

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
The OECD (Organization for Economic Cooperation and Development) reported that the quality of healthcare services of its member states have, on average, improved each year and that medical demands are also on the rise (1). Along with such enhancement of the quality and quantity of healthcare services, medical malpractices are also increasing. It was reported that 7 million cases of medical malpractices occur each year, drawing attention to the danger of medical malpractices occurring in healthcare settings (2). Such medical malpractices may lead to litigation, and efforts to resolve such medical lawsuits incur socio-economic loss and may hurt the public image of the involved medical facility along with mistrust thereof, impairing its relationship with patients (3). A notable example occurred in Korea, after a medical procedure lead to the death of a famous Korean entertainer, the hospital took a defensive attitude and distorted the facts, damaging its public image and incurring significant socio-economic losses.
This increasing number of medical accident lawsuits was mentioned in the IOM (the Institute of Medicine)'s report on ‘To Err is Human' and was attributed to the fact that healthcare providers lacked communication skills in responding to medical malpractice (4). It was also indicated that doctors and other relevant medical personnel are afraid that admitting their mistakes and apologizing may lead to their reputation being damaged or getting their licenses revoked. Such concerns lead to healthcare providers merely preparing for legal action while avoiding direct communication with the victims or the victims' families (56).
With lack of communication after the occurrence of medical malpractice being shown to create problems, relevant experts have conducted research on the relationship between communication and the occurrence of medical malpractice. Several researches indicated effective communication between patient and the medical team improved doctor-patient relationship and had positive effects on treatment results (78). Further, it was reported that efforts to communicate with the victims or their families immediately after the damage-inducing procedure led to earlier settlements, reducing the possibility of developing into lawsuits, and helped improve doctor-patient relationship (910). When medical lawsuits do occur, delivering sufficient information to patients, and actively communicating with patients had significant impact on doctor-patient relationship (61011). As previously mentioned, previous studies on medical malpractice were limited to doctor-patient communication during diagnosis or patient interviews (1112).
There is a dearth of research regarding changes in doctor-patient relationships in accordance to crisis communication strategies in response to medical malpractice situations. In over 30 states in the USA the “I'm sorry law” was enacted along with the implementation of the “disclosure program”, leading to a decrease in medical litigation. Also, six Veterans Affairs Medical Centers in Kentucky, Tennessee, and West Virginia began to organize and operate a medical mistake disclosure and apology program in 1987. This program revealed that communicating directly with patients and acknowledging their mistakes was a more effective strategy than seeking to evade their responsibilities for medical accidents (13). However, research is lacking on whether the implementation of the apology strategy contributed directly to reducing medical lawsuits.
Research on communication strategies during crisis situations was conducted mostly in the business management field or the government sector in relation to image restoration and trust improvement (1415). In recent years, such research is being conducted with the focus on situational changes associated with efforts for communication, which reports that the apology strategy, amid crisis situations, has significant impact (1617). Still, the effects of the apology strategy in all crisis situations is under debate. Some studies reported that when the cause of the crisis is natural, by a third party or other external factors, the denial strategy is effective, and that depending on the degree of responsibility, apology, denial and ingratiation strategies have varying effectiveness (1819).
In particular, studies with a focus on medical accidents often examine doctors' personal perception of medical accidents; thus, there is a need to measure changes before and after medical accidents so as to analyze the effectiveness of apology strategies in an empirical research setting. During the occurrence of medical malpractice, the apology strategy moderated patient's anger, sense of responsibility, and attitude, while the doctor's active response improved patient's satisfaction, adaptation, and understanding (61020). Yet, the strategy's impact on the improvement of doctor-patient relationship needs to be verified.
Hence, this study sought to measure relational changes in medical malpractice situations according to crisis communication strategies to prove that the crisis communication strategies have causational relationships in triggering doctor-patient relationship changes. Due to the assumption that crisis communication strategies may bring about different results according to types of medical facilities, this study is focuses on medical malpractice situations at primary medical institution.
MATERIALS AND METHODS
Selection of subjects and methodology
In this study, experiments were conducted to verify the message delivery power and the reliability of the results. Subjects consisted of males and females in their 20s, 30s, 40s, and 50s. A total of 116 subjects was divided into four groups, each group consisting of 20 or more people, with consideration for demographic ratio and statistical reliability.
The relational scale was premeasured for each subject with the same metric. Further, the experimenter gave the subjects thorough explanations about the scenarios and apology message to ensure understanding on the subject. To prevent group bias, an experimenter was assigned to each group who was responsible for answering any questions given within each group. To measure the survey, the subjects were then divided into four groups where each group read different medical malpractice scenarios and communication strategy messages after which their relational scales were measured again. In re-measuring the relational scale, the order of questions was randomly recomposed to minimize order bias (Fig. 1).
