

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Glioblastoma (GBM) is the most aggressive diffuse glioma of the astrocytic lineage and corresponds to grade IV according to the WHO classification (1). It is also the most frequently diagnosed brain tumor, accounting for 45.2% of primary malignant brain tumors, 54% of all gliomas, and 16% of all primary brain tumors (2). GBM comprises of primary and secondary subtypes, which evolve through different genetic pathways, affect patients at different ages, and have different survival rates (3).
GBMs can have aberrant expression of different growth-control genes and their proteins, including impaired alpha thalassemia/mental retardation syndrome X-linked (ATRX) expression (ATRX-), p53 overexpression (p53+), and mutant IDH1 (H09) expression (IDH1+). Previous studies have shown that in unselected GBMs, IDH mutations were found in approximately 8.8% of the patients (4). Selectively, IDH mutations were detected in almost 90% of secondary GBM, whereas these mutations are uncommon in primary GBM (5). Moreover, IDH mutations are established markers of better prognosis in GBM (678). Mutations in p53 have been found in approximately 60% patients with secondary and 25% with primary GBMs (6910). Association of TP53 mutations with survival outcome in GBM patients has not been consistent; some studies reported better survival in patients with TP53 mutations (1112) while others have failed to find such association (13). ATRX is frequently mutated in secondary (57%) but rarely in primary GBMs (111415). In GBMs, ATRX mutations are usually accompanied by IDH and TP53 mutations (14). ATRX enables the incorporation of the histone variant H3.3 into the heterochromatin, giving rise to changes in telomere length and genomic instability (1617). Mutations of ATRX are still under study to determine its association with survival outcome in GBM patients and to establish these mutations as prognostic factors.
Therefore, the aims of our study were to determine the protein expression signatures of important growth-control genes, i.e., IDH1, p53, and ATRX, in our cohort of GBMs, and to determine whether in GBM altered protein expression of any of these growth-control genes, or their combined variants, were associated with significant increase in patient survival and, thereby, to establish prognostically distinct molecular subgroups of GBM irrespective of the histopathological diagnosis.
MATERIALS AND METHODS
Patient population and tissue microarray
A cohort of 163 patients diagnosed with GBM, who underwent surgery and were treated at Seoul National University Hospital (SNUH) in Korea between 1999 and 2011, were enrolled in this study, which had full medical history, survival data, enough formalin fixed paraffin embedded tissues (FFPE) for tissue microarray (TMA) and definite diagnosis of grade IV astrocytoma with microvascular proliferation and/or necrosis. Median age of our cohort was 49.4 years old (21-79 years old) and male to female ratio was 1.4:1. Archived slides and paraffin blocks for all the cases were obtained from the Department of Pathology, SNUH. Immunohistochemistry were carried out on TMA. Archival hematoxylin and eosin (H & E) stained slides were re-evaluated to determine the diagnostic accuracy and representative tumor regions for inclusion in the TMA. An average of 3-mm cores were cut from FFPE tissue blocks. If the cores of TMA were not representative or the results were not convincing due to losses of large part of core tissue during processing or squeezing artifact of tumor cells or extensive tumor cell necrosis seen in selected areas for TMA blocks, an entire sections from the other blocks were immunostained and re-analyzed. The clinical and survival data of the patients were obtained from the SNUH online portal.
Histological evaluation
Histological evaluation was performed on H & E stained archival slides from 163 cases. All cases were reviewed by the neuropathologists and confirmed as WHO grade IV astrocytomas according to the 2007 WHO classification scheme.
