

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Forecasting cause-specific mortality can help estimate the future burden of diseases and can be used as fundamental data for developing public health policies. The number of deaths worldwide has been increasing; it increased 13.5% from 46.5 million in 1990 to 52.8 million in 2010, and the disease burden is expected to increase (1). To reduce the disease burden, estimations of the future cause-specific mortality are needed to shape public policy and plan for expenditures. Moreover, mortality projections are needed to address the increase in chronic diseases from population aging in Korea. Although the trend analysis of the leading causes of death has been conducted in the observed period 1983-2012 (2), long-term future predictions of the leading causes of death up to 2032 have not been conducted in Korea.
The Norwegian cancer registry developed nordpred software, which was an R-based program that relied on a modified APC (age-period-cohort) model (34). The nordpred was originally designed to predict cancer incidence (U.K. [56], Canada [7], Switzerland [8] and U.S.A. [9]) and mortality (U.K. [10]). Instead of evaluating the cancer incidence and mortality, we adopted the general cause-specific mortality to the nordpred APC model.
Our objectives were as follows. First, the cause-specific mortality in future periods (2013-2017 to 2028-2032) was estimated by reflecting the mortality trends in the observed periods 1983-1987 to 2008-2012. Second, the overall change in the death rates was analyzed with the following three components: the change in the risk, age structure and population size.
MATERIALS AND METHODS
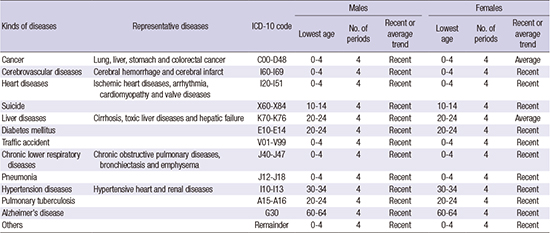
The death and population data were obtained from Statistics Korea. The death data consisted of 12 major causes of death (cancer, cerebrovascular diseases, heart diseases, suicide, liver diseases, diabetes mellitus, traffic accident, chronic lower respiratory diseases, pneumonia, hypertension diseases, pulmonary tuberculosis and Alzheimer's disease) from 1983 to 2012 by sex and age group in Korea (11). The ICD-10 codes (International Classification of Diseases version 10 by World Health Organization) of the 12 causes of death were shown in Appendix 1.
From the WHO research, completeness and quality of the death registration data of each countries were evaluated at the end of 2003. They grouped death registration data into high quality (23 countries), medium quality (55 countries) and low quality (28 countries) according to the criteria using the completeness and the ill-defined codes (completeness was defined as the proportion of all deaths covered by the vital registration system). Korea was included as medium quality group and has 89% completeness and 14% deaths coded to ill-defined codes (12).
The population data consisted of the observed (1983-2010) and estimated populations (2011-2032) by sex in Korea. The future populations are estimated using the cohort component method from the population census provided by the Statistics Korea (13). The death data were aggregated into 6 five-year periods (1983-1987 to 2008-2012) by sex and cause of deaths. The population data were aggregated into 10 five-year periods (1983-1987 to 2028-2032) by sex. The death data were aggregated into 17 five-year age groups (0-4 to 80+) by sex and cause of death. The population data were aggregated into the same age groups by sex.
To forecast future mortality, we evaluated the general mortality data, instead of cancer mortality data, in nordpred (modified APC model). The model was written as: Rap
= (Aa
+ D ∙ p + S ∙ Pp
+ Cc
)5. Rap
was the mortality rate in the age group ‘a’ and calendar period ‘p’. D was the common drift parameter. Aa
was the age component of the age group ‘a’. Pp
was the non-linear period component of the period ‘p’. Cc
was the non-linear cohort component of the cohort ‘c’. As Moller et al. (34) recommended, the power 5 function, instead of the logarithm function, was used as a link function to level off the exponential growth. If the trend had significant curvature (S) in the observed periods, the most recent 10 years instead of all observation periods were used to predict the future mortality. The drift parameters were empirically reduced by 0%, 25%, 50%, and 75% in the first, second, third, and fourth future periods, respectively. The lowest age groups in the model were determined by considering the number of deaths in each cell (shown as Appendix 1). Below the lowest age groups, the future mortality was estimated by using the average trend of the most recent 10 years. Age-standardized rates were calculated using the Segi world standard population with some modification of summing up the 80-84 and 85+ groups into the 80+ group (1415). The prediction base (number of periods) was determined when fitting the model by considering the goodness of fit.