Scenarios of medical malpractices and development of health communication strategies
The process of selecting medical malpractice scenarios is as follows. First, 1,400 cases of medical malpractices caused at primary medical institution, filed with Korean Medical Association Mutual Aid from 2010 to 2012, were examined to analyze the department of diagnosis, area of diagnosis, medical act, and circumstance of medical error. Of these cases, departments and medical acts that may skew to specific gender or age group such as dermatology, urology, and plastic surgery were excluded. From the remaining, the case with the highest frequency of occurring was chosen for Scenario I. The scenario was written focusing on the medical act, and the course of events. The case selected for the Scenario I was the diagnosis of acute keratitis caused by injuries associated with the examination device during a cataract surgery at an ophthalmology clinic. This scenario was classified as medical malpractice caused by “direct medical procedure”. Although medical malpractice arising from non-medical-procedure-related device malfunction does not frequently occur, due to a relatively high-profile case involving such a situation, Scenario II illustrated such a situation. Scenario II was constructed as the same form as Scenario I. The accident in Scenario II resulted in fractures, caused by poor bed railings. The patient was undergoing physical therapy and when attempting to climb out of bed, the bed railing gave out, causing the patient to slip on the floor. Scenario II was classified as “indirect medical malpractice.”
Derived from Coombs's six response strategies (18), this study chose denial, apology, and ingratiation. Four responses were created by combining ingratiation strategy with denial strategy, and ingratiation strategy with apology strategy. The denial strategy was given to mean that the physician asserted that no crisis existed and reacted with corresponding behaviors. The apology strategy showed the physician attempting to seek forgiveness from the victim regarding the crisis, and to mention future corrective actions. The ingratiation strategy was intended to remind the victim of the past good deeds of the physician. With the assumption that the crisis situation was caused at the patients' primary medical institution, the overall communication strategy contents was presented as if the doctor is delivering messages to the patient orally. Each medical malpractice scenario and communication strategy message was designed to consist of around 300 characters, using the same wording, and was equally delivered to each subject. All message contents were written out to be easy for subjects to understand, and proofread by a specialist in journalism and mass communication.
Questionnaires and statistical methods
Four types of questionnaire were developed for the four communication strategies to analyze the difference. The questionnaires included 6 questions of sociodemographic characteristics, 12 questions of manipulation verification, and 18 questions of measurement variables.
Sociodemographic characteristics included sex, age, education level, marital status, income, the number of visits to the primary medical institution. Questions for manipulation verification included those used in the research of Coombs and Holladay (21) and Lee (22), such as three responsibility verification questions, three apology verification questions, two denial verification questions, and four ingratiation verification questions. Each questions was measured by the 7-point Likert scale, ranging from “Not at all” (1 point) to “Very much so” (7 points). The 12 questions were measured immediately after subjects read the communication strategy messages, and the results were analyzed using the two sample t-test between message samples. The doctor-patient relationship measurement variable used Hon & Grunig's public-organization relationship measurement tool. Hon and Grunig (23) suggested that when a crisis arises to determine the relationship between the public and organization, six relational dimensions involving trust, control mutuality, commitment, satisfaction, exchange relationship, and public relationship should be measured. Questions from Hon and Grunig consisted of 11 trust questions, 8 control mutuality questions, 8 commitment questions, 8 satisfaction questions, 7 exchange relationship questions, four public relationship questions, totaling 46 questions. In order to assess doctor-patient relationship, four scales for trust, control mutuality, commitment, and satisfaction were used for this study. Trust entails its degree and continuity in a relationship, commitment means efforts to maintain relationships, satisfaction signifies mutual positive expectation and affection, and control mutuality means equality of power and decision making within relationships (24). Questions consisted of Hon and Grunig's short scale questions with six questions on trust, four for control mutuality, four for commitment, and four for satisfaction, totaling 18 questions (23). The 7-point Likert scale, ranging from “Not at all” (one point) to “Very much so,” (seven points), was used.
All data analysis was conducted through using the statistical program SPSS 21.0 and expressed in terms of average and standard deviation. Demographic characteristics for each group were measured using chi-square test and Fisher's exact probability test; differences in initial relationship scale between groups were measured using one way ANOVA; the interaction of major effect variables was measured using Repeated Measure ANOVA. All statistical levels of significance were set at P < 0.05.
