8.85 weeks) after receiving HIFU treatment. Although it is considered safe for women to get pregnant 1 year after HIFU treatment, the need for a large-scale study on the topic has been mentioned (13). However, Bohlmann et al. (14) mentioned that there has yet to be any prospective research on the effects of HIFU treatment on pregnancy; therefore, they recommend that HIFU treatment be conducted selectively only for the following types of patients: patients at high risk of undergoing surgery, patients who refuse surgery, or infertile patients. Complications observed have been predominantly of Society of Interventional Radiology class A (no medical intervention required), with a small number of Society of Interventional Radiology class B (nominal therapy, no consequence). Class A adverse effects have included abdominal pain, mild sciatic/buttock pain, genital bleeding/increased discharge, and a prolonged next period (15). Zhang et al. (9) reported a slightly increased frequency of abdominal pain (64% vs 71%) and skin reaction (0.8/2.4%) in patients with diffuse adenomyosis compared with those with focal disease. In their recent large analysis of 346 cases, Lee et al. (10) reported a range of more unusual complications, including foot drop (one case), transient unilateral leg weakness (one case), tumor lysis syndrome with transient acute prerenal failure (one case), sleep apnea due to a sedative agent (one case), first degree skin burn (five cases), second degree skin burn (three cases), and transient hematuria (ten cases) (10). Research on HIFU complications is planned in the future.
HIFU is a relatively effective method of treating benign uterine tumors. It can be used for patients who cannot undergo the conventional surgical methods due to their poor medical condition. In conclusion, HIFU might replace existing methods of treating benign uterine tumors.
 XML Download
XML Download