

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Heterotopic pregnancy (HP) is defined as the simultaneous occurrence of both intrauterine and ectopic pregnancy (1). Previously, the prevalence of HP was only 1 in 30,000 normal gestations (1). However, the frequency of HP has increased to approximately 152 cases in 100,000. This change may be related to the advent and growing use of technologies such as ovulation induction and assisted reproductive technology (ART) (23). Infertile patients who undergo ART frequently have tubal factor infertility; tubal pathology happens to be one of main causes of ectopic pregnancy (45). Therefore, since HP is no longer as rare as it once was, it is important to consider, especially when women conceive via ART treatment.
The early diagnosis and treatment of HP is critical to avoid its life-threatening consequences including hypovolemic shock, maternal mortality and fetal loss. However, in its early stages, HP can be difficult to diagnose because there may also be an intrauterine pregnancy (56). Therefore, if a patient has risk factors for HP, it is very important to suspect the diagnosis.
HP is ideally treated by (surgically and medically) removing the ectopic pregnancy, while maintaining the intrauterine pregnancy. Ectopic pregnancies can be removed surgically via laparotomy or laparoscopy. The success rate of parturition after these conservative treatments is between 58% and 70% (6). However, this successful management is confined to several case reports. The surgical area involved in an interstitial pregnancy is different from that in a tubal pregnancy. The intrauterine pregnancy outcome may differ between interstitial and tubal pregnancies. Therefore, this is concern for potential fetal loss after such surgical treatments (7).
The objective of this study was to investigate and compare the HP outcomes after treatment for interstitial and tubal ectopic pregnancies. It also addresses the risk factors that are associated with HP following in vitro fertilization (IVF)-embryo transfer (ET).
MATERIALS AND METHODS
We evaluated 48 patients who were diagnosed with HP between May 1998 and December 2012 from a single center. The patients underwent infertility treatments including Clomid with timed coitus (n = 1, 2.1%), superovulation with intrauterine insemination (n = 7, 14.6%), fresh non-donor IVF-ET (n = 33, 68.8%), and frozen-thawed cycles (n = 7, 14.6%). An additional 84 infertility patients were randomly selected as controls from the IVF registry database from the same period. The control group patients conceived intrauterine singleton or twin pregnancies through fresh non-donor IVF-ET (n = 72, 85.7%) and frozen-thawed cycles (n = 12, 14.3%).
Patients from the IVF registry could not be contacted. Clinical characteristics including age, gestational age at diagnosis, method of pregnancy, site of ectopic pregnancy, treatment of ectopic pregnancy, and clinical manifestations of heterotopic pregnancy were analyzed. The following basal characteristics were analyzed and compared between the control and heterotopic pregnancy groups: age, body mass index, previous ectopic pregnancy history, previous tubal surgery, previous pelvic inflammatory disease (PID) history, duration of infertility, infertility diagnosis, IVF parameters (stimulation duration (days), total dose of gonadotropin (IU), serum estradiol (E2) level on hCG day (pg/mL), number of retrieved oocytes, number of transferred embryos, serial serum ß-hCG (mIU/mL), incidence of ovarian hyperstimulation syndrome (OHSS), and pregnancy outcome (first trimester fetal loss, live birth, mode of delivery, follow up loss). The serum ß-hCG was checked serially on days 12, 14, and 21 of the ovum retrieval. A first trimester fetal loss was defined as an abortion that occurred before the 12th week of gestation. This included fetal losses that occurred after surgery for HP. If at least one live baby was born, the pregnancy outcome was regarded as a live-birth delivery. The pregnancy outcomes were analyzed according to singleton or twin pregnancies. Preterm delivery was defined as delivery occurring before the 37th gestational week. Term deliveries occurred after 37 gestational weeks. These definitions were also applied to twin pregnancies. The mode of delivery was classified as cesarean section or vaginal.
The statistical analyses were performed using IBM SPSS (ver. 21.0). Continuous variables were presented as means ± standard deviations (SD) and categorical variables were expressed as raw numbers or percentages. We compared the risk factors of heterotopic and normal intrauterine pregnancies in the IVF-ET patients. First, Kolmogorov-Smirnov test was used if normality was satisfied. If normality was not satisfied, Mann-Whitney U test used to compare effects between groups. With normality satisfaction, two sample t-tests were used to compare the mean values between the HP group and the control group. In contrast, χ2 test, Fisher's exact test, and linear by linear association method were used to compare percentages. We also used repeated-measures two factor analysis according to singleton and twin pregnancies to evaluate the serial serum ß-hCG level. Multiple logistic regression analysis was used to calculate the odds ratio (OR) and 95% confidence interval (CI) of the risk factors for predicting HP. P values < 0.05 were considered statistically significant.