The total change in the number of deaths consisted of the following three components: the change in the risk (rate), the change in the age structure, and the change in the population size. Nras
was the number of deaths given a cancer risk ‘r’, an age structure ‘a’, and a population size ‘s’. Nfff
was the number of deaths given the future rate, the future age structure, and the future population size. Nooo
was the number of deaths given the observed rate, the observed age structure, and the observed population size. Noff
was the number of deaths given the observed rate, the future age structure, and the future population size. Noof
was the number of deaths given the observed rate, the observed age structure, and the future population size.
The four changes were divided by Nooo
and were expressed as percentages (%). The methods were referenced in the study by Moller et al (3).
RESULTS
Table 1 summarized the observed (2008-2012) and predicted (2028-2032) numbers of deaths by cause of death, and the total change in the number of deaths was resolved into the change in the risk, age structure and population size from 2008-2012 to 2028-2032.
Table 1
The total change in the number of deaths due to changes in the risk, age structure and population size from 2008-2012 to 2028-2032
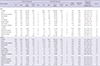
For males, the number of deaths is expected to increase by 52.7% from 2008-2012 to 2028-2032 (707,538 to 1,080,552 deaths). The APC (annual percent change) of all deaths will be 2.1% over the 20 years from 2008-2012 to 2028-2032. The overall change is due to the change in the risk (-66.7%), age structure (119.4%) and population size (4.4%). Although the risk is predicted to decline from 2008-2012 to 2028-2032, the overall number of deaths will increase because of the age structures, which make the largest contribution to the changes in the deaths.
For females, 41.9% of all deaths are expected to increase from 2008-2012 to 2028-2032 (565,347 to 802,243 deaths). The APC of all deaths will be 1.8% during the 20 years from 2008-2012 to 2028-2032. The overall change is due to the change in the risk (-73.3%), age structure (115.2%) and population size (6.4%).
For both sexes, the trends in the mortality by the cause of death were similar to each other as follows: increasing pattern from 2008-2012 to 2028-2032 (cancer, suicide, heart diseases, pneumonia, Alzheimer’s disease) and decreasing pattern (cerebrovascular diseases, liver diseases, diabetes mellitus, traffic accident, chronic lower respiratory diseases and pulmonary tuberculosis). Hypertension diseases is expected to increase in males, while it is expected to decrease in females. For both sexes, cancer ranked first among the 12 causes of death in 2008-2012, and this trend is expected to continue to 2028-2032.
Fig. 1 showed the projections of the crude rates and the age-standardized rates by major cause of death in the future period 2013-2032 based on the observed period 1983-2012. For all deaths, the age-standardized rates in the world standard population are expected to decrease from 2008-2012 to 2028-2032 (males: 447.6 to 307.0 [-31.4%], females: 230.9 to 156.4 [-32.3%] per 100,000 person-years). However, the crude rates are expected to increase from 2008-2012 to 2028-2032 (males: 570.7 to 834.7 [46.3%], females: 458.3 to 611.2 [33.4%] per 100,000 person-years).
Fig. 1
The projection of the crude and age-standardized rates by the major causes of death in the future period 2013-2032 based on the observed period 1983-2012.
MC, Male crude rates; FC, Female crude rates; MA, Male age-standardized rates; FA, Female age-standardized rates (per 100,000 person-years).
