

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Radical cystectomy and orthotopic neobladder reconstruction is the most complicated surgery in urology. Various complications occur in the early and late postoperative periods in a significant proportion of cases, even with experienced surgeons (123). Urinary tract infection (UTI) is one of the most common complications after radical cystectomy and orthotopic neobladder. Specifically, previous studies have shown that patients with orthotopic neobladder had higher incidence of UTI than patients who received an ileal conduit (45). Although the rate of symptomatic UTI is lower than that of bacteriuria in patients with orthotopic neobladder, patients with febrile UTI are at increased risk of urosepsis (678). Moreover, several studies have reported that febrile UTI can adversely affect renal function in patients with ileal neobladder reconstruction (910). Most UTIs occur within one year after surgery (11), possibly due to differences in mucosal host response against bacteria between the intestine and urothelium. Various risk factors for UTI have been suggested, but studies usually focus on clinical factors such as gender, diabetes or body mass index (71213). Data on the relationship between urodynamic parameters and febrile UTI is limited, particularly in patients who are adapting to different voiding conditions in the early postoperative period after neobladder reconstruction. In addition, although bacterial species associated with UTI in neobladders have been described, there has been no investigation of the relationship between implicated bacterial species in these patients and time after surgery.
In this study, we investigated the incidence of febrile UTI and associated pathogens with time after surgery and aimed to identify urodynamic parameters associated with increased risk of febrile UTI after ileal neobladder reconstruction.
MATERIALS AND METHODS
Patients and surgical procedure
A review of medical records identified 296 patients who underwent radical cystectomy and urinary diversion for bladder cancer from January 2001 to May 2015 at our institution. Of the 296 patients, a total of 236 patients who underwent radical cystectomy and ileal neobladder were included in this study. All operations were performed with the standard open surgical approach. A Studer pouch was used for orthotopic substitution (14) and ureteroileal anastomosis was performed using the Nesbit technique. All patients were treated with prophylactic antibiotics, which usually included 7 days of second generation cephalosporin and 5 days of metronidazole, intravenously. Preoperative bowel preparation with 4 liters of oral polyethylene glycol was routinely performed. Ureteral stents were removed on postoperative day 7; however nonstented ureteroileal anastomosis was performed from August 2014, thus ureteral stents were not placed at the time of surgery in 51 patients. Urethral catheters were maintained for 10-14 days after surgery. All patients were educated to adequately empty the neobladder and achieve a desired volume of 400-500 mL without incontinence.
Measurement and definitions
Clean catch urine samples were obtained according to standard sterile procedures for cultures and antimicrobial susceptibility testing. Febrile UTI was defined as a positive urine culture with at least 104 colony-forming units per milliliter of urine and an elevated body temperature (≥ 38°C). Sepsis was defined in accordance with the updated clinical criteria in The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3): increase in the Sequential Organ Failure Assessment (SOFA) score of 2 points or more (15). All patients with febrile UTI were admitted and treated by intravenous broad spectrum antibiotics. Susceptibility tests were used to guide antibiotic choice in patients who did not respond to the initial antibiotics treatment.
Videourodynamic study
From November 2013, we performed video urodynamic testing at 3-6 months after surgery as part of a comprehensive functional evaluation of ileal neobladder. Multichannel urodynamic system (MMS Solar, Medical Measurement System, Enschede, The Netherlands) was used for urodynamics and all methods, definition, and units conformed to the standards proposed by the International Continence Society. The urodynamic parameters included the maximal cystometric capacity, residual volume, maximal flow rate, compliance, and detrusor pressure at maximum flow rate. Incidence and characteristics of vesicoureteral reflux (VUR) were also evaluated.
Statistical analysis
Every episode of febrile UTI was identified during follow up. We also identified patients with positive blood cultures for same bacteria or sepsis. We investigated the associated pathogens in association with time after surgery. Quantitative variables were compared using Student’s-t test and qualitative variables were compared using χ2 and Fisher’s exact tests. The probability of febrile UTI was evaluated using Kaplan-Meier methods. Multivariate logistic regression analysis was conducted to identify risk factors associated with the development of febrile UTI after ileal neobladder reconstruction. The Statistical Package for Social Science for Windows, version 18.0 (SPSS, Chicago, IL, USA) was used for all statistical analyses. A P value < 0.05 was considered significant, and all P values were two-sided.