Immunohistochemical studies
Immunohistochemical staining was performed according to the manufacturer’s protocols using BenchMark XT (automated immunohistochemical slide staining system, Roche Diagnostics, IN, USA). Immunohistochemistry was performed on TMA sections using antibodies against ATRX (rabbit polyclonal, 1:600; Sigma-Aldrich, St. Louis, MO, USA), p53 (mouse monoclonal, Clone: DO-7, 1:50; Dako, Glostrup, Denmark), and IDH1 R132H mutant protein (mouse monoclonal, clone H09, 1:50; Dianova, Hamburg, Germany). Positive and negative controls were included in all TMAs. Sections from known mutation-positive and immunoreactive GBM tumors were used as positive controls. Negative controls consisted of sections incubated with normal rabbit serum instead of the primary antibody. IDH1and ATRX were scored as positive or negative. p53 were scored using a four-tiered scale, namely the percentage of stained nuclei was quantified and grouped into one of the four classes: (-), < 10% of the nuclei stained indicating the absence of immunoreactivity; (l+), 10-30% of the nuclei stained; (2+), 30.1-50% of the nuclei stained; (3+), > 50% of the nuclei stained (121318). And 2+ and 3+ were regarded as positive. Immunoreactivity was performed using the Aperio ImageScope software with Nuclear v9 algorithm.
Statistical analysis
Survival analysis was performed using the Kaplan-Meier estimator and log-rank test to assess the significant association of immunopositive versus immunonegative ATRX, p53, and IDH1 proteins with overall survival (OS) and progression free survival (PFS) times in GBM patients. A P < 0.05 was considered statistically significant. Analyses were carried out using IBM SPSS Statistics software V22.0.
Ethics statement
Clinical data were obtained from Seoul National University Hospital (SNUH) online medical records in accordance with institutional review board (IRB)-approved protocols (1307-093-505). We used anonymized tissue microarray blocks (TMA) made from formalin fixed paraffin embedded tissues made before 2013 February when newly updated life and ethical law is operated and informed consent was waived.
RESULTS
Clinical dataset
The demographic and survival characteristics of the unselected GBM population are summarized in Table 1. The study population consisted of 163 adult patients with a median age at diagnosis of 49.4 years (Age range: adults 21-79 years). The cohort consisted of 95 males and 68 females (1.4:1). The results of median OS and PFS were analyzed according to aberrant protein expression status, as each or combinations of three proteins, in our cohort of GBM patients, (Table 2, 3, 4).
Table 1
Demographic summary of patient cohort with glioblastoma (GBM) in this study
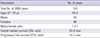
Table 2
The result of ATRX, IDH, and p53 immunoexpression in enrolled GBMs and median overall and progression free survivals in each subgroup
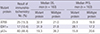
Table 3
Analysis of various combination of two proteins-pairs in adult GBMs and survival outcomes
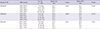
P value was obtained by log rank test of Kaplan Meier survival analysis.
IHC, immunohistochemistry; GBM, glioblastoma; OS, overall survival; PFS, progression free survival; ATRX-, loss of ATRX expression; ATRX+, positive ATRX protein expression; p53+, over-expression of p53; p53-, lack of p53 expression; IDH1+, Positive IDH1 protein; IDH1-, negative for mutated IDH1 (R132H) protein.
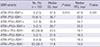
Table 4
Combined triple proteins of ATRX, p53, and IDH1 immunohistochemical results and survival outcomes
Immunohistochemical and survival analysis of GBMs with individual IDH1, ATRX and p53 protein expression, and patients’ age
Immunohistochemical characteristics of the enrolled GBM population are summarized in Table 2. From the overall study population, aberrant expression was observed in 25 GBMs (15.3%) for ATRX, 17 GBMs (10.4%) for IDH1, 80 GBMs (48.4%) for p53 (Fig. 1). The patients’ median OS and PFS in correlation with the aberrant protein expression are summarized in Table 2. In all patients each ATRX- and IDH1+ tumors showed the similarly excellent median OS of 32.9 and 31.9 months, and median PFS of 25.9 and 28.1 months, respectively, whereas the patients with p53-overexpressing tumors showed the worst median OS (19.3 months) and PFS (15.8 months). Kaplan Meier survival analysis showed statistically better OS and PFS in patients with GBMs with mutant protein expression of ATRX (ATRX-) and IDH1 (IDH1+) than the patients with GBMs with counterpart status of these two proteins (Fig. 2A-D). However, in case of p53 protein expression status, the better PFS was found in the patients with p53 negative GBMs, but OS was not correlated with P53 status (Fig. 2C and 2D). If the GBM patients stratified as two groups, younger and older age group, the p53 overexpressed tumors were correlated with poor OS (P = 0.014), however, in young age group under 45 years old, p53 overexpression did not affect the patients’ OS. The younger patients under 45 years old had statistically better OS (P = 0.011) than the older patients (≥ 45 years old), however, they had better tendency in PFS than older patients (P = 0.113) (Fig. 2E and 2F).