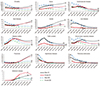
Fig. 2 showed the projections of the age-specific rates for the period 1983-2012 for all deaths on the basis of the observed period 2013-2032. As the age group was older, the age-specific rates sharply increased, especially in the over 80 years of age group.

Fig. 3 demonstrated that trends of the crude rates for the 12 major causes of death from 1983-1987 to 2028-2032. The major causes of death in 2028-2032 will be cancer, cerebrovascular diseases, heart diseases, suicide, pneumonia and diabetes mellitus.
Fig. 3
The trends of the crude rates according to 13 major causes of death from 1983-1987 to 2028-2032 in both sexes.
CA, Cancer; CVD, Cerebrovascular diseases; HD, Heart diseases; SUI, Suicide; LD, Liver diseases; DM, Diabetes mellitus; TA, Traffic accident; CLRD, Chronic lower respiratory diseases; PNA, Pneumonia; HTN, Hypertension diseases; TB, pulmonary Tuberculosis; ALZ, Alzheimer's disease.

DISCUSSION
Our main results were as follows. Although the age-standardized rates are expected to decrease from 2008-2012 to 2028-2032 in both sexes, the total number of deaths is expected to increase in both sexes (males: 52.7%, females: 41.9%). For both sexes, deaths from cancer, suicide, heart diseases, pneumonia and Alzheimer’s disease are predicted to increase from 2008-2012 to 2028-2032. On the other hand, the number of deaths from cerebrovascular diseases, liver diseases, diabetes mellitus, traffic accident, chronic lower respiratory diseases and pulmonary tuberculosis are predicted to decline. Additionally, cancer is expected to be the highest cause of death in both the 2008-2012 and 2028-2032 periods. Furthermore, the largest contribution to the overall change in the number of deaths is the change in the population, especially the change in the age structures.
In Korea, the proportion of aged people is expected to increase in 2028-2032 compared with the past periods, 1983-1987 and 2008-2012. The aged-child ratios (percentages of people over 65 years old over those younger than 14 years old) will increase in both sexes (males: 10.3% in 1983-1987, 53.5% in 2008-2013 and 168.1% in 2028-2032; females: 18.3% in 1983-1987, 84.2% in 2008-2013 and 219.3% in 2028-2032). Comparing between Korea and worldwide, the aged-child ratios of the aging population in Korea are expected to be higher than the world standard population (22.6%) in 2008-2013 and 2028-2032. Although the age-standardized rates are projected to decrease, the total number of deaths is projected to increase because of population aging in Korea.
Worldwide in 2030, ischemic heart diseases (13.4% of the total deaths), cerebrovascular diseases (10.6%), HIV/AIDS (8.9%), chronic obstructive pulmonary diseases (COPD) (7.8%), lower respiratory infection (3.5%), lung cancer (3.1%) and diabetes mellitus (3.0%) are expected to be the leading causes of death (16). In the comparison between worldwide and Korea, cancer, cardiovascular diseases (including heart diseases and cerebrovascular diseases), respiratory diseases and diabetes mellitus will be the most common leading causes of death in 2030.
Worldwide, ischemic heart disease and cerebrovascular disease were predicted to rank first and second, respectively, in 2002 and in 2030. The rankings for the following causes of death are estimated to increase from 2002 to 2030: HIV/AIDS, COPD, lung cancer and diabetes mellitus. However, the rankings for the following causes of death are estimated to decrease: lower respiratory infection, perinatal condition, diarrheal disease and tuberculosis (16).
HIV/AIDS is projected to rank higher among the causes of death worldwide than Korea because Africa has had the highest rate of deaths from HIV/AIDS (Africa: 1,100,000 deaths and world: 1,500,000 deaths in 2013 from the WHO website). However, suicide is expected to rank higher in Korea than worldwide due to the socioeconomic circumstances in Korea.
We evaluated the reasons for the increasing trends of several diseases (cancer, cardiovascular diseases, suicide, pneumonia and Alzheimer’s disease) and decreasing trends of other diseases (liver diseases and pulmonary tuberculosis). The increasing numbers for various causes of death were significantly associated with the elderly and with the population aging in Korea.