RESULTS
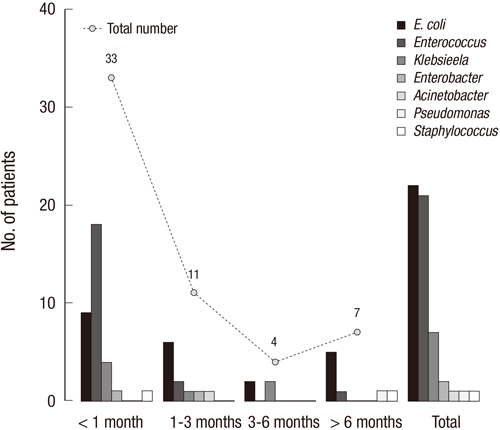
The characteristics of all 236 patients are summarized in Table 1. During the median follow up period of 25 months (IQR, 18-37), 55 episodes of febrile UTIs were identified in 46 patients (19.4%). Six episodes were associated with positive blood cultures with same pathogen. Sepsis occurred in 2 patients. Seven patients (2.9%) developed multiple episodes of febrile UTI. Of 55 episodes of febrile UTIs, 33 (61.1%) occurred within 1 month after surgery; eleven (20.3%) and 4 (7.4%) episodes developed at 1-3 months and 3-6 months after surgery, respectively. Overall, 88% of febrile UTIs occurred within 6 months after surgery. The probability of febrile UTI was 17.6% and 19.8% at 6 months and 24 months after surgery, respectively. Overall, Escherichia coli was the most common implicated pathogen (40.0%, 22/55). However, of the 33 episodes that occurred within the first month after surgery, Enterococcus spp. were the most frequently isolated organism (54.5%, 18/33) (Fig. 1).
Table 1
Characteristics of patients
![]()

Several parameters were compared between patients with and without febrile UTI (Table 1). Patients with febrile UTI had a significantly higher incidence of ureteral stricture (8.7% vs. 1.6%, P = 0.028). There were no between-group differences in age at surgery, gender, body mass index, presence of hypertension or diabetes. In a multivariate analysis, only ureteral stricture was an independent risk factor associated with the development of febrile UTI (OR 5.93, P = 0.023) (Table 2). Although ureteral stricture independently affected the development of febrile UTI, only 6 episodes (10.9%, 6/55) were associated with ureteral stricture overall, and 4 of these episodes occurred 6 months after surgery.
Table 2
Multivariate logistic regression analysis to identify risk factor associated with febrile UTI after neobladder reconstruction
![]()
To identify risk factors associated with febrile UTI in the initial postoperative period, we assessed videourodynamics within 6 months after surgery in 38 patients included in our study cohort (Table 3). Of the 38 patients, 10 had a febrile UTI within 6 months after surgery and none had ureteral stricture. On videourodynamic evaluation, maximal cystometric capacity, maximal flow rate, compliance, and detrusor pressure at maximum flow rate were not significantly different between patients with and without febrile UTI. Patients with febrile UTI had larger residual urine volume than those without (212.0 ± 193.7 vs. 90.5 ± 148.2, P = 0.048). VUR was identified in 25 renal units (32.9%) in 16 patients (42.1%). VUR was bilateral in 9 patients and grade III or higher in 10 renal units (13.1%). The rate of VUR presence in patients who had febrile UTI was not significantly different from those in patients without febrile UTI (50% vs. 39.3%, P = 0.556). Of 16 patients with VUR, patients with low compliance (< 20 mL/cm H2O) were more likely to experience febrile UTI than patients with normal compliance (57.1%, 4/7 vs. 11.1%, 1/9), but the difference was not statistically significant (P = 0.106).
Table 3
Videourodynamic parameters at 3-6 months after ileal neobladder reconstruction
![]()
DISCUSSION
In the present study, we examined 236 patients who underwent radical cystectomy and ileal neobladder. Although febrile UTI occurred in a significant proportion of patients who underwent radical cystectomy and neobladder reconstruction, most febrile UTIs developed in the early postoperative period, a finding consistent with previous studies (811). The observed decline in the incidence of UTI over time after surgery might make UTI seem less important at long term follow up. However, recurrent UTI increases the risk of developing urosepsis (7) and quality of life can be impaired in patients with symptomatic UTI (16). Moreover, febrile UTI has the potential to affect renal function outcomes regardless of type of urinary diversion (91017). Nishikawa et al (10) suggested that inflammation or bacteriuria associated with symptomatic UTI might influence renal function deterioration irrespective of urinary tract obstruction.