Fig. 1
The figures show representative pictures of one of GBMs and aberrant protein expression, that is, ATRX-/p53+/IDH1+, which are the least common combination of protein status, comprising 1.8% of our studied cohort. (A) H & E. (B) ATRX. (C) p53. (D) IDH1, (A-D) × 200.
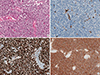
Fig. 2
Kaplan-Meier plots for GBM patient survival by ATRX, IDH and p53 protein expressions status. (A, B) The better survival (OS and PFS) is found in the patients with GBMs with positive IDH1 than the patients with lack of IDH1. (C, D) The better survival (OS and PFS) is noted in the patient with loss of ATRX expression than the patients with preserved ATRX expression. (E, F) The better survival with GBMs with lack of p53 overexpression has better PFS than the patients with GBMs with p53 overexpression, but OS is not statistically significant difference between the patients with p53 positive and negative GBMs. (G, H) Younger age patients (≤ 45 years old) have statistically significant better survival than the older GBM patients (> 45 years old).

Immunohistochemical and survival analysis of GBMs with combinations of two protein expression
Table 3 shows immunohistochemical results of two protein pairs, ATRX/IDH1, ATRX/p53, and IDH1/p53 and their median OS and PFS. In two protein pairs, the three largest combinations were ATRX+/IDH1- (78.5%), IDH1-/p53- (46.0%) and ATRX+/p53- (42.9%). However, ATRX+/p53+ and IDH1-/p53+ combination was also similarly high (41.7% and 43.6%, respectively). The three smallest subgroups were ATRX-/DH1+ (4.3%), ATRX-/p53+ (6.7%), and IDH1+/p53+ (4.9%).
By analyzing the patients’ survival according to the combinations of the ATRX/IDH1 pair, the highest median OS (42.71 months) and PFS (42.2 months) were found in the patients with ATRX-/IDH1+, while the lowest median OS (20.7 months) and PFS (16.8 months) were observed in the patients with ATRX+/IDH1-. The analysis of the ATRX/p53 pair revealed that ATRX-/p53- expression evidenced the highest median OS and PFS (39.9 and 29.6 months, respectively), while the ATRX+/p53+ combination showed the lowest median OS and PFS (18.5 and 15.0 months, respectively). IDH1/p53 pair revealed that IDH1+/p53- group was correlated with the highest median OS and PFS (33.4 and 30.3 months, respectively), while IDH1-/p53+ group have the lowest median OS and PFS (18.0 and 14.7 months, respectively). Kaplan Meier survival analysis of two protein expression pairs also revealed the same results. Among them, the best survival combinations group were ATRX-/IDH1+, ATRX-/p53- and IDH1+/p53- (Fig. 3).
Fig. 3
Kaplan-Meier plots for GBM patient survival by combined two and three gene immunohistochemical status. (A) Among ATRX/IDH1 combination subgroups, the highest median OS of 42.7 months is found in the patients with ATRX-/IDH1+ status. (B) Among ATRX/p53 combination subgroups, the highest median OS of 39.9 months is found in the patients with ATRX-/p53- status. (C) Among IDH1/p53 combination subgroups, the highest median OS of 33.4 months is found in the patients with IDH+/p53- status. (D) The highest median OS of 47.9 months is found in patients with ATRX-/p53-/IDH+ status among three protein combination subgroups.