RESULTS
Clinical characteristics of heterotopic pregnancy (HP)
The clinical characteristics of the 48 patients with HP are shown in Table 1. All 48 patients conceived using infertility treatments with ovulation induction, or with IVF-ET. The average diagonal gestational age was 7.5 ± 1.2 weeks (range 5.4-10.3). Forty-one patients (85.4%) with HP were diagnosed based on clinical symptoms including severe abdominal pain or vaginal bleeding. Thirty-three patients (68.8%) had hemoperitoneum and nine patients (18.8%) developed hypovolemic shock requiring a blood transfusion. Only seven patients (14.6%) were asymptomatic. Six patients (12.5%) were diagnosed within three weeks of undergoing treatment for missed abortions. None of these six patients had a history of ectopic pregnancy, but they had undergone fresh non-donor IVF-ET.
Table 1
Clinical characteristics of patients with heterotopic pregnancy

![]()
Ectopic pregnancies most frequently occurred in the fallopian tubes (70.8%), then in the interstitial (18.8%), and cervix (4.2%). Three patients (6.3%) had surgery at another hospital, so the site of ectopic pregnancy was unknown. Heterotopic pregnancies were treated with methotrexate intramuscular injections (n = 3, 6.3%; 2 cases of post-curettage status and 1 case of cervical pregnancy) or surgical procedures (such as laparoscopic salpingectomy (n = 33, 68.8%) or laparotomy (n = 10, 20.8%). Dilatation and curettage (n = 1, 2.1%) was performed for a single case of cervical pregnancy (Table 1).
Comparing the IVF-ET characteristics of the heterotopic and control groups and risk factors for predicting HP in IVF-ET cycles
This study compared the baseline clinical characteristics of the HP group (n = 40, IVF-ET only) and the control group (n = 84) (Table 2). There were no significant differences in patient age or BMI between the groups. A higher proportion of patients in the HP group underwent IVF-ET treatment because of tubal factor infertility than did in the control group (35% vs. 13.1%, P = 0.001). There were also significant differences in the rates of previous ectopic pregnancy (22.5% vs. 3.6%, P = 0.002) and previous tubal surgery (32.5% vs. 14.3%, P = 0.018) between the two groups. There was a significantly higher rate of prior abortion in the HP group than there was in the control group (P < 0.001). The incidence of primary infertility was higher in the control group than in the HP group (P = 0.011) (Table 2). When we analyzed between fresh nondonor and frozen thawed cycles, there was a difference in previous tubal surgery (fresh cycles, control 13.9% vs. heterotopic 24.2%, P = 0.191 ; frozen cycles, control 16.7% vs. heterotopic 71.4%, P = 0.045).
Table 2
Baseline characteristics of In vitro Fertilization– Embryo transfer (IVF-ET) patients in control and heterotopic pregnancies

Values are expressed as mean ± standard deviation or n (%).
PID, pelvic inflammatory disease; FSH, follicle-stimulating hormone.
*t-test; †χ2 test; ‡Linear by linear association; §Fisher’s exact test.
![]()
The IVF parameters are compared in Table 3. The duration of stimulation was short in the HP group (P = 0.017). Significantly more oocytes were received and more embryos were transferred in the HP group compared to those in the control group (15.9 ± 9.3 vs. 7.5 ± 3.3, P < 0.001; 3.5 ± 0.9 vs. 3.1 ± 0.9, P = 0.035). There was a significantly higher incidence of OHSS in the HP group than there was in the control group (21.1% vs. 4.8%, P = 0.009). We evaluated the serial serum β-hCG using repeated-measures ANOVA according to the number of intrauterine fetuses. There was no significant difference in the ß-hCG levels between the two groups according to singleton (P = 0.978) and twin pregnancies (P = 0.715) (Table 3).
Table 3
Comparison of In vitro Fertilization– Embryo transfer (IVF-ET) characteristics of control and heterotopic pregnancy patients

Values are expressed as mean ± standard deviation or No. (%).
ICSI, intracytoplasmic sperm insemination; OPU, ovum pick up; OHSS, ovarian hyper-stimulation syndrome.
