

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Niemann–Pick disease, type C (NP-C), is a rare autosomal recessive lysosomal storage disorder characterized by progressive neurological symptoms and various degrees of visceral involvement (12). NP-C is caused by mutations in the genes NPC1 or NPC2, with approximately 95% of patients showing mutations in NPC1. The protein encoded by the NPC1 gene is predominantly localized in late endosomes; thus, NPC1 gene mutations lead to late endosome trafficking defects. Esterification is essential for successful cholesterol secretion from cells, which requires transport of endocytosed cholesterol from late endosomes to the Golgi apparatus and endoplasmic reticulum. NPC1 gene mutations therefore lead to intracellular accumulation of unesterified cholesterol and several glycosphingolipids (345). Patients with NP-C show a few common characteristic symptoms and signs, including vertical supranuclear gaze palsy (VSGP), dystonia, ataxia, psychosis, and hepatosplenomegaly. However, clinical presentation and progression of NP-C varies greatly, and is mainly influenced by the age of neurological symptom onset (67). Here, we present the first reported Korean cases of adolescent- and adult-onset NP-C in two siblings.
CASE DESCRIPTION
Case 1
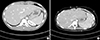
Our first patient was a 24-year-old man, who presented with psychosis, abnormal posturing, and gait disturbance. The conditions surrounding his birth and course of development had been unremarkable. At the age of 18, he started to develop delusions and abnormal posturing in both hands. At age 21, he was hospitalized at our Department of Psychiatry for psychotic symptoms, including visual and auditory hallucinations, aggressiveness, and impulsive behavior. Around this time, he also developed gait disturbance and cognitive impairment. Despite treatment, all symptoms gradually worsened. By age 24, he was completely dependent on caregivers and was confined to a wheelchair. An evaluation of family history revealed that his younger sister (Case 2) had similar symptoms. In November 2014 at the age of 24, neurological examination revealed generalized dystonia prominent in both upper limbs, severe ataxic gait, VSGP, severe dysarthria, and a mini mental status examination (MMSE) score of 18. Brain magnetic resonance imaging (MRI) showed no definitive signal change; however, mild atrophy of posterior brain regions was observed. A positron emission tomography (PET) scan using the radioligand 18F-FP-CIT showed mildly decreased uptake in both caudate and right anterior putamen compared to the posterior putamen (Fig. 1). An abdominal computed tomography (CT) scan revealed hepatosplenomegaly, which was undetected during a routine physical examination (Fig. 2). No abnormalities were found in routine laboratory tests or nerve conduction studies. Evaluations for Wilson's disease were performed, including the Kayser–Fleischer ring, 24-hour urine copper, serum copper and ceruloplasmin tests; however, all results were negative. Genetic tests for spinocerebellar ataxia 1,2,3,6,7,17, pantothenate kinase-associated neurodegeneration, dentatorubral-pallidoluysian atrophy, DYT-1, and Huntington's disease were all negative. NPC1 gene sequencing revealed a compound, heterozygous mutation, with aberrations in exon 9 (c.1552C>T [R518W]) and exon 18 (c.2780C>T [A927V]), which were previously identified as a genetic cause of NP-C (8). We additionally evaluated cultured skin fibroblasts for filipin staining, another diagnostic test for NP-C; patient results were positive (Fig. 3).
Case 2
Our second patient was a 23-year-old woman, who was the younger sister of patient 1. She visited our clinic in November 2014 for the first time. The patient had no other siblings, and there was no further notable family history. Her symptoms began with clumsiness in the right hand at age 19. Initial symptoms were followed by psychosis, cognitive impairment, and gait disturbance, which gradually worsened over the next 4 years. On examination, she had similar symptoms to her older brother (including VSGP). However, symptoms appeared to be milder; she was able to walk unassisted and independently perform daily living activities. Cognitive impairment (with an MMSE score of 23) was also less severe than that in her older brother. An abdominal CT scan revealed hepatosplenomegaly (Fig. 2), and a brain MRI showed diffuse brain atrophy. Sequencing analysis revealed a genetic mutation identical to that of her brother, and filipin staining results were positive (Fig. 3). Based on the evaluations, this patient was also diagnosed with NP-C. We have initiated miglustat therapy in our patients, with careful observation for common side effects, such as diarrhea and other gastrointestinal symptoms.
