

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Implant-based immediate breast reconstruction after skin sparing mastectomy has recently become an accepted approach for management of patients with breast cancer (1). However, there remains a clinical dilemma regarding implant-based immediate breast reconstruction as the indications for adjuvant radiotherapy are dependent on final pathology results after mastectomy. Thus, many patients can undergo radiotherapy after implant-based immediate breast reconstruction, and are ultimately faced with the prospect of capsular fibrosis and contracture.
The pathophysiology of radiotherapy-induced capsular fibrosis is similar to those of other fibrotic diseases (23). The incidence of identifiable capsular fibrosis and contracture in breast reconstruction patients who undergo radiotherapy is as high as 100 percent (4). Capsular fibrosis and contracture can lead to unnaturally shaped breasts, implant hardening, and pain in severe cases. Therefore, less morbid and non-invasive treatment methods are required for prevention of capsular fibrosis, and, set against this background, pharmacologic inhibition of inflammation around implants offers a promising strategy (56).
Periprosthetic capsular tissues contain elevated levels of transforming growth factor (TGF)-β, which plays a central role in development of tissue fibrosis by activating inflammatory cells and fibroblasts in irradiated and non-irradiated breasts (78). Recent experimental evidence obtained using various models of fibrosis show that statins, well known lipid lowering agents, have anti-inflammatory and anti-fibrotic properties which are due to the inhibition of a downstream mediator of TGF-β (910).
In this study, we investigated the protective effect of simvastatin, a member of the statin group, on radiation-induced periprosthetic capsular fibrosis and the potential therapeutic value of simvastatin for prevention of capsular contracture.
MATERIALS AND METHODS
Animal preparation
All applicable institutional and/or national guidelines for the care and use of animals were followed. Eighteen male Sprague-Dawley rats weighing 250 to 300 g were used and maintained in a university vivarium. Animals were randomly divided into an experimental group (9 rats, 18 implants) and a control group (9 rats, 18 implants). Simvastatin (15 mg/kg/day, Hanmi Pharm Co., Seoul, Korea) was administered by oral gavage in the experimental group from 1 week prior to surgery until the end of the experiments. The control group received pure water. All rats had free access to standard rat chow and were housed in individual cages and maintained at 21 ± 2°C and a 12-hour light/12-hour dark cycle (light on 7 AM to 7 PM).
We used 36 custom-made miniature silicone implants, which were smooth-surfaced hemispheres 10 mm in diameter, crafted especially for the experiment and sterilized (SUN MEDICAL Co., Uiwang, Korea).
Surgical procedures
Rats were anesthetized with ketamine (60 mg/kg) and xylazine (4 mg/kg) and prepared using iodine solution. A 15 mm transverse incision was made on the middle third of the back involving skin and panniculus carnosus. Two pockets of 10 mm by 10 mm in size were made beneath the panniculus carnosus on the left and right sides of the back, while taking care to achieve hemostasis. An implant was then inserted into each pocket. The incision was then closed with interrupted monofilament sutures. General and wound check-ups were performed daily throughout the experiment.
After 12 weeks, rats were euthanized using a carbon dioxide inhalation and implant and all tissues surrounding implants were harvested in one piece.
Radiation protocol
The day following implant insertion, rats in both groups were anesthetized and a directed 10 Gy dose of radiation was administered to both sides from a clinical accelerator (Clinac 21EX; Varian Medical Systems, Palo Alto, CA, USA). The photon beam radiation was targeted at implants to induce capsular fibrosis and minimize systemic effects.
Histologic analysis
Harvested specimens were fixed in phosphate-buffered 10% formaldehyde, embedded in paraffin, cut into 5 μm sections, and stained with Masson trichrome. The stained sections were examined under an optical microscope (Nikon Eclipse 80i; Nikon Corp., Tokyo, Japan) equipped with a digital camera (ProgRes C14 Plus digital camera; JENOPTIK, Jena, Germany). Capsular thickness was determined as average values of measured 5 different locations per specimen. Fibrosis ratio was calculated by O'Brien method using a computer-assisted automated image analyzer (Image-pro Plus; Media Cybernetics Inc., Rockville, MD, USA) (11).
