

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Transurethral resection (TUR) has been the gold standard in the operative management of benign prostatic hyperplasia and bladder tumor; however, it is associated with several complications that may cause patient discomfort. Among them, early complications including urgency induced by indwelling Foley catheter and postoperative hemorrhage are issues of concern for anesthesiologists and urologists. Catheter-induced bladder discomfort is frequently related to emergence agitation. It can worsen the quality of anesthesia and may also cause unintended patient movement such as pulling on the catheter, which can lead to injury to the patient during the perioperative period. Furthermore, emergence in light anesthesia is often related to increased sympathetic tone, which can be detrimental in patients undergoing TUR who have a high prevalence of hypertension (1), because emergence agitation induced by urinary catheter together with elevated sympathetic activity can promote postoperative bleeding of the surgical site and lead to a clot in the urinary tract, which may require a change of urinary catheter or reoperation.
Various approaches, including dexmedetomidine, have been tested for prevention of emergence agitation but there have been no reports evaluating the effect of dexmedetomidine in decreasing emergence agitation primarily caused by bladder discomfort in patients undergoing TUR.
Dexmedetomidine, a highly selective and potent alpha-2 adrenergic agonist, is well known for its advantageous effects that include anxiolysis, analgesia, anesthetic-sparing, and sympatholytic properties with minimal respiratory depression (2). Based on these properties, dexmedetomidine is considered useful as a medication for relieving anxiety and providing hemodynamic stability in patients at risk from emergence agitation and increased sympathetic tone related to catheter-induced bladder discomfort.
The aim of this study was to evaluate the effect of continuous infusion of dexmedetomidine after administration of a loading dose on emergence agitation, hemodynamic status, and recovery profiles in patients undergoing elective TUR.
MATERIALS AND METHODS
Patient characteristics
All patients provided written informed consent. Sixty male patients aged 30 to 80 yr with American Society of Anesthesiologists status I or II who were scheduled for elective TUR under general anesthesia were included in this study. Patients with severe cardiovascular, neurologic, renal, or hepatic disorders, and those who were taking psychoactive drugs were excluded. Participants were randomly assigned to two groups (control group, group C; dexmedetomidine group, group D).
Methods
Premedication was not administered. Upon arrival in the operating room, standard monitors including electrocardiogram, non-invasive blood pressure, bispectral index (BIS), pulse oximeter, and capnogram were connected and baseline values were recorded. Anesthesia was induced with 2.0 mg/kg of 1% propofol and 0.6 mg/kg of rocuronium. After insertion of a tracheal tube, desflurane in 50% nitrous oxide and oxygen was used to maintain anesthesia and was adjusted continuously to maintain a BIS value between 40 and 60. Additional rocuronium (0.15 mg/kg) was used if neuromuscular relaxation was inadequate. Patients were mechanically ventilated to maintain end tidal carbon dioxide partial pressure of 30-40 mmHg. Simultaneously with the induction of anesthesia, a loading dose of 0.5 µg/kg dexmedetomidine diluted with isotonic saline for group D, or an equal volume of isotonic saline for group C, was slowly administered intravenously over 5 min. Subsequently, a continuous infusion of dexmedetomidine (0.5 µg/kg/hr) or the equal amount of isotonic saline was administered to groups D and C respectively. Five minutes prior to the end of surgery, the neuromuscular blockade was reversed with intravenous 0.2 mg/kg pyridostigmine. At completion of surgery, all anesthetics and study drugs were discontinued. After confirming appropriate spontaneous breathing, the tracheal tube was removed from the trachea. Perioperative hemodynamic instabilities including bradycardia (heart rate slower than 50 beats/min) and hypotension (systolic blood pressure [SBP] lower than 80 mmHg) were managed with 10 mg ephedrine. If the patient presented postoperative nausea and vomiting (PONV) during emergence, a rescue anti-emetic drug (4 mg ondansetron) was given.
Assessment
Demographic data including age, gender, weight, height, and duration of anesthesia were recorded. Oxygen saturation and hemodynamic variables such as heart rate, SBP, and diastolic blood pressure (DBP) were monitored every 5 min in all patients during anesthesia and recorded at four time points before the end of anesthesia: baseline (T1), induction of anesthesia (T2), beginning of surgery (T3), and discontinuation of anesthetics (T4). After anesthesia, these data were monitored every 10 min over 30 min and recorded at the following times: arrival at post-anesthetic care unit (PACU; P1), 10 min after arrival at PACU (P2), 20 min after arrival at PACU (P3), and 30 min after arrival at PACU (P4). Side effects including PONV, hypotension, or bradycardia and the use of rescue drugs were recorded. The need for airway assistance to improve oxygen desaturation, and reoperation for bleeding control was also recorded.
Recovery profiles including the recovery time (time interval from the cessation of anesthetics to eye opening in response to verbal command), the discharge time (time interval from arrival at PACU to discharge of patient from the PACU), and emergence agitation were recorded. Discharge of the patient was permitted when the Aldrete recovery score reached 9 (3). Emergence agitation was evaluated according to the 4-point agitation score as follows: 1=calm; 2=slightly agitated but consolable; 3=moderately agitated and inconsolable; 4=severely agitated and highly inconsolable (4). A score greater than 3 was defined as an agitated state. Catheter-induced bladder discomfort was assessed by a 3-point scoring system as follows: 1=comfortable, 2=uncomfortable but bearable, and 3=severely uncomfortable.
