

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lung cancer is one of the most common cause of cancer-related death worldwide (1). Its median survival for non-small cell lung cancer (NSCLC) is estimated to be 8 to 10 months, and 1-year survival to be only 30% to 35% with standard chemotherapeutic treatment (2345). Some of the NSCLCs have specific mutated oncogene which is considered to be the main genetic defect that leads to cancer (6). The two most commonly mutated oncogenes in lung cancer are epidermal growth factor receptor (EGFR) and Kirsten rat sarcoma viral oncogene homologue (KRAS) (6). EGFR has a pivotal role as a receptor tyrosine kinase, controls signal pathways that controls cell growth and proliferation. As a consequence, mutations in the kinase domain of EGFR gene (exons 18-21) strongly correlate with improved overall survival and disease-free survival in patients with NSCLC who receive the EGFR tyrosine kinase inhibitors erlotinib or gefitinib as treatment therapy (78). These mutations are commonly associated with never or non-smoker, adenocarcinomatous morphology, and Asian ethnicity (68). On the other hand, unlike those of EGFR mutant, KRAS mutations are usually found in those with significant smoking history (69). Moreover, KRAS mutations, which encodes a GTPase downstream of EGFR, are associated with primary resistance to tyrosine kinase inhibitors in patients with NSCLC, which appears to be mutually exclusive to EGFR mutations in NSCLC (69). Taken together, current evidence suggests that EGFR and KRAS mutations define distinct subgroups of NSCLC patients, with different responses to EGFR- targeted therapies.
In these backgrounds, testing for EGFR and KRAS mutations have now become a routine practice for therapeutic management (10). Sensitive, rapid, and at the same time, reliable methods for detecting these mutations are required for targeted treatment. Thus now, the most frequently used conventional method for detecting EGFR and KRAS mutations is considered to be direct DNA sequencing method (11). However, this technique has some limitation, including frequent interference of nonmalignant cells, and is not necessarily practical for clinical use with suboptimal sensitivity (1112). Pyrosequencing is a simple and accurate DNA sequencing technique based on detection of released pyrophosphate during DNA synthesis (13).
In the past, cytologic specimens have not been widely used for mutational sequence analysis due to sparse cellularity (12). But in recent years, cytology specimens are being more frequently used for mutational tests, especially when cytological materials are the only available tissues for molecular testing (14). Several studies reported that cytology specimens also yield comparative results similar to surgical specimens (51014). Overall, preservation and quality of the DNA extracted seemed to matter more than the actual number of tumor cells present in the samples. In a recent consensus for mutation testing in NSCLC, there was agreement that the quality of amplifiable DNA is more important than its quantity.
In this study, we aimed to evaluate the testing for EGFR and KRAS mutations by pyrosequencing method, and compared the yield of cytology versus histology specimens in a consecutive series of patients with NSCLC in Konkuk University Medical Center, Seoul, Korea.
MATERIALS AND METHODS
Patient selection
This retrospective study examined 446 patients who were diagnosed as lung cancer in Konkuk University Medical Center, Seoul, Korea from January, 2008 to September, 2014. The eligible criteria were as follows: a) patient who presented with lung mass and diagnosed as primary or metastatic cancer with the methods of cytology, biopsy, and excision, b) cases which EGFR and K-RAS mutation studies were done. We also included the specimens, such as lymph nodes, from the metastatic sites with primary lung cancer. According to the above criteria, total number of 399 and 323 patients who had EGFR and KRAS mutation tests were included in the study, respectively. Among them, 60 patients had received both EGFR and KRAS mutation studies.
Clinicopathological analysis
To evaluate the clinicopathologic features of the patients, medical records of 399 (patients who had EGFR mutation test) and 323 (patients who had KRAS mutation test) patients were reviewed including patient age, gender, history of smoking, pathologic diagnosis, and most importantly, the diagnostic methods.
The smoking history was determined according to pack years (py), and subdivided into current, ex-smoker, non-smoker. We defined current smoker as more than 10 py history, and ex-smoker who has smoked greater than 100 cigarettes in their lifetime, does not currently smoke, but used to smoke daily. Never smoker are defined as who have never smoked a cigarette or who smoked fewer than 100 cigarettes in their entire lifetime.