*3 missing data; †repeated-measures two factor analysis for serial serum β-hCG levels, according to singleton (P = 0.978) and twin (P = 0.715); ‡χ2 test; §t-test; ‖Fisher’s exact test.
![]()
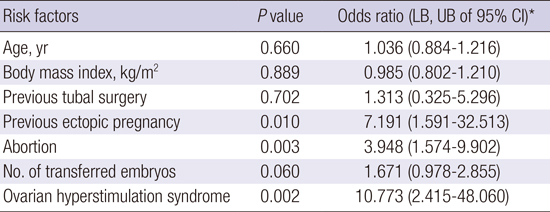
The risk factors of HP included a history of previous ectopic pregnancy (odds ratio (OR) 7.191, 95% CI 1.591-32.513, P = 0.010), number of abortions (OR 3.948, 95% CI 1.574-9.902, P = 0.003), and OHSS (OR 10.773, 95% CI 2.415-48.060, P = 0.002) (Table 4).
Table 4
The risk factors of heterotopic pregnancy in IVF-ET patients
![]()
Outcomes after the surgical treatment of HP
Eight patients were excluded (6 post-curettage status, 1 methotrexate, and 1 induced abortion), leaving 40 patients to be evaluated for their pregnancy outcomes after HP (Table 5). After surgery for ectopic pregnancy, there was no significant difference in the rates of first trimester intrauterine fetal loss (15.0% vs. 13.1%, P = 0.773) or live birth (80.0% vs. 84.1%, P = 0.605) between the HP group and the control group. In the HP group, 83.3% of the subjects delivered near term, while 16.7% delivered preterm. There was no discernable difference in the delivery mode between the two groups (Table 5).
Table 5
Pregnancy outcomes in control and all of heterotopic pregnancies
![]()
Comparison between HP at interstitial (HP-interstitial) and HP at tube (HP-tube)
There were 9 cases of HP-interstitial and 34 cases of HP-tube. There was a significantly high rate of previous ectopic pregnancies in the HP-interstitial group compared to that in the HP-tube group (55.6% vs. 11.8%, P = 0.011) (Fig. 1). There were five cases (55.6%) of bilateral tubal obstruction as demonstrated on hysterosalpingography (HSG). The tubal obstruction more commonly occurred on the left side (data not shown). All of the HP-interstitial were conceived using IVF (6 fresh non-donor IVF-ET cycles, 3 frozen-thawed cycles). There were three cases of first trimester fetal loss (37.5%, 3/8, excluded 1 post curettage status) in the HP-interstitial group and two cases (6.9%, 2/29, excluded 5 post- curettage status) in the HP-tube group. This difference was relatively high, but did not reach statistical significance (P = 0.057).
 | Fig. 1Clinical characteristics and pregnancy outcomes according to the site of heterotopic pregnancy.
The data exclude 6 post-curettage status (1 interstitial pregnancy, 5 tubal pregnancy).
IVF-ET, in vitro fertilization – embryo transfer.
Fisher’s exact test; *
P < 0.05, statistically significant.
|
There were live births in 4 of the HP-interstitial cases (57.1%, 4/7, excluded 1 follow up loss) and 19 in the HP-tube group (90.5%, 19/21, excluded 8 follow up loss) (P = 0.082). Seventy-five percent (3/4) of patients with HP-interstitial had preterm deliveries, while 94.7% (18/19) of those with HP-tube delivered at term.
Among the singleton intrauterine pregnancies, two were delivered preterm in the HP-interstitial group and one in the HP-tube group (28.6%, 2/7, 36.2 vs. 4.8%, 1/21, P = 0.051). In the cases of twin intrauterine pregnancy, there was one preterm delivery in the HP-interstitial group and no preterm delivery in the HP-tube group (14.3%, 1/7 vs. 0%, 0/21). All of the HP-interstitial were delivered through cesarean section (100% vs. 63.2%, P = 0.273) (Fig. 1).
DISCUSSION
Ovulation induction and ART are associated with an increased risk of HP (7). Despite the early transvaginal ultrasonography performed in patients with IVF-ET, only 16% of asymptomatic patients were diagnosed with HP. Early diagnosis is quite difficult (8). Clinical manifestations of HP include abdominal pain, vaginal bleeding and spotting. However, these symptoms are also sometimes observed in intrauterine pregnancies. Furthermore, the serum β-hCG levels are not helpful in the diagnosis of HP. Therefore, HP may be discovered late, increasing the risk of considerable intraperitoneal bleeding and life-threatening hypovolemia (5612). Shah et al. (8) found that HP is more likely to require blood transfusions secondary to hypovolemic shock (13.8% vs. 33.4%) than are ectopic pregnancies. Ultimately, having a high index of suspicion for HP, and knowing its risk factors are the most important ways to attempt an early diagnosis.