Statistical analysis
Assuming that dexmedetomidine would reduce the incidence of catheter induced emergence agitation by 37%, we calculated that the number of patients required for each group was 28 for a level of significance of 0.05 and a power of 0.8. To make allowance for unexpected dropout, thirty patients were recruited for each group. Statistical analysis was performed using the SPSS (version 21; SPSS Inc., Chicago, IL, USA). Data are expressed as means±SD. Numerical variables (age, gender, weight, height, duration of anesthesia, recovery time, discharge time) were analyzed with Student's t-test. Nominal variables (emergence agitation, bladder discomfort, side effects) were compared using the chi-square test. Changes in blood pressure and heart rate between two groups were analyzed by repeated measures ANOVA. A P value<0.05 was considered statistically significant. The statistical analyses performed in this study were advised by the Catholic Medical Center Clinical Research Coordinating Center.
RESULTS
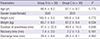
A total of 60 male patients were enrolled in this study and randomly assigned to group C (n=30) or group D (n=30). Demographic data and duration of anesthesia were not significantly different between the two groups (Table 1).
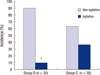
There were no significant differences between the two groups in terms of recovery profiles including recovery time and discharge time (Table 1); however, the quality of emergence in group D was marked by a significantly lower incidence of emergence agitation than in group C (P=0.015) (Fig. 1). The number of patients that presented agitation was 3 (10%) in group D compared with 11 (36.7%) in group C. The agitation scores of both groups are given in Fig. 2. Agitation scores of 1, 2, and 3 were observed in 14 (46.7%), 13 (43.3%), and 3 (10%) patients in group D and 5 (16.7%), 14 (46.7%), and 9 (30%) patients in group C, respectively. No patients in group D reached an agitation score of 4, whereas 2 (6.7%) patients in group C had an agitation score of 4. Fig. 3 shows the intensity of bladder discomfort in both groups. In group D, 16 (53.3%), 13 (43.3%), and 1 (3.3%) patient felt a degree of discomfort of 1, 2, and 3 compared with 7 (23.3%), 17 (56.7%), and 6 (20.0%) patients in group C, respectively. Patients in group D therefore felt less discomfort induced by the indwelling Foley catheter than those in group C (P=0.022).
Changes in intraoperative (T1-T4) and postoperative (P1-P3) SBP, DBP, and heart rate are given in Fig. 4. The hemodynamic variables at T1 and T2 were similar between the two groups, but patients in group D presented significantly lower systolic, diastolic pressures, and heart rate at T3, T4, and P1-P3 than those in group C, respectively. Overall hemodynamic changes over time demonstrated significantly lower systolic (P<0.001) and diastolic blood pressures (P=0.001) and heart rate (P=0.005) in group D compared to group C.
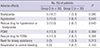
No statistically significant differences were found between the two groups with respect to side effects including bradycardia (P=0.085), hypotension (P=0.640), and PONV (P=0.389) in PACU (Table 2). There was also no significant difference in use of rescue drugs for bradycardia, hypotension (P=0.640), or PONV (P=0.389) between the two groups. The requirement for airway assistance to improve oxygenation was not also significantly different between the groups (P=0.313). Although 2 patients (6.7%) in group C underwent reoperation for bleeding control, there was no statistical difference between the two groups (P=0.150).
DISCUSSION
This study demonstrates that continuous infusion of dexmedetomidine after a loading dose significantly reduces the incidence and severity of emergence agitation and alleviates catheter-induced bladder discomfort without serious complications in patients undergoing TUR. Postoperative bladder discomfort derived from a urinary catheter can be distressing and frequently leads to emergence agitation. Catheter-induced irritation shares symptoms such as urgency and frequency with overactive bladder, which is characterized by an involuntary bladder contraction. Regulation of bladder contraction is considered to be associated with several neurotransmitters including acetylcholine, noradrenaline, adenosine triphosphate, and nitric oxide (5), however, it is widely accepted that bladder contraction is mainly mediated by cholinergic receptors (6). Therefore anti-muscarinic drugs have been the mainstay of pharmacological therapy for overactive bladder. However, treatment with anti-muscarinic drugs is restricted by their diverse efficacy and well-known side effects such as dry mouth, which may lead to lack of patient compliance and interruption of medication (78).
Dexmedetomidine is an alpha-2 adrenergic receptor agonist with an 8 times greater affinity than clonidine. It exhibits sedative, anxiolytic, and analgesic properties by inhibiting the release of nor-epinephrine mediated through alpha-2 adrenergic receptors in the locus ceruleus and spinal cord (9). Moreover, it does not produce respiratory depression or oversedation through accumulation, unlike other commonly used sedatives such as propofol or midazolam. Therefore, dexmedetomidine has been used not only as an ideal short-term sedative agent for mechanically ventilated patients in the intensive care unit, but also for a smooth conversion from anesthesia to sedation (10) or prevention of emergence agitation (11).