The subtypes of diagnostic methods are divided into three categories: Biopsy, Cytology, and Excision. In ‘Biopsy’ category, the specimens includes small biopsy specimen from bronchoscopic biopsy, transbronchial lung biopsy, percutaneous needle biopsy, pleural biopsy or needle biopsy from metastatic sites. The ‘Cytology’ includes the cytologic specimens from sputum, bronchial washing/brushing, pleural fluids, aspiration biopsy cytology of primary or metastatic sites. ‘Excision’ category includes specimens form excisional surgical biopsy such as segmentectomy, lobectomy, pneumonectomy and metastatectomy.
The pathologic diagnoses were made by individual pathologists. Diagnoses from biopsy specimens were reviewed by experienced lung pathologist, and classified according to the WHO classification (WSK). Adenocarcinoma subtypes were evaluated separately from non-adenocarcinomatous lesions, for it is well known that both EGFR and KRAS mutations have tendency to occur primarily in adenocarcinomatous subtype.
EGFR and KRAS mutation analysis – pyrosequencing method
In all the cytologic and histologic samples, target tumor rich areas were marked by microscopic examination of pathologists. The tumor cells were scraped from the archived slides after the coverglass and xylene were removed. Microdissections on both cytological and tissue slides were done with 26-guage needle. The DNA was extracted from the tumor cells by the following in order – 1) Transfer the collected cells to 30 µL DNA isolation buffer, 2) Add 0.3 µL (20 mg/mL) Proteinase K and vortex, 3) Incubate at 56°C until complete lysis is done, 4) Incubate at 100°C for 20 minutes, 5) Immediately centrifuge at 12,000 rpm for 10 minutes at 4°C, 6) Transfer supernatant (DNA) to a new tube. EGFR and K-RAS mutation were analyzed by pyrosequencing method.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA). Chi-square test and Fisher’s exact test were used to determine correlations between EGFR and K-RAS mutation status and clinicopathological parameters. A P value of < 0.05 was considered statistically significant.
RESULTS
EGFR mutations and clinicopathologic characteristics
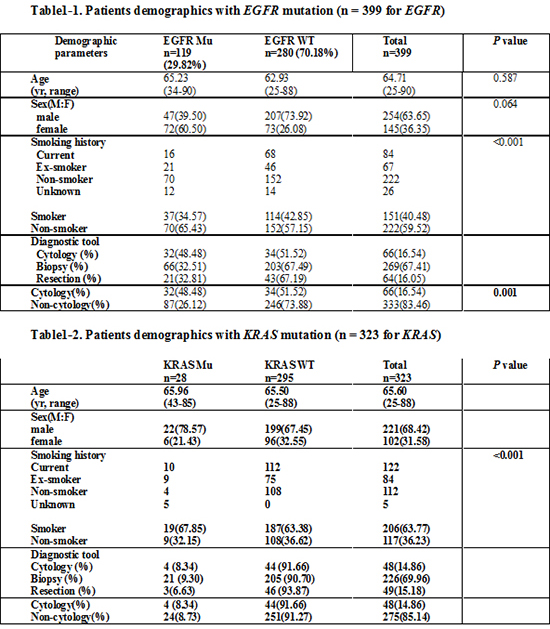
Of the 399 patients who had EGFR mutation test, 254 were male, and 105 were female (male:female = 254 [63.7%]:105 [36.3%]). The patient age ranged from 25 to 90 years old, with median age of 65.47 years. Among the three diagnostic tools, majority of cases (269, 67.4%) were biopsy specimen, followed by cytology specimens; 66 (16.5%), and resection specimens; 64 cases (16.1%).
Of them, 119 patients were positive for EGFR mutation (29.8%), and among them, 72 patients were female (60.5%, n = 72). Deletion in exon 19(E746 _A750) was the most frequently found mutation (48 cases, 40.3%), followed by L858R point mutations in exon 21 in 35 cases (29.4%). The detailed EGFR mutation profiles are summarized in Supplementary Table 1.
