

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Streptococcus pneumoniae is a leading cause of invasive bacterial infection in children. The invasiveness and antibiotic resistance pattern of pneumococcus vary according to serotype (1). After the introduction of the 7-valent pneumococcal conjugate vaccine (PCV7, Prevnar, Wyeth, Collegeville, PA, USA), the annual incidence of invasive pneumococcal disease (IPD) caused by the PCV7 serotypes decreased. However, replacement by non-PCV7 serotypes has been observed, and pneumococcus has caused significant morbidity despite the reduction of PCV7-type IPD. In 2010, a 13-valent conjugate vaccine (PCV13, Prevnar-13, Pfizer, New York, NY, USA) replaced PCV7 for use during routine immunization in children (2), and by June 2013, the incidence of IPD, especially that caused by the PCV13 minus PCV7 serotypes, was further reduced across all age groups in the USA (3).
In Korea, S. pneumoniae is the most common cause of invasive bacterial infections in immunocompetent children aged 3 months to 5 years (4). PCV7 was first introduced in Korea in November 2003 for optional use in the private sector, and the estimated PCV7 coverage rates among children aged 7–83 months increased from 44.8% to 73.8% for the 3-dose infant series and from 31.3% to 50.8% for the toddler dose from 2006 to 2010 (5). Although PCV7 was available as an optional immunization, a multicenter study between 2006 and 2010 revealed a significant reduction in the proportion of PCV7 serotypes and a significant increase in non-PCV7 serotypes (especially 19A) isolated from children with IPD (6). In June 2010, the 10-valent pneumococcal conjugate vaccine (PCV10, Synflorix®; GlaxoSmithKline, Brentford, London, UK) and PCV13 replaced PCV7 in Korea. In May 2014, both PCV10 and PCV13 were included in the national immunization program for children under 60 months of age.
The purpose of this study was to analyze the early changes in the serotype distribution of pneumococcus isolated from Korean children with invasive disease during the 3-year period following the introduction of the 10- and 13-valent pneumococcal conjugate vaccines (PCVs) in Korea.
MATERIALS AND METHODS
Study design
From January 2011 to December 2013, twenty-five hospitals located throughout Korea participated in this study. Children under 18 years of age with IPD were included in this study. IPD was defined as the isolation of S. pneumoniae from a normally sterile body fluid (e.g., blood, cerebrospinal fluid, pleural fluid, joint fluid, or ascites). A standardized case report form was used to collect information. The demographic data, comorbid disorders, clinical diagnoses, and outcomes were collected. The comorbid disorders were classified according to the recommendations of the Advisory Committee on Immunization Practices (ACIP). In the current study, the following conditions were considered risk factors for pneumococcal infection: chronic heart disease, chronic lung disease, cerebrospinal fluid leaks, cochlear implants, functional or anatomic asplenia, and weakened immunity secondary to chronic renal failure and nephrotic syndrome, the administration of immunosuppressive drugs, or congenital immunodeficiency (2).
Serotype determination
A total of 75 pneumococcal isolates obtained from IPD patients were prospectively collected and subjected to serotype determination. Each isolate collected from participant centers was sent to the main study center (Seoul National University Children’s Hospital), and serotype determination was performed using the Quellung reaction and antisera (Statens Serum Institut, Copenhagen, Denmark). One isolate failed to regrow, and the serotype was determined using 8 sequential multiplex polymerase chain reactions (PCRs) (78). As previously described, to assign serotypes 6C and 6D, all serogroup 6 strains were screened for the wciNβ and wciP genes (9).
The serotypes 4, 6B, 9V, 14, 18C, 19F, 23F, and 6A were classified as PCV7 types. The PCV13 minus PCV7 types included 5 additional serotypes: 1, 3, 5, 7F, and 19A. The non-PCV13 types included all other serotypes (310).
The serotype distribution was analyzed according to age, the presence of comorbid disorders, clinical diagnosis, and outcome. Trend analysis was performed by year.
Statistical analysis
The statistical analyses were performed using SPSS software version 22.0 (IBM, Armonk, NY, USA). The rates and proportions were appropriately compared using either the χ2 test or Fisher’s exact test. For trend analysis, a linear-by-linear association model was used in addition to the Pearson χ2 test. A P value < 0.05 was considered statistically significant.
RESULTS
Patient characteristics
A total of 105 episodes of invasive pneumococcal infections was identified during the study period. Among these cases, 75 isolates (71.4% of the total) were collected from consenting participants for inclusion in the study. The breakdown according to year was as follows: 24 cases in 2011, 33 cases in 2012, and 18 cases in 2013.