RESULTS
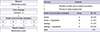
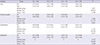
Table 1 presents the results of the manipulation verification of whether or not the two medical malpractice messages and the three communication strategy messages, as major variables in this study, were properly written out to be suitable for the purpose of this research. The analysis found that Scenario I (mean = 6.30), compared to Scenario II (mean = 5.65), showed higher responsibility, and in both scenarios, the average score of case groups (Denial = 4.73 [I], 4.44 [II]; Apology = 5.13 [I], 4.64 [II]; Ingratiation = 3.21 [I], 3.69 [II]) using the denial, apology or ingratiation strategies, were higher compared to the control groups (Denial = 3.16 [I], 3.16 [II]; Apology = 1.87 [I], 2.70 [II]; Ingratiation = 2.73 [I], 3.21 [II]) without using the strategies, making the results statistically significant. This confirmed that the subjects understood the level of mistake by the health professional and the communication strategy used in each scenario and thus were manipulated to fit the purpose of this research.
Table 1
Manipulation verification between health communication strategy messages (Unit = Mean [SD])
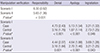
Table 2 presents the general characteristics of 116 subjects. Group A (denial) consisted of 28 subjects, Group B (denial + ingratiation) consisted of 31, Group C (apology) consisted of 31, and Group D (apology + ingratiation) consisted of 26; as such, a cross analysis of general characteristics by group showed no statistical difference, confirming that subjects were homogeneously divided into four groups.
Table 2
Sociodemographic characteristics (n = 116)
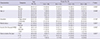
Table 3 presents the degree of subjects' usual relationships with the primary medical institution. Groups A and B showed the highest control mutuality score (mean = 4.71, mean = 4.55), Group C showed the highest trust score (mean = 4.40), and Group D showed the highest satisfaction score (mean = 4.47). The initial relationship scale was analyzed using one-way ANOVA to confirm homogeneity with the relationship scale measured after the application of communication strategy, revealing that trust, control mutuality, commitment, and satisfaction all did not show a statistically significant difference in the relationship scale for all four groups. This confirmed that homogeneity could be maintained between the first relationship scale and the relationship scale after the application of communication strategy.
Table 3
Baseline characteristics between groups (Unit = Mean [SD])

The changes between the usual doctor-patient relationship scale and the relationship scale after the application of communication strategy in Scenario I are presented in Table 4. Changes in the relationship scale before and after the application of the communication strategy in the four groups were analyzed through repeated measures ANOVA. As a result, the difference in the level of trust between groups was statistically significant (F = 4.226), and an ex post analysis of changes between groups found that there was a difference between Group A (denial) and Group C (apology). The relationship scale change over time showed a statistically significant difference (F = 153.739), and there was also a significant difference in the interaction between groups and measurement time (F = 8.080). Control mutuality was statistically significant when there was a change in the relationship scale over time (F = 100.708), and as well as the interaction between groups and measurement time (F = 8.824). For commitment, a significant difference in the change in relationship scale over time was found (F = 87.837). There was also a significant difference in the interaction between groups and measurement time (F = 9.815). The difference in the level of satisfaction between groups was statistically significant (F = 5.108), and an ex post analysis of the difference between groups revealed a difference between Groups A and B, and Group C. A change in relationship scale over time was significantly decreased after the application of the communication strategy compared to before the application (F = 132.464), and there was a significant difference in the interaction between groups and measurement time (F = 8.723).
Table 4
Comparison of relationship scales between groups on Scenario I
In sum, when employing communications strategies after a medical malpractice case, the apology strategy (line C) is more effective than the denial strategy (line A) in terms of trust, control mutuality, commitment, and satisfaction. When using the ingratiation strategy, it was found to be effective when used with the denial strategy (line B) but was ineffective when used with the apology strategy (line D) (Fig. 2). Therefore, it can be said that the most effective strategy to improve doctor-patient relationship is the use of only the apology strategy.
Fig. 2
Comparison of relationship scales between groups and time.
Group A, Denial; Group B, Denial + Ingratiation; Group C, Apology; Group D, Apology + Ingratiation.
*
P < 0.01.