Real-time PCR analysis
Tissues were homogenized in Tri-solution (BSK-BIO, Daegu, Korea) using an Ultra-Turrax T25 instrument (IKA-Labortechnik, Staufel, Germany). RNA was reverse transcribed to cDNA from 1 μg of total RNA using a High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems, Foster City, CA, USA). Quantitative real-time PCR was performed using the Real-Time PCR 7500 system and Power SYBR Green PCR master mix (Applied Biosystems), according to the manufacturer's instructions. The expression level of GAPDH was used as an internal control. The reactions were incubated at 95°C for 10 minutes, followed by 45 cycles of 95°C for 15 seconds, 60°C for 20 seconds, and 72°C for 35 seconds. Primers for rat Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) (forward, 5'-TGATGACATCAAGAAGGTGGT-3'; reverse, 5'-TGCTGTTGAAGTCACAGGAGA-3'), TGF-β1 (forward, 5'-TGCTGACCCCCACTGATA-3'; reverse, 5'-GAAGCGAAAGCCCTGTATTC-3'), Connective tissue growth factor (CTGF) (forward, 5'-GGCCCAGACCCAACTATG-3'; reverse 5'-GTAACTCGGGTGGAGATGC-3') were designed using the Primer Express program (Applied Biosystems). The relative quantifications of the mRNAs of interest were performed by normalizing their amplification signals versus GAPDH (∆Ct). Relative quantification values were calculated using the 2-∆∆Ct method.
RESULTS
Histologic evaluation
The average capsular thickness was 371.2 μm in the simvastatin group, compared with 491.2 μm in the control group. This difference was not statistically significant (P = 0.381). The collagen fibers of the capsule in the simvastatin group showed a loose pattern and fibers in the control group showed a dense collagen pattern (Fig. 1). The fibrosis ratio was significantly different, with 32.33% ± 10.38% in the simvastatin group and 58.44% ± 15.69% in the control group (P < 0.001; Fig. 2).
Fig. 1
Capsules were Masson trichrome stained and imaged at 40 × (A, B) and 100 × (C, D). Representative histologic sections of capsular fibrosis from the control (A, C) and the simvastatin groups (B, D). The collagen fibers of capsule showed a dense parallel pattern in the control group and a loose pattern in the simvastatin group. The bidirectional arrow shows capsule thickness; scale bar, 1,000 μm.

Real-time PCR analysis evaluation
The effect of simvastatin on the gene expression of CTGF and TGF-β1 in capsules was examined by real-time quantitative PCR. CTGF gene expression was 1.9 fold higher in the control group (0.90 ± 0.16) than in the simvastatin group (0.46 ± 0.15), and TGF-β1 gene expression was 2.0 fold higher in the control group (1.00 ± 0.24) than in the simvastatin group (0.50 ± 0.16). Based on these observations, CTGF and TGF-β1 gene expression decreased significantly in the simvastatin group compared to the control group (P < 0.001; Fig. 3).
Fig. 3
Quantitative analysis by real-time PCR showed that CTGF gene expression in the simvastatin group (0.46 ± 0.15) decreased significantly compared to the control group (0.90 ± 0.16) (P < 0.001, A). TGF-β1 gene expression in the simvastatin group (0.50 ± 0.16) decreased significantly compared to the control group (1.00 ± 0.24) (P < 0.001, B).

DISCUSSION
In this study, we hypothesized that because simvastatin has anti-fibrotic effects, it could be used to reduce radiation induced capsular fibrosis. As hypothesized, capsular fibrosis was reduced in simvastatin treated rats, as indicated by fibrous ratio and mRNA expression of CTGF and TGF-β1. These findings suggest that simvastatin down-regulates the production of fibrogenic cytokines, thus reducing periprosthetic fibrosis. Lower values of capsular thickness were also shown in simvastatin treated rats. However, no significant difference in capsular thickness was observed between two groups. We suggest that there are a few possible reasons for this. First, because the capsule is a three dimensional structure, variation of capsular thickness may occur according to the cutting angle of the section. In other words, capsular thickness is a one-dimensional measurement. Second, collagen pattern may affect capsular thickness. Loose collagen layers observed in the simvastatin group may increase capsular thickness more than dense collagen layers observed in the control group. Another possibility is that the capsular thickness may differ according to the period for the surface of implant and postop (12). Finally, simvastatin could have an effect on the parenchymal thickness, and it is possible that capsular fibrosis ratio is changed.
Simvastatin, a 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitor, catalyzes the rate-limiting step of the cholesterol synthesis pathway in liver and other tissues, thereby reducing cholesterol levels and improving serum lipid profiles. In recent years, simvastatin has also been found to have pleiotropic effects, including immunomodulatory and anti-inflammatory effects (1314).
TGF-β1 plays a central role in development of tissue fibrosis including periprosthetic capsular formation by activation of inflammatory cells and fibroblasts (15). It is one of the most widely studied cytokines in the context of radiation-induced injury. This radiation injury is triggered by a cascade of cytokine activations, beginning with the early activation of an inflammatory process, and TGF-β1 acts as the master switch for this cascade (1617). Katzel et al. (818), who introduced a Smad3 knockout mouse model to study capsular contracture using a 10 Gy induction dose, found that radiation-induced prosthetic capsular formation was prevented by inhibiting TGF-β1 signaling.