The male-female ratio in the current study was 1.08:1 (39:36). The percentage of patients separated by age group was 40.0% (30 cases) aged 0-23 months, 42.7% (32 cases) aged 24-59 months, and 17.3% (13 cases) aged ≥ 60 months. Twenty-four patients (32%) were at increased risk of pneumococcal infection (10 patients received immunosuppressive drugs, 4 had chronic heart disease, 3 had chronic renal failure or nephrotic syndrome, 2 had congenital immunodeficiency, 2 had cerebrospinal fluid leak, 2 had cochlear implants, and 1 had chronic lung disease). The clinical diagnoses were pneumonia (i.e., bacteremic pneumonia or empyema; 28 cases), bacteremia without focus (22 cases), meningitis (19 cases), osteoarthritis (4 cases), and peritonitis (2 cases). Because 5 cases were transferred to other hospitals not participating in this study, outcomes were known for only 70 patients. Fifty-five participants (78.6%) recovered without complication, 10 participants (14.3%) had complications (i.e., hearing loss, developmental delay, or decreased pulmonary function), and 5 participants (7.1%) died.
Serotype distribution of invasive pneumococcal isolates
The most common serotypes in the current study were 19A (32.0%), 10A (8.0%), 15C (6.7%), 6A (5.3%), 11A (5.3%), 15B (5.3%) and 23A (5.3%). The PCV7 types accounted for 14.7% of the total isolates: serotype 6A (5.3%), 19F (2.7%), 23F (2.7%), 6B (1.3%), 9V (1.3%), and 14 (1.3%). The PCV13 minus PCV7 types accounted for 32.0% of the total isolates; however, only serotype 19A was in this group. No isolates belonging to additional PCV10 serotypes (1, 5, and 7F) were observed. The non-PCV13 types accounted for 53.3% of the total isolates (Table 1).
Table 1
Serotype distribution of invasive pneumococcal isolates from children by year

Temporal changes of serotype distribution
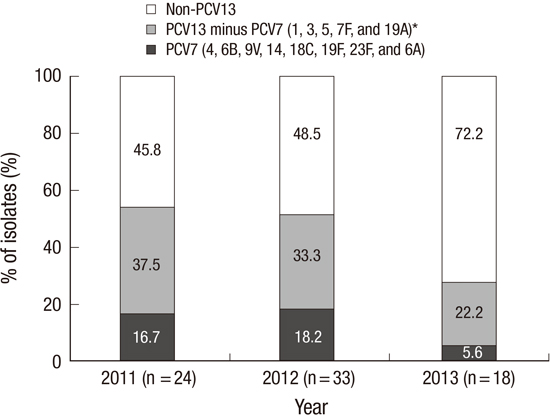
The proportion of isolates that were the PCV7 type was 16.7% in 2011, 18.2% in 2012, and 5.6% in 2013. The proportion of PCV13 minus PCV7 type (as noted above, serotype 19A was the only serotype identified in this study) decreased from 37.5% in 2011, to 33.3% in 2012 and to 22.2% in 2013; however, this trend was not statistically significant (P = 0.309). The proportion of non-PCV13 types was 45.8% in 2011, 48.5% in 2012, and 72.2% in 2013 (P for trend = 0.108) (Fig. 1). Among the non-PCV13 type isolates, the proportion of serotype 15C increased from 4.2% in 2011 to 22.2% in 2013 (P = 0.036) (Table 1).
Serotype distribution according to clinical characteristics
According to the age group, the proportion of non-PCV13 types exhibited no differences (50.0%-56.7%). However, when comparing the results from the group aged 0-23 months with the group aged 24-59 months, the proportion of PCV7 types (23.3% vs. 3.1%, P = 0.024) and PCV13 minus PCV7 types (20.0% vs. 46.9%, P = 0.033) exhibited significant differences (Fig. 2).
Fig. 2
Serotype distribution of invasive pneumococcal isolates from children according to vaccine serotype by age group.
*In PCV13 minus PCV7 types, only serotype 19A was recovered; †mo, months.

With respect to host comorbidity, among 51 participants not at risk of pneumococcal infection, PCV7 types and PCV13 minus PCV7 types accounted for 17.6% and 37.3%, respectively. The proportions were slightly lower among the 24 participants at increased risk of pneumococcal infection; the PCV7 types and PCV13 minus PCV7 types accounted for 8.3% and 20.8%, respectively. The proportions of non-PCV13 types were significantly different: 45.1% among those without risk factors compared with 70.8% among those with risk factors (P = 0.037). Among participants without risk factors for pneumococcal infection, 19A (37.3%), 10A (11.8%), 15C (9.8%), and 6A (7.8%) were the most common serotypes. However, serotypes 19A (20.8%), 11A (12.5%) and 15A (12.5%) were the most common serotypes in participants at increased risk of pneumococcal infection (Fig. 3).