Cancer is estimated to be the leading cause of death among both men and women for the periods from 2008-2012 to 2028-2032 in Korea. As the average life expectancy increases, cancer is more likely to occur because cancer mortality is higher in the older age groups than in the younger age groups (17). Cancer mortality might be influenced by the high prevalence of smoking among adult males in Korea (1819). Smoking was responsible for 20.9% of cancer incident cases and for 32.9% of cancer deaths among adult males (20). Particularly, 71% of lung cancer deaths were attributable to smoking (20). Despite the prevalence of Helicobacter pylori has been decreased, which is a well-demonstrated risk factor for gastric cancer and was responsible for 80.3% of non-cardia gastric cancers in males and 78.7% in females (21). Westernized diets (red meat and processed meat), decreased physical activity, and increased prevalence of obesity were the risk factors for colorectal cancer in Korea (22).
The number of deaths from cardiovascular diseases (ICD-10: I00-I99) is estimated to increase 13.3% in males from 2008-2012 to 2028-2032 in Korea. The increasing trend is likely because of the increased prevalence of risk factors, such as smoking, physical inactivity, obesity and high-fat diets (2324). The prevalence of obesity in adult males has been increasing (from 25.4% in 1998 to 36.7% in 2007) in Korea (25). Additionally, the dietary habits and lifestyles have transitioned to the Western style (high fat content from red meat, high sugar and salt contents from processed foods) in Korea.
From the WHO website, the age-standardized suicide rate of both sexes in Korea (28.9 per 100,000 person-years) was the second highest rate among the 171 countries in 2012. We deduced that the high suicide rates were due to socioeconomic polarization and inequalities, social isolation and maladaptation to modern society in the setting of the rapid economic development in Korea. The high suicide rates in the elderly have been a serious problem in Korea (26).
The economically productive population (15-64 years) has increased from 1983-1987 to 2008-2012 [from 65.6% to 72.8%], and it will decrease sharply by 2028-2032 [63.1%]. The children and infant dependency ratio (0-14 years / 15-64 years × 100) has decreased from 1983-1987 to 2028-2032 [from 46.0% to 20.0%], but the old age dependency ratio (more than 65 years/15-64 years × 100) has increased from 1983-1987 to 2028-2032 [from 6.5% to 38.5%]. Overall, total dependency ratio (sum of two ratios) has decreased from 1983-1987 to 2008-2012 [from 52.5% to 37.4%], which is expected to increase by 2028-2032 [58.5%]. As population aging has progressed, the economically productive population is predicted to decrease and the dependency ratio is expected to increase. Therefore, supporting expenses of the economically productive population and their social pressure are expected to increase, which will be the risk factors for suicide in Korea.
The number of deaths from pneumonia will sharply increase from 2008-2012 to 2028-2032 (males: 319.9%, females: 274.1%). As population aging has been ongoing in Korea, the number of deaths from pneumonia will increase because the incidence of pneumonia is higher in elderly people (27) and because the elderly are particularly vulnerable to the functional decline of organ systems, such as the respiratory, immune and digestive systems, as well as the comorbidity with age-associated diseases (28).
The number of deaths from liver diseases is predicted to decrease from 2008-2012 to 2028-2032 (males: -48.1%, females: -33.1%). Because hepatitis B virus (HBV) was a major risk factor for liver diseases such as hepatitis and cirrhosis, (29) decreasing future projections of deaths from liver diseases may be due to the decreasing trend of the seropositive prevalence for hepatitis B virus surface antigens (HBsAg) (4.61% in 1998 and 2.98% in 2010) as well as the use of antiviral therapy for HBV in Korea (30).