Six patients (12%) in this study were diagnosed with HP three weeks after already undergoing treatment for missed abortions. These patients ranged between 26 and 35 years old, and had conceived through fresh non-donor IVF treatment. There was higher number of transferred embryos (up to 4) and no history of ectopic pregnancy in these cycles. There may be an associated risk of HP in young people who have multiple transferred embryos. Even in the case of a small suspicion of HP, clinicians should check serial serum β-hCG levels after abortion treatment. In addition, minimizing the number of the transferred embryos or single embryo transfer could be best way to avoid the HP in young patients.
A history of PID and tubal damage have previously been reported as the major risk factors for HP (9). The most meaningful risk factors that we identified for HP included a history of ectopic pregnancy, abortion history, and OHSS. Generally, the history of an ectopic pregnancy increases the risk of a subsequent ectopic pregnancy. The characteristics of HP were similar to those of ectopic pregnancy (5).These knowledge may be applicable even in the IVF–ET setting of transferred embryos into the uterus. Several researchers have previously suggested that HP may be more likely after ART because multiple embryos are transferred, along with a large volume of culture media (1011). In contrast, other studies have shown that the number of transferred embryos does not affect the incidence of HP (311). Similarly, we did not find that the number of transferred embryos was significantly correlated with the risk of HP.
The primary goals of treating a HP are removing the ectopic mass, while sustaining the intrauterine pregnancy. Clayton et al. (5) reported that the relative risks of spontaneous abortion and induced abortion in intrauterine pregnancy after the treatment of HP are 2.05 and 10.3, respectively. Buckett et al. (13) reported that the rates of biochemical pregnancy and miscarriage are 17.4% and 15.2%, respectively. Barlow et al. (14) observed similar rates of early pregnancy loss. Soriano et al. (15) reported that approximately 33% of patients experienced first- or second-trimester miscarriage, leading the group to believe that surgical intervention may affect pregnancy loss. In our study, there was no significant difference in the rate of the first trimester intrauterine fetal loss related to the surgical procedures between the HP group and the control.
However, when the first trimester fetal loss was analyzed according to the site of the HP, there was marginal significance (37.5% vs. 6.9%, P = 0.057) between the HP-interstitial and HP-tube. The treatment for HP-interstitial may affect the rate of fetal loss. However, in order to detect such an effect, more cases are needed. The rate of first trimester fetal loss was lower in HP-tube (6.9% vs. 13.1%) than it was in the controls. In early pregnancy, therefore, laparoscopic salpingectomy may be a safe procedure with regard to the intrauterine pregnancy. To the best of our knowledge, this is the first study that separately evaluates the HP outcomes separately between HP-interstitial and HP-tube [PUBMED, term "heterotopic pregnancy", July 23, 2015]. Previous reports were confined to case reports or to the use of the large population-based ART registry. Other groups could not do so because of a lack of data, or a small sample size.
Clayton et al. (5) report little difference between the live birth delivery outcomes in women with intrauterine pregnancies and those with HP. There is also a similar live birth rate in the HP and control groups. In this study, the live birth rate in the HP group was 80%, which was not different from that of the controls, and is comparable to the results of other reports (515). The live birth rate was higher in HP-tube than in HP-interstitial, although the result was not statistically significant (90.5% vs. 57.1%). Preterm delivery of HP-interstitial was higher than that of HP-tube in a singleton intrauterine pregnancies (28.6% vs. 4.8%) with borderline significance (P = 0.051). However, this phenomenon may have been a result of scheduling early elective surgery after confirming fetal viability (36.2 ± 2.0 vs. 38.7 ± 1.7, weeks, data not shown) to avoid the risk of uterine rupture during labor.
In conclusion, a history of ectopic pregnancy, abortion, and OHSS may be meaningful risk factors for subsequent HP in the setting of IVF-ET. The surgical treatment of HP-tube does not appear to affect the rates of early pregnancy loss or live birth. However, more data are needed to clarify the pregnancy outcomes after HP-interstitial. Regardless, medical professionals should consider sharing these findings with patients who are scheduled to undergo surgery for HP.
 XML Download
XML Download