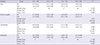
Table 5 presents an analysis of the change in usual doctor-patient relationship scale and the post-strategy relationship scale for Scenario II. The relationship scale changes, over time, for the four groups before and after the application of the communication strategy, were analyzed through repeated measures ANOVA. As a result, trust was statistically significant when there was a change in the relationship scale over time (F = 29.993), as well as the interaction between groups and the measurement time (F = 5.768). For control mutuality, a significant difference in the change in relationship scale over time was found (F = 21.157). The interaction between groups and measurement time showed a significant difference (F = 9.081). For commitment, the relationship scale change over time (F = 29.100), and the interaction between groups and measurement time were statistically significant (F = 8.301). In the case of satisfaction, the inter-group difference was statistically significant (F = 2.723), and an ex post analysis of the inter-group difference found a difference between Groups A and B, and Groups C and D. The relationship scale change over time was statistically significant (F = 48.088), and the interaction between groups and measurement time showed a significant difference (F = 5.638).
Table 5
Comparison of relationship scales between groups on Scenario II (Unit = Mean [SD])
The apology strategy (line C) is more effective than the denial strategy (line A) in terms of trust, control mutuality, commitment, and satisfaction, the improvement in control mutuality and commitment is especially notable. When using the ingratiation strategy with the apology strategy (line D), it was found to be effective for trust and commitment but did not produce any change for control mutuality and satisfaction (Fig. 2). Therefore, it was found that the most effective strategy to improve doctor-patient relationship was using the apology strategy along with ingratiation.
DISCUSSION
Since the occurrence of medical malpractice cannot be forecasted, and can inflict direct damage to humans, public relationship management can be especially complicated. Given that even primary medical institution are experiencing an increasing number of medical malpractices due to the complexity and specificity of medical acts (25), medical malpractice can arise from any medical act or in any medical institution and in various degrees of seriousness. Amid such crisis situations, the importance of communication between medical personnel is emphasized in an effort to improve the doctor-patient relationship. In addition, aside from the direct physical damage caused to patients, even before such direct damage was caused, a clear explanation on consequence should be given to the patient, including follow-up steps for preventative measures to avoid the recurrence of accidents (26). This study was based on health communication strategies proposed by Mazor et al. (26) and Elsbach (27) for medical accidents that frequently occur in primary medical institutions. The doctor-patient relationship scale was measured before and after crisis occurrence and the interaction effects of response strategies were analyzed.
Examining the results for the analysis of repeated measures ANOVA of keratitis accidents, which are classified as direct medical malpractice (Scenario I), and of fall accidents caused by faulty beds, which are classified as indirect medical malpractice (Scenario II), the apology strategy, compared to the denial strategy, had a smaller average difference in, control mutuality, commitment, and satisfaction before and after the communication strategy, and had a significant interaction effect between the communication strategy and the time passage before and after the strategy. These findings are similar to the results of Itoh and Andersen's research (6) where the apology strategy boosted the victim's acceptance of apologies to 55% (mild) and 38% (severe) in the two scenarios of fatal medical malpractices and non-fatal ones, respectively. Also, given that the doctor's responsibility or non-responsibility for accidents did not make a difference in changing the patient's perception of the incidents, but reduced the patient's monetary demands, negative ex post acts, and anger (10), the doctor's admission of his or her responsibility and expression of regret and avowal to prevent the recurrence of the accident may have positive effects on the victim. In crisis situations, the apology strategy, compared to the denial strategy, is effective in improving the doctor-patient relationship, and it was found to be more effective for Scenario II than for Scenario I.
Scenario I is similar to the results of research by Grappi and Romani (17). They reported that, with regard to preventable crises, the apology strategy, compared to the denial strategy and the excuse strategy, can be more effective in reducing the victim's anger, boosting the victim's sympathy, and alleviating the accident's social impact (17). In the case of Scenario II (medical malpractices caused by indirect medical acts) as well, the apology strategy was effective in improving all relationship scales of trust, control mutuality, commitment, and satisfaction. According to research by Coombs (16), even if the cause of a crisis is attributed to a different party, the relevant organization is deemed liable for the consequences, so the apology strategy along with an explanation about the causes of the accident is effective. Also, Liebman and Hyman (28) reported that if a doctor is not forthcoming in terms of communicating with the patient regarding a medical accident, the patient can feel angrier towards and blame the doctor; thus, a sufficient explanation of what went wrong should be given to the patient.
In cases where the causes of a crisis stem from a third party, thereby inflicting damage on the relevant organization, the denial strategy may be effective. In cases where the causes are unclear, however, the denial strategy gives the impression that the organization is evading its responsibility, possibly generating negative emotions among third parties (1929). In these studies, in both Scenario I and Scenario II, the denial strategy decreased doctor-patient relationship, but the impact factors should be differently defined according to the degree of responsibility. In Scenario I, the denial strategy had clear responsibility attribution but tended to evade the situation itself, contributing to reducing the doctor-patient relationship. In Scenario II, the denial strategy tended to transfer unclear responsibility attribution to a third party, contributing to reducing the doctor-patient relationship.