The distribution of the serotypes was also analyzed according to the clinical diagnoses. In the groups of patients with bacteremia without focus (n = 22), the PCV7, PCV13 minus PCV7, and non-PCV13 types accounted for 18.2%, 27.3%, and 54.5% of isolates, respectively. In the meningitis group (n = 19), the PCV7, PCV13 minus PCV7, and non-PCV13 types accounted for 15.8%, 5.3%, and 78.9% of isolates, respectively, and in the pneumonia group (n = 28), the PCV7, PCV13 minus PCV7, and non-PCV13 types accounted for 7.1%, 53.6%, and 39.3% of isolates, respectively.
There were 5 case fatalities: 2 deaths attributable to 19A and 1 death attributable to each 6C, 10A, and 23A. The case fatality rate of serotype 19A infection was 8.7% (2 fatal cases among 23 cases with known outcomes).
DISCUSSION
This study reports the early changes in the IPD serotype distribution among children during the 3-year period following the introduction of PCV10 and PCV13 as optional immunization in the Korean private sector. In addition to reporting the early impact of these extended-valent vaccines, this study also surveyed the period before routine vaccination with PCV10 and PCV13 in Korea. PCV10 and PCV13 were first introduced as optional immunizations in June 2010, and 4 years later, in May 2014, both vaccinations were included in the Korean national immunization program.
From January 2011 to December 2013, 75 IPD cases from 25 hospitals were included in this study. Eighty percent of the participants with IPD were aged 3-59 months, and 32% of these participants had a comorbidity that predisposed them to pneumococcal infection. The PCV7 types (including serotype 6A) accounted for 14.7% of the total isolates tested, and the PCV13 minus PCV7 types accounted for 32.0% of the total isolates tested. Serotype 19A was the only serotype found among the PCV13 minus PCV7 types and was the most common serotype (32%). Although statistically insignificant, the proportion of serotype 19A decreased from 37.5% in 2011 to 22.2% in 2013 (P = 0.309), and the proportion of non-PCV13 types increased from 45.8% in 2011 to 72.2% in 2013 (P = 0.108).
In Korea, PCVs had been used as optional immunizations for 11 years before PCV10 and PCV13 were made part of the national immunization program in 2014. Korea has been a unique environment for the development of pneumococcal infection. According to the results of a retrospective single-center study, the percentage of pediatric IPD cases caused by serotype 19A increased even prior to the introduction of PCV7 in 2003: from 0% between 1991 and 1994 to 18% between 2001 and 2003. Some experts speculate that the increased incidence of pediatric IPD infection caused by serotype 19A may be associated with the antimicrobial selection pressure in Korea (11). After optional immunization with PCV7, a retrospective multicenter study suggested a decreased percentage of PCV7 isolates (excluding 6A) from 62.5% in 2006 to 21.4% in 2010. Furthermore, the percentage of the PCV7 plus 6A types decreased from 65.6% in 2006 to 28.6% in 2010, and the percentage of PCV13 minus PCV7 types (1, 3, 5, 7F, and 19A) increased from 18.8% in 2006 to 39.3% in 2010. According to this same study, the proportion of serotype 19A increased from 15.6% in 2006 to 35.7% in 2010 (6). The current study, which examines the period after the introduction of optional immunization using PCV10 or PCV13 in 2010, demonstrated a further decrease in the proportion of PCV7 types (plus 6A) from 16.7% to 5.6% and a decrease in the proportion of PCV13 minus PCV7 types (serotype 19A) from 37.5% in 2011 to 22.2% in 2013.
The impact of extended-valent PCVs, especially PCV13, has also been reported in other countries. In the United States three years after the introduction of PCV13, the incidence of IPD decreased by 64% among children younger than 5 years, with a 93% decrease in the PCV13 minus PCV7 serotype. Additionally, the proportion of PCV13 minus PCV7 types changed from 59% to 28% (3). In England and Wales, the incidence of IPD decreased by 46% in groups aged < 2 years and 48% in those aged 2-4 years. Additionally, the incidences of six other serotypes covered by PCV13 were 89% and 91%. The incidence of the additional six serotypes covered by PCV13 decreased from 59.4% to 11.7%, four years after introduction of PCV13 (12). In the current study, the proportion of the PCV13 minus PCV7 types in Korea was 37.3% from 2009 to 2010 (6) and decreased to 22.2% in 2013. This change is smaller than that observed in other countries, which may be because PCV was not initially included in the Korean national immunization program. As an optional form of immunization, parents choosing to have their children immunized with PCV were required to cover the full cost of the immunization. Thus, because of cost and lack of awareness, the PCV coverage rate was lower than that of vaccines included in national immunization program. Although we do not know the exact vaccination rates for each of PCV10 and PCV13 during 2011-2013 in Korea, the overall PCV coverage rate in 2010 was 73.8% for the infant series and 50.8% for the toddler dose and there should be no great change during the 3 year-study period when the vaccine were administered as an optional vaccine given in the private sector (5). Therefore, the impact of the vaccine might have been smaller than in other countries where the vaccine was routinely administered.