DISCUSSION
There are approximately 500 NP-C cases diagnosed worldwide; however, the actual number of patients with NP-C is believed to be much higher (9). This is the first adolescent- or adult-onset NP-C case report in Korea. Although the estimated incidence of NP-C is 1 in 120,000–150,000 live births, there has been only one previous case of perinatal-onset NP-C reported in Korea (diagnosed by genetic analysis), presenting with neonatal cholestasis, hepatosplenomegaly, and no neurological symptoms (610). A highly probable reason that NP-C has been underdiagnosed in Korea is that there is extreme heterogeneity in disease-related symptoms and signs (1112).
Symptoms are greatly influenced by age of onset; therefore, NP-C is grouped into the following categories, based on onset time: perinatal, early and late infantile, juvenile, and adolescent or adult (126). The most representative systemic NP-C sign is hepatosplenomegaly. However, patients with adolescent- or adult-onset disease forms, as our patients, are often asymptomatic; thus, abdominal imaging studies are useful diagnostic tools in all suspected cases (13).
Among the various symptoms, VSGP should be considered a highly important sign for NP-C diagnosis. VSGP is present in between 66 and 81% of NP-C cases (171415). Although patients with diseases other than NP-C may present with VSGP (16), the majority of these conditions are adult-onset neurodegenerative disorders, including progressive supranuclear palsy, corticobasal syndrome, Huntington's disease, and Creutzfeldt–Jacob disease. VSGP is relatively very uncommon in all of these conditions, with the exception of progressive supranuclear palsy. Thus, the presence of VSGP in a young patient is a strong indicator of possible NP-C. Moreover, because genetic disorders showing both hepatosplenomegaly (the most representative systemic NP-C sign) and VSGP are rare (other than NP-C) detecting these two signs together narrows possible diagnoses significantly. Thus, detailed neurological and physical examinations that test for VSGP and hepatosplenomegaly are highly important to improve diagnostic accuracy.
There have been few neuroimaging studies in NP-C cases, and MRI findings are often normal early during the disease. However, as NP-C progresses, there is a strong correlation between common clinical signs and cortical atrophy, predominantly in the frontal lobes, brainstem, or cerebellum (13). In contrast, Case 1 had posterior brain atrophy. The significance of this differential atrophy pattern is unknown, meriting further clinicopathological studies.
There has been no systematic neuroimaging report assessing substantia nigra dopaminergic neuronal loss in patients with NP-C. Although Case 1 showed no obvious clinical features of parkinsonism, decreased dopaminergic uptake was detected using 18F-FP-CIT. The dysfunction pattern, however, appeared to be different from that in neurodegenerative parkinsonism and there has been no report of dopaminergic neuroimaging on NP-C. Further studies are therefore needed to determine whether dopaminergic dysfunction and its distinct pattern are another feature of NP-C.
Two important tools used in NP-C diagnosis are the genetic and filipin tests. The filipin test detects unesterified cholesterol in cultured skin fibroblasts stained with filipin, a fluorescent chemical compound. The hallmark storage pattern (an increased number of filipin-stained vesicles) can be identified in 80%–85% of cases (3).
NP-C became among a minority of treatable genetic diseases with the development of miglustat, a competitive inhibitor of glucosylceramide synthase (17). Patients who begin treatment early in the disease course show improved responses, highlighting the need for rapid diagnosis. When a patient with relevant familial background presents with idiosyncratic NP-C features, diagnosis is straightforward. However, in cases with atypical symptomology, a careful examination for VSGP is critical to enhance diagnostic accuracy in potential NP-C cases.


 XML Download
XML Download