The number of deaths from Alzheimer’s disease will increase from 2008-2012 to 2028-2032 in Korea (males: 108.0%, females: 3.0%). The female population above 80 years has been approximately two times more than the male population from 1983-1987 to 2008-2012, and this trend will persist up to 2028-2032. Therefore, female deaths due to Alzheimer’s disease will be more than male deaths because Alzheimer’s disease is frequently diagnosed among the aged people (31). However, the number of deaths due to Alzheimer’s disease was relatively small compared to the number of deaths due to other diseases and mortality trends have drastically changed recently. The nordpred model using the power 5 function as a link function was very sensitive to the recent trends. We thought that the prediction results of Alzheimer’s disease had large RBs (relative biases), and they should be interpreted carefully. A validation study for predicting mortality is needed in the future.
In addition to the growing population of the aged people in Korea, cerebrovascular disease, hypertension, type 2 diabetes, and obesity are the risk factors of Alzheimer’s disease. Cerebrovascular diseases such as hemorrhagic or ischemic infarctions can directly affect the brain region involved in the memory function, which can cause an increase in the prevalence of Alzheimer’s disease. Hypertension can reduce the integrity of the blood-brain barrier (BBB). Therefore, protein extravasation in the brain cells can increase, which can cause damage to the brain cells (32).
The number of deaths from pulmonary tuberculosis is projected to decrease from 2008-2012 to 2028-2032 (males: -49.7%, females: -23.4%). This decreasing trend may be due to the development of an anti-tuberculosis drug and improvement of personal hygiene in Korea.
The projection of mortality rates using the nordpred model had some limitations. First, the predictions of the nordpred model were not performed well in some diseases. In a preliminary study, ASR in 2008-2012 (5 years) was predicted based on the period from 1983-1987 to 2003-2007 (25 years) by sex and kinds of diseases. RBs were calculated between the estimated (E) and observed (O) ASR as follows: RB=|E-O|/O×100. Predictions of total deaths had better performance than those of disease-specific deaths because over-estimation and under-estimation of each disease-specific death were compensated by summing each death. RBs of all deaths were 3.6% in males and 0.1% in females, which were lower than those of the specific disease by sex.
Predicting mortality for some diseases having small numbers and recently drastic changes had large RBs than other diseases having large numbers and small recent changes. For example, pneumonia and Alzheimer’s disease had large RBs in both sexes. Although the power 5 function as a link function was important for estimating the long-term projections, some diseases having small numbers were very sensitive to application of the model using the recent trends. Therefore, careful interpretation is required for pneumonia and Alzheimer’s disease. Second, prediction of mortality for the diseases except for cancer has not been performed yet. Although the nordpred model was developed for projecting cancer incidence and mortality, we thought that it is applicable to estimating mortality for other diseases because of use of common age, periods and cohort variables (APC model) in the epidemiology. Validation of the nordpred model should be performed in the future. Third, the nordpred model predicted incidence better than mortality. Mortality was generally sparse than incidence in the specific disease. Therefore, modeling mortality was challenging than modeling the incidence (33).
Despite the disadvantages, predictive performance of the nordpred model seemed to be good. A Canadian group compared several APC models to estimate the long-term cancer incidence and mortality projections (34). They evaluated differences between the projected and observed rates of each models to figure out which models more precisely predicted the rates. The nordpred model and the Bayesian model performed better than the other models including GAM (generalized additive model) and conventional APC model. Particularly, the nordpred model using the power 5 function as a link function generally performed better than the model using the logarithm function.
Moller et al. (4) empirically compared the validity of the short and long-term projections among the various nordpred models by calculating the absolute median value of the differences between observed and predicted cases. Generally, the nordpred model using the power 5 function more improved the predictions than the classical APC model by leveling off the overestimated trends of the APC model.
Our study was meaningful with respect to presenting the first picture of predicting the 20-year disease-specific mortality based on the 30-year data. Under the circumstances of increasing medical expenditures of diseases such as cancer, cerebrovascular diseases, heart diseases and diabetes mellitus, a study predicting mortality can provide a valuable clue to develop policies and to allocate resources.
 XML Download
XML Download