To support this, we tried to investigate the vaccination history of the patients with vaccine type pneumococcal infection. In 11 cases with PCV7 serotype infection, 8 cases were known of vaccination history and all of them were incompletely vaccinated. In PCV13 minus PCV7 serotype infection, 19 out of 24 cases were known of vaccination history. Twelve cases were unvaccinated or vaccinated with only PCV7, and 4 cases were incompletely vaccinated with PCV13. Three cases were not at risk of pneumococcal infection and were fully vaccinated according to ACIP guideline; 2 cases with 3 primary doses of PCV7 and 1 booster dose of PCV13, and 1 case with 4 doses of PCV7 and 1 supplement dose of PCV13. Therefore, among 27 cases of PCV13 serotype pneumococcal infection with known vaccination history, there were no cases who received full (primary and booster) series of PCV13 vaccination.
Also, according to the age group, the proportion of PCV13 minus PCV7 serotypes was highest in the group aged 24-59 months. This age group had more chance to get PCV7 other than extended-valent vaccines in the study period. Among the 32 IPD cases aged 24-59 months, 26 cases were known of vaccination history and 15 cases were unvaccinated or vaccinated with only PCV7, while 11 cases were vaccinated with at least one dose of PCV13. On other hands, among the 30 IPD cases aged 0-23 months, 26 cases were known of vaccination history and 8 cases were unvaccinated, while 3 cases were vaccinated with PCV10 and 15 cases were vaccinated with PCV13.
In the United States, the changes in pneumococcal serotypes after the introduction of PCV13 was also associated with change in the epidemiology of IPD clinical features. Furthermore, the incidence of pneumococcal meningitis remains unchanged, and pneumococcal meningitis accounts for a relatively larger proportion of IPD after the introduction of PCV13 (313). Decreases in pneumonia and bacteremia, but not meningitis, were also reported in Spain (14). In our study, although there were fewer cases of meningitis than bacteremia or pneumonia, the proportion of non-PCV13 (78.9%) was the highest among meningitis cases. This finding may suggest that following the continued administration of PCV13 the potential decrease in the incidence of meningitis may be less than that of other diseases.
Although the annual incidence of IPD caused by PCV13 types has decreased, there remains concern about the emergence of IPD due to non-PCV13 serotypes (12). Furthermore, there is an increase in the prevalence of underlying disorders contributing to illness among patients with IPD (3). Among patients with comorbidities associated with increased pneumococcal infection, several non-vaccine serotypes might emerge as important causes of IPD (15). Similar findings are observed in the current study; 32% of IPD patients exhibited risk factors for pneumococcal infection, and among these patients, the proportion of non-PCV13 types (70.8%) was larger than that (45.1%) among those without increased risk.
This study has several limitations. First, this study was not population-based; therefore, only proportions of isolates were evaluated, and the incidence was not estimated. However, the 25 centers included in this study are regional representative hospitals located throughout Korea; thus, we believe that the results of this study approximate the common pattern of pneumococci serotype distribution among Korean children. Second, the study period was too brief to examine the trend of serotype changes after the introduction of extended-valent vaccine. Additionally, the statistical power of the results was small. However, to evaluate any further impact of routine immunization with PCV as recommended by the Korean national immunization program, understanding the pre-routine use of extended-valent vaccines was indispensable. Third, large proportions of missing pneumococcal isolates were noted (28.6% or 30 of 105 IPD cases), which could represent a discrepancy between the current study and real-world findings.
However, despite these limitations, because Korea did not routinely survey pneumococcal infection before PCV was made part of the national vaccination program in 2014, the current study reports the most significant epidemiologic data examining pediatric IPD during the early period of optional use of extended-valent PCVs in Korea. Serotype 19A continued to be the most common serotype for IPD in children; however, the proportion of 19A seemed to decrease, and non-vaccine serotypes seemed to emerge as an important cause of IPD. In the future, surveillance studies will be needed to evaluate the impact of PCVs, which are now a part of the national immunization program in Korea. Additionally, efforts to develop more effective pneumococcal vaccines for children must continue.
 XML Download
XML Download