Immunohistochemical and survival analysis of GBMs with combinations of three protein expression
As shown in Table 4, combined three-protein immunohistochemical analysis revealed eight different molecular variants. About 1.8% (3/163) of the samples was consisted of aberrant protein expression of all three proteins, i.e., ATRX-/p53+/IDH1+, while 39.9% (65/163) were wildtype protein expression group, i.e., ATRX+/p53-/IDH1-.
The survival analysis of patients with these three proteins combination revealed the highest median OS and PFS of 47.9 and 47.9 months for ATRX-/P53-/IDH1+ combination and the lowest OS and PFS group was ATRX+/P53+/IDH1- combination (17.8 and 14.5 months, respectively) (Table 4).
In three biomarker combination group, the best survival was noted in the patients with ATRX-/p53-/IDH1+, which were comprised only 2.5% of GBMs (Fig. 3D) (P = 0.010).
DISCUSSION
It was previously observed in various studies that some relationship exists between aberrant expression of ATRX, p53, and IDH1 proteins in GBM patients and their OS. Though those studies, better OS outcomes in GBM patients with ATRX- and/or IDH1+ than patients with counterpart protein expression status (111415). The aim of our study was to establish a correlation between survival (OS and PFS) of GBM patients and the immunohistochemical expression of ATRX, IDH1, and p53, individually, as well as in different combinations. Immunohistochemically, we found ATRX loss in 15.3%, p53 overexpression in 48.4%, and IDH1 positivity in 10.4% of unselected GBM patients. Survival analysis based on immunohistochemical results showed a statistically significant better survival with ATRX- and/or IDH1+ when compared to patients with ATRX+ and/or IDH1- (Fig. 2). To date, some studies have demonstrated a correlation between TP53 gene mutations and decreased median survival, while others have not found such correlation. In our cohort, the patients with p53 overexpression showed a poorer median overall survival (19.3 months) when compared to GBM patients with p53- (26.2 months) (P = 0.019). However, the Kaplan Meier survival analysis, the only PFS was statistically better in GBM patients with p53- than patients with p53+ and the OS was tendency of better survival in the GBM patients with p53- than the patients with counterpart result (Fig. 2). Our results are in line with those obtained by Newcomb et al. (13); here, p53 mutations were found to be related to survival in an age specific manner being favorable if mutations are found in younger population (22-40 age group), whereas unfavorable after 40 years old (41-60 and 61-80 age groups). Our cases of GBMs with p53 overexpression also showed unfavorable OS in the patients with 45 years old and over that age (P = 0.014).
Immunohistochemically analyzing two and three protein combinations, we hypothesized whether certain molecular alterations were more likely to be associated with better OS and PFS. We found that the different protein alterations were associated with distinct survival rates. The survival differences reached statistical significance in all ATRX/p53, ATRX/IDH, and IDH1/p53 combination, and ATRX/IDH1/p53 combinations, with P < 0.05 in all categories (Fig. 3).
In conclusion, we have shown aberrant expression of ATRX, p53, and IDH1 proteins in our cohort of GBMs. Immunohistochemical analysis of ATRX, p53, and IDH1 individually, and in different combinations, revealed that aberrant expression of ATRX and IDH1 proteins and lack of p53 expression, together with combinations of ATRX-/IDH1+, ATRX-/p53-, IDH1+/p53-, and ATRX-/p53-/IDH1+ groups, were associated with a distinct and statistically significant increased survival rates regarding both OS and PFS. Therefore, these protein expression signatures individually, as well as the combined protein expression signatures, can stratify GBMs into prognostically relevant subgroups and may be used as prognostic markers in addition to diagnostic markers.
 XML Download
XML Download