The overall incidence of emergence agitation in previous studies varies from 16.1% to 64% (111213) according to age and gender, while our result (37%) slightly exceed the previous data of male adult (28.1%). In the present study, we demonstrated that dexmedetomidine decreases emergence agitation. The incidence of emergence agitation was decreased by 72.7% in group D compared to group C, which is consistent with previous studies (1112). As predicted, catheter-induced bladder discomfort was less intense in group D compared to group C. The incidence of bladder discomfort was also reduced by 39.1% in group D of this study, which is as effective as previously reported various pharmacological attempts (1415). It should be noted that the sedative property of dexmedetomidine could be considered a disadvantage as it may prolong the time to awake from anesthesia. However, previous studies have presented various outcomes in this regard. Guler et al. (12) and Kim et al. (16) reported that the time to removal of endotracheal tube or laryngeal mask airway was significantly prolonged in the dexmedetomidine group compared to the control group while it was noted that a single dosage of dexmedetomidine had little influence on the emergence time in comparison with placebo (17). In the present study, the recovery time of group D showed a wide range from 3 to 11 min, compared with 4 to 10 min in group C. Since quite a large number of patients (24 of 60) were discharged from PACU less than 30 min after their arrival at PACU, the time point (P4) that was planned when setting up the research plan was excluded. Furthermore, two patients in group C left PACU 15 min after arrival at the PACU. Nonetheless, there were no significant differences in recovery time and discharge time between the two groups. The anesthetic-sparing effect and unique sedative properties of dexmedetomidine may account for this result. The distinct property of dexmedetomidine as a sedative offers easy arousability and rapid falling asleep similar to natural sleep; these characteristics are not shared with other sedatives (18). Furthermore, Venn et al. (19) reported that a high dose of dexmedetomidine paradoxically has a favorable influence on fast awakening owing to its anesthetic-sparing effect.
Dexmedetomidine provides notable hemodynamic stability through the inhibition of central sympathetic outflow. In fact, the hemodynamic changes vary with the dose or rate of infusion of dexmedetomidine (20), which can produce transient hypertension at higher doses although it mostly causes hypotension and bradycardia. In the present study, initial hypertension at the beginning of infusion was not observed, which can be explained by the relatively low loading dose and the offsetting vasodilating effect of propofol. The hemodynamic variables at T1 and T2 were similar between the two groups, but patients in group D had significantly lower SBP, DBP, and heart rate at the other time points (T3-P3) than those in group C. Adverse hemodynamic outcomes including bradycardia and hypotension occurred more frequently in group D compared with group C, although there was no significant difference between the groups. There was also no statistically significant difference in the need for rescue drugs for bradycardia or hypotension. Five patients in group D experienced bradycardia; the heart rates of two patients were spontaneously restored, and the others were given rescue drugs since they also exhibited hypotension. The severity of hemodynamic side effects was not great enough to decrease the lowest heart rate to 40 beats per minute, and additional second doses of the rescue drug were not necessary in any of the patients. However, meticulous caution should be applied for patients who are considered to have increased vagal tone, advanced heart block, or severe ventricular dysfunction preoperatively because dexmedetomidine can sometimes induce severe bradycardia leading to asystole (21).
Previous studies have reported that dexmedetomidine has a beneficial effect in decreasing PONV (22) although PONV is actually listed in the index of adverse effects of dexmedetomidine (23). In the present study, the incidence of PONV was not significantly different between the two groups. The occurrence of adverse respiratory event was not significantly different between the two groups and the present study may support minimal respiratory depression by dexmedetomidine. While no patient in group D showed respiratory depression, one patient in group C presented hypoxemia in PACU that was improved shortly after applying Ambu-bag ventilation with 100% oxygen. This was probably caused by the combined effect of temporary bronchospasm and inadequate emergence from general anesthesia.
Controlled hypotension is necessary for patients undergoing TUR during the recovery period because they often experience hypertension and decreased cardiac reserve, which may induce perioperative cardiovascular side effects, in addition to its role in reducing postoperative bleeding. In the present study, 2 patients in group C had reoperation for bleeding control compared with none in group D, but there was no statistical difference in the need for reoperation between the two groups. The present study did not conclusively document the effectiveness of dexmedetomidine in decreasing the incidence of postoperative bleeding in patients undergoing TUR despite its effect in decreasing perioperative blood pressure. Further large studies are suggested to confirm this issue.
This study showed that intraoperative dexmedetomidine infusion following a bolus dose effectively reduced the incidence and intensity of emergence agitation and catheter-induced bladder discomfort without delaying recovery time and discharge time, thus providing smooth emergence during the recovery period in patients undergoing TUR. Intraoperative use of dexmedetomidine offers hemodynamic stability with well-controllable side effects that include bradycardia and hypotension. There was no evidence of adverse effects including PONV and respiratory depression in the patients who were given dexmedetomidine.
We conclude that dexmedetomidine may have advantages in preventing emergence agitation and catheter-induced bladder discomfort during recovery from anesthesia.



 XML Download
XML Download