CTGF, a potent profibrotic mediator, acts downstream of and in concert with TGF-β1 to drive fibrogenesis. CTGF also shares some of the biological actions of TGF-β1, including stimulation of cell proliferation and extracellular matrix protein synthesis by fibroblasts. However, unlike TGF-β1, CTGF does not have a growth inhibitory effect on epithelial cells. Mazaheri et al. (19), who studied the role of CTGF during prosthetic capsular formation, suggested that CTGF might be a more desirable pharmacological target than TGF-β1 for blockade of capsular formation after prosthetic breast surgery.
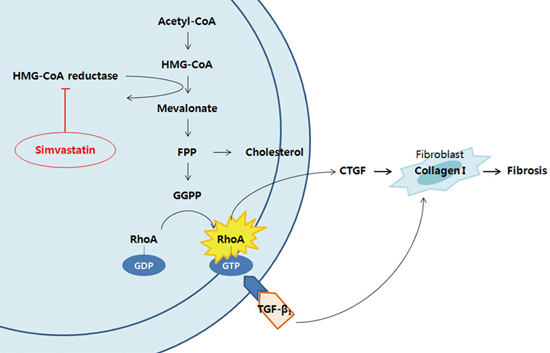
Several studies have demonstrated that HMG-CoA reductase inhibitors reduce CTGF expression and its induction by TGF-β1 via a RhoA signaling pathway during tissue fibrosis (2021). This pathway is known to play important roles in inflammatory and fibrotic responses, and to involve the depletion of cellular pools of isoprenoid intermediates, such as farnesyl pyrophosphate (FPP) and geranylgeranyl pyrophosphate (GGPP), by HMG-CoA reductase inhibitors. Isoprenoid intermediates are important lipid attachments for the posttranslational modification of RhoA, which enables binding of RhoA to the cell membrane and exertion of its signaling activities. Therefore HMG-CoA reductase inhibitors contribute to the inhibition of the pleiotropic RhoA signaling pathway related to inflammation and fibrosis (Fig. 4).
Fig. 4
Intracellular mechanism of the inhibition of RhoA signaling by simvastatin. Simvastatin inhibits HMG-CoA reductase, thus, depleting the cellular pool of isoprene precursor molecules, such as FPP and GGPP. Isoprene precursor molecules are required for the prenylation of RhoA GTPase. Subsequent loss of RhoA signaling activity blocks the production of CTGF, which is required for fibrosis.
CoA, coenzyme A; HMG, 3-hydroxy-3-methylglutaryl; FPP, farnesyl pyrophosphate; GGPP, geranylgeranyl pyrophosphate; GDP, guanosine 5'-diphosphate; GTP, guanosine 5'-triphosphate.

The use of simvastatin for prevention or treatment of periprosthetic capsular formation is a promising concept, however many questions remain unanswered. One question is in regard to determination of the optimum therapeutic dose required to achieve a therapeutic effect without adverse effects. The most common adverse effects of statins are elevated liver enzymes and muscle problems (22), and a recent meta-analysis suggested an association of statins with an increased rate of developing new onset diabetes (23). In a study with a large number of patients, simvastatin-treated group showed more clinically significant elevations in aminotransferases than placebo-treated group (24). Dose-dependent adverse effects on the liver tests were observed and occurred mainly within the first year after the initiation of therapy. Simvastatin has been associated with liver injury, such as acute hepatitis, cholestatic hepatitis, and acute liver failure (2526). Therefore, it is recommended that liver function tests be performed before the initiation of therapy and at follow-up period in patients on simvastatin therapy.
With regard to dosage, Ou et al. (27) reported that at daily oral dose of 5 and 20 mg/kg, simvastatin successfully attenuated bleomycin-induced pulmonary fibrosis in rats. On the other hands, Hsieh et al. (28) reported that simvastatin failed to reduce inflammation in the periprosthetic capsular tissues of rats at an oral concentration of 2mg/kg/day. Although 15 mg/kg/day of oral simvastatin inhibited capsular formation in the current animal study, optimal dosages that do not cause unwanted adverse effects remain to be determined in human clinical studies.
The limitation and the possibility for additional study in the future are as follows. First, the following assessments can be included as a test for contracture: capsule collagen density, myofibroblast distribution, and tensile strength. In addition, with a greater number of animal experiments, capsular thickness with statistical significance may be obtained.
The current study showed that simvastatin can attenuate radiation-induced capsular fibrosis around silicone implants in a rat model. These findings suggest an alternative therapeutic strategy for reducing capsular formation after expander or implant breast reconstruction in irradiated fields.
 XML Download
XML Download