The EGFR mutation and smoking history showed strong inverse correlation (P < 0.001); 65% was non-smoker, and only 35% had history of smoking. The detection rates of EGFR mutation were highest in cytologic samples; 32 out of 66 samples (48.5%), resection specimens the 2nd highest; 21 of 43 (32.8%), and then biopsy specimens; 66 out of 269 (32.5%). As a result, cytology was more sensitive than non-cytology (histology) samples in detecting EGFR mutations (cytology: 48.5%, non-cytology: 26.1%). Table 1 summarizes the detailed information about patients who had EGFR mutation test.
Of the various histologic subtypes in 399 cases, adenocarcinoma was the most common subtype, being more than 70% of the whole samples (70.4%, 281 out of 399), followed by squamous cell carcinoma (n = 69), large cell carcinoma (n = 15), and small cell carcinoma (n = 12). In 281 adenocarcinoma cases, 111 cases were EGFR mutation positive (39.5%). Five of 69 squamous cell carcinoma were EGFR positive, and none of large cell and small cell carcinoma were EGFR positive. Among 119 EGFR mutation positive cases, 111 cases were diagnosed as adenocarcinoma. Five cases were squamous cell carcinoma, followed by 2 adenosquamous cell carcinoma, and 1 non-small cell carcinoma. The details about the EGFR mutation and the pathologic subtypes are shown in Table 2.
On the basis of the fact that EGFR mutations most frequently occur in adenocarcinoma, we compared the diagnostic yield of detecting adenocarcinoma in cytology, biopsy, and resection specimens. The proportion of adenocarcinoma was highest in cytology; being 59 out of 66 cases (89.4%), followed by resection; 52 out of 64 cases (81.3%), and biopsy; 173 out of 269 cases (64.3%). Table 3 shows more detailed information about the diagnostic tools and their pathologic subtypes.
KRAS mutations and clinicopathologic characteristics
Of the 323 patients who had received KRAS mutation test, 221 were male, and 102 were female (male:female = 68.4%:31.6%). The age of the patient ranged from 25 to 88 years old, with median age of 65.6 years. Similar to those of EGFR mutation tests, biopsy specimens were the most common, being 206 (63.8%). 49 (15.2%) and 48 (14.9%) samples were resection and cytology specimens, respectively.
A total of 28 of 323 patients were positive in KRAS mutation test (8.7%), and 22 were male, and 6 were female (male:female = 22 [78.6%]:6 [21.4%]). None of the 28 patients had EGFR mutation. Among the 28 KRAS mutation positive patients, 19 patients had smoking history (smoker:non-smoker = 19 [67.9%]:9 [32.1%]). Point mutations in codon 12 were most frequently observed mutation (18 cases, 5.6%), followed by mutation in codon 61 (7 cases, 2.2%). Mutation profiles of KRAS are summarized in Supplementary Table 1. Detection of KRAS mutation was highest in biopsy specimen; 21 of 226 (9.3%), followed by cytology; 4 of 48 (8.3%), and resection; 3 of 49 samples (6.6%). More information about patient data, smoking history and diagnostic tools of KRAS mutation are summarized in Table 1.
The most common histologic subtype was adenocarcinoma (74.0%, 211 of 289 cases), followed by squamous cell carcinoma (22.1%, 64 cases), large cell carcinoma (4.5%, 13 cases), and small cell carcinoma (4.15%, 12 cases). Among 28 KRAS positive cases, 23 cases were adenocarcinoma, 3 were squamous cell carcinoma. Detection of adenocarcinoma was highest in resection specimen (85.7%, 42 of 49 cases). The association of diagnostic tools of KRAS mutation and histologic subtypes Table 4.
EGFR and KRAS mutations in non-smokers
It is well-known that EGFR mutation is more frequent in non-smoker, whereas KRAS mutation strongly correlates with smoking history. We investigated the correlation between the smoking history and mutation rates according to diagnostic tools. As expected, EGFR mutations were detected more frequently non-smokers in all three types of specimens (cytology, 53.1% [17 of all 32 mutation positive cases]; biopsy, 62.7% [37 of 59 cases]; resection, 80% [16 of 20 cases]). Details about the mutational status according to the diagnostic tools in non-smokers are summarized in Table 5.