Ureteroiliac stricture can affect both febrile UTI and renal function deterioration. In this study, ureteral stricture was the only independent risk factor associated with febrile UTI. However, ureteral stricture accounted for only a small proportion of febrile UTIs and most episodes developed within 6 months after surgery irrespective of ureteral stricture. This finding suggests the possibility that febrile UTI might be associated with immature urodynamics of the neobladder in the early postoperative period.
In this study, we performed a subgroup analysis of patients who had videourodynamic examination. All tests were performed within 6 months after surgery to reflect the initial urodynamic features of the neobladder. Patients with a febrile UTI in the early postoperative period had larger post-void residual urine volume. This finding is in line with previous studies, which reported that complete emptying of the neobladder reduces bacterial colonization and larger post-void residual urine volume is significantly related to febrile UTI (918). These findings strongly indicate that active postoperative education for emptying the neobladder and regular follow up are both necessary.
The need for an anti-reflux mechanism has been the subject of controversy. A recent single center randomized study demonstrated that an anti-reflux system did not have a significant impact on either renal function change or the development of symptomatic UTIs (19). In our results, approximately 40% of patients had VUR at videourodynamic evaluation. While the incidence of febrile UTI was not higher in patients with VUR, greater than half of patients with VUR and low compliance experienced febrile UTI. Although the compliance profile is expected to improve with the decline in intravesical pressure at follow up, this finding suggests that low compliance may increase the risk of febrile UTI in patients with VUR. Follow up urodynamic examination could reveal the change of compliance and persistence of VUR with maturation of the neobladder.
Several studies have identified bacterial species involved in UTI after neobladder reconstruction (681118). Among the various uropathogenic species, Escherichia coli is the most common pathogen in most studies, in line with our results. However, Enterococcus spp. were the most common pathogen associated with febrile UTI within the first month after surgery in our study. The difference could be simply due to incomplete bowel preparation with residual microbial flora in the ileal segment of the neobladder. Although Large et al. (20) reported that omitting mechanical bowel preparation did not increase the risk of postoperative UTI in patients undergoing radical cystectomy and urinary diversion, greater than half of the patients in their study were treated with ileal conduit. Antibiotic prophylactic regimens may have also contributed to this result. Enterococcus spp. are not fully sensitive to second generation cephalosporin, which was used as a prophylactic antibiotic in our cohort and may have led to temporary predominance of Enterococcus spp. in the early postoperative period. However, we are not able to fully explain postoperative UTI with residual burden or species of bacteria in the bowel segment used for neobladder reconstruction. Although the colon is the primary site of microbial colonization (21), colonic neobladder is associated with lower rates of UTI than ileal neobladder (818). These findings suggest that postoperative UTI after neobladder surgery might be influenced by environmental conditions such as the inflammatory response or mucosal structure of the bowel segment rather than the bacterial population burden. The underlying mechanism for the greater incidence of bacteriuria in ileal neobladder compared to colonic neobladder is unknown. Wullt et al. (22) demonstrated that the mucosal response to colonization of uropathogens is more prominent in ileal neobladders than colonic neobladders. Histologic findings of neobladder ileal mucosae show structural modification (6), and prolonged contact with urine may change the mucosal structure or inflammatory response of neobladder mucosae. Changes in expression patterns of specific receptors for pathogen recognition or innate immune activation may have contributed to not only selection of certain uropathogens but also the observed decline in the incidence of UTI with time after surgery.
This study had several limitations. It was a retrospective study and follow up time was relatively short. Information on follow up urine cultures after surgery was incomplete and we did not investigate the incidence and significance of asymptomatic bacteriuria. Videourodyamic testing was not performed in all patients. In addition, serial follow up of urodynamic evaluation was not available. Serial urodynamic examinations might improve our understanding of the change of urodynamic parameters and their association with VUR and UTI at long term follow up. Further research using biospecimens such as neobladder mucosae or urine microbiotas is necessary and may reveal differential gene expression according to prolonged contact with urine and environmental changes in the neobladder.
In conclusion, although febrile UTI is a common complication after radical cystectomy and ileal neobladder reconstruction, most episodes of febrile UTI occurred within 6 months after surgery. Febrile UTI occurred more frequently in patients with large residual urine volume. Active postoperative education for adequate neobladder emptying is important to prevent febrile UTI during the early postoperative period. While Escherichia coli is the most common cause of febrile UTI, Enterococcus spp. were the most common microorganism isolated during the first month after surgery.
 XML Download
XML Download