In using communication strategies with regard to crises, the apology strategy and the denial strategy, when supported by ingratiation, showed different results. Coombs (18) reported that in Scenario II wherein the causes of an accident are indirect and unintended, the ingratiation strategy is suitable, and that the public - if the organization's past achievements are positive - places high trust in the statement and tends to more readily accept the organization's apologies. But if the public does not know about an organization's past achievements during normal times and thus has a neutral opinion on that organization, the use of the ingratiation strategy will create an opportunity to generate the awareness of positive past achievements. Also, positive past achievements can boost organization-public trust, and enhances the possibility of the public accepting the organization's explanation. But positive past achievements may change depending on the public's awareness thereof, so the use of the ingratiation strategy requires careful consideration of the crisis situation at hand and the contents of the response statement.
This study verified the effectiveness of the apology strategy with regard to various medical malpractices, and found that using the ingratiation strategy with denial was effective in both scenarios, but when using the apology strategy, ingratiation was found to be effective only in specific situations. In the case of direct medical malpractice, using only the apology strategy was effective, while for indirect medical malpractice cases, using ingratiation along with apology was more effective. Above all, apology was accepted more as indication for the doctor's attempt to actively communicate with patients rather than as a means of establishing the doctor's negligence. In the research by Robbennolt as well (20), the doctor's sufficient explanation and apologies reduced the victim's anger, the organization's responsibility attribution, improved mutual trust and control mutuality, and reduced possible lawsuits over medical malpractices by 40%. As such, patients want an appropriate explanation and apologies with regard to the accident rather than monetary compensation. Yet, only a minimum level of explanation is usually given to the victims, and the apology strategy is not frequently used.
Noland and Carl (30) conducted research on doctors' communicative approach with patients regarding medical accidents by interviewing resident doctors. 40% of subjects said that they would honestly report medical accidents, but 96% of them replied that they would report to their head doctors instead of directly informing the patient involved about the accident, and that the head doctors should be responsible for the consequences (30). Also, Hannawa (31) reported, after studying doctor-patient communication problems using the physician mistake disclosure model, that if the doctor is more likely to decide that there would be less blame and criticism from others, he or she wants to have direct communication with the patient, and that the levels of mistakes in and responsibility for medical accidents have less bearing on attempts to communicate. As such, this is because the apology strategy is believed to be tantamount to admitting that the accident was caused by the doctor's negligence and that the responsibility for such a crisis is placed on the doctor, resulting in the doctor sustaining damage and experiencing tremendous psychological stress (32). But if the doctor and the patient make an attempt to address one another in a positive and constructive manner, and if the doctor expresses his or her sincere sympathy, then this will significantly reduce the number of medical disputes. Further, since the formation of control mutuality in normal times may reduce the danger of wrong diagnosis, doctors working at primary medical institution are advised to facilitate communication with patients (33). Thus it is very important to improve normal and usual relationships as well as engaging in positive communication when a crisis occurs.
Existing studies on doctor-patient communication with regard to the occurrence of medical accidents reported that communication problems mainly focused on medical centers, or have given a fragmented description of strategies employed during the occurrence of crisis situations (13263031). This study differed from risk communication research which focuses on individual characteristics (343536), but was similar to crisis communication research which focuses on the organization-public relationships (637). It also verified the effectiveness of apology strategies, focusing on patients in the event of medical accidents. Due to the thorough explanation given to subjects about the scenario and communication strategy, the subjects were able to realistically experience the situations which provide realistic data for the purpose of this research. In order to secure the reliability of the data and homogeneity between research groups, the difference in response strategies by socio-demographic characteristics was not analyzed.
Since the sample size was not sufficiently large due to the difficulty of controlling subjects, the representativeness of the findings of this study may be limited. Although medical malpractices with the highest frequency of occurrence were selected from among those registered with Korean Medical Association Mutual Aid, the two scenarios, designed in this study, does not sufficiently represent all medical malpractice situations since medical malpractices are unintended and are related to particular situations. Thus, in addition to classifying crisis situations into direct and indirect accidents according to the extent of the doctor or the patient's responsibility, there is a need to conduct communication strategy effectiveness research which includes diverse cases of medical malpractices, including cases wherein the doctor or the patient is clearly entirely responsible for the accident. While this study explored the effectiveness of the apology strategy and when coupled with ingratiation, studies researching apology strategy combined with corrective action, monetary compensation, and other diverse strategies should be further examined.
 XML Download
XML Download