DISCUSSION
Pyrosequencing is a non-electrophoretic, real-time, nucleotide extension sequencing method using luminometric detection (15161718). It is based on the transformation of pyrophosphate. Briefly, pyrophosphate is released when the nucleotide anneals to template and the primer extends. Subsequently, the released pyrophosphate is converted to adenosine triphosphate, which is utilized to produce light (1517). Pyrosequencing is being increasingly used in various conditions, such as bacterial strain typing, mutation detection, SNP genotyping, and quantitative CpG island methylation analysis (15192021222324).
There are various and newly developed techniques for detecting mutations in lung cancer such as Amplification Refractory Mutation System (ARMS), cationic conjugated polymer-based fluorescence resonance energy transfer (CCP-RFLP), Smart Amplification Process (SmartAMP), pyrosequencing, etc (24). Standard method for detecting mutation of EGFR or KRAS is still direct DNA sequencing method. But, pyrosequencing has more advantages than conventional sequencing method, in that pyrosequencing is more sensitive, saves time, and cost-effective (1115161718). Recently, some studies have been reported to show efficacy of detecting EGFR and KRAS mutations by pyrosequencing methods (1117252627). However, most of these studies had performed only either one of EGFR or KRAS mutation testing by pyrosequencing, not both at the same time. Two previous reported studies have reported the usefulness of pyrosequencing in EGFR, KRAS, and BRAF mutations, but these studies were not solely done on lung carcinoma cases, and mainly focused on introducing new methodology with no available patient’s clinical data (2526).
The present study was performed with a large number of lung cancer patients (399 and 323 patients) in a single institution in Korea which shows both clinicopathologic characteristics and EGFR and KRAS mutation results by pyrosequencing. According to a nation-wide study of EGFR mutations in Korean patients, the overall EGFR mutation rate was 34.3% in patients with NSCLC and 43.3% in patients with adenocarcinoma (28). In our study, EGFR mutations were detected in 30.7% of NSCLC and in 39.8% of adenocarcinoma. Although, we did not compare pyrosequencing with other methods, pyrosequencing method is sensitive in detecting both EGFR and KRAS mutations. Similar to previous reports, EGFR mutations were prevalent in non-smokers (65.43%, P < 0.001), whereas KRAS mutations were common in smokers (67.85%, P < 0.001), and the two mutations are mutually exclusive in our study (6782529).
The utility of cytology samples in detecting mutations in lung cancer have recently been increased and relatively widely investigated (8303132). Cytology samples are especially useful in advanced lung cancer patients, when it is difficult to obtain tissue samples. In the present study, we compared the detection rates of both EGFR and KRAS mutations in cytology, biopsy and resection specimens. The detection rate of EGFR mutation in cytology was higher than non-cytology (biopsy or resection) materials (cytology: 48.48%, non-cytology: 26.12% [biopsy: 32.51%, resection: 32.81%]). Detection rate of KRAS mutation by cytology was comparable to non-cytology specimens as well (cytology: 8.34%, non-cytology: 8.73% [biopsy: 9.30%, resection: 6.63%]).
The present study showed that cytology specimens are comparable, or even better than non-cytology specimens, in detecting both EGFR and KRAS mutations. Cytology specimens are easier to obtain then tissue samples for several factors. First, lung biopsy is a very complicated process that requires both good patient condition and physician’s technique. Many lung cancer patients have no specific symptoms until they develop into advanced stage, when the general condition of the patients is not good for lung biopsy. Moreover, in many cases, FFPE specimens are small, and contain many non-tumorous components, such as non-neoplastic lung parenchyma, fibrous tissue, or inflammatory cells, and could yield false negative results in mutation tests (833).
Detecting EGFR and KRAS mutations are crucial for treatment of non-small cell lung cancer patients, especially for advanced-stage patients who do not have many treatment options. In many cases, cytology specimens could be the only available samples for diagnostic or therapeutic approach. In conclusion, we suggest that cytology specimens are good alternatives that can readily substitute tissue samples for testing both EGFR and KRAS mutations. Moreover, pyrosequencing method is highly sensitive in detecting EGFR and KRAS mutations in lung cancer patients.




 XML Download
XML Download