

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As perinatal and neonatal care are continuously advancing, more preterm infants are surviving and being discharged from the neonatal intensive care unit (NICU) (1). However, many preterm infants who are discharged from the NICU have neonatal morbidities such as bronchopulmonary dysplasia (BPD), necrotizing enterocolitis (NEC), and hydrocephalus, which result in the use of medical resources and become risk factors for readmission (234).
A better understanding regarding the use of medical resources among preterm infants after discharge from the NICU, and identification of associated risk factors during their stay in the NICU, could facilitate discharge planning of preterm infants and education for their parents. Previous studies have reported that 40.1% of preterm infants born at <32 weeks' gestation (4) and 15% of preterm infants <36 weeks' gestation (3) were readmitted, and 22.2% of infants (5) who were born at <32 weeks' gestation visited an emergency center during the first year of life. However, those studies were focused mainly on healthcare costs and perinatal factors associated with readmission (367). To date, no nation-wide study has looked at the use of medical resources among preterm infants after discharge from the NICU in Korea.
The aim of this study was to evaluate the incidence of readmission and visits to emergency centers as well as regular or irregular visits to outpatient clinics following discharge from the NICU in preterm infants of <33 weeks' gestational age in Korea.
MATERIALS AND METHODS
This study was performed as a project entitled "Retrospective Study to Evaluate Rehospitalization & Health Care Utilization after NICU Discharge in Preterm Infant of <33 weeks' gestation (RHANPI)"
Patient population
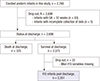
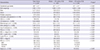
The cohort included all preterm infants born between 22 and 32 weeks' gestation who were discharged from the NICUs of 44 Korean hospitals between April 2009 and March 2010, regardless of survival or death (n=2,698). The total number of infants encompassed about two-third of annual births at <33 weeks' gestation in Korea (8). Among those infants, 2,373 (88.0%) had survived and were discharged from the NICU. After excluding 21 infants who had incomplete data collection, 2,35l infants were enrolled in this study (Fig. 1). Mean±standard deviation (SD) of gestational age (GA) of total infants was 29+4±2+1 weeks and Mean±SD of birth weight was 1,403±413 g. Perinatal and neonatal characteristics of the total infants, infants born at ≥30 weeks' gestation (infants ≥30 weeks) and infants born at <30 weeks' gestation (infants <30 weeks) are shown in Table 1.
Data collection
The Committee on Data Collection and Statistical Analysis of the Korean Society of Neonatology chose 44 NICUs in Korea. Data collection was performed by the neonatologists of the 44 NICUs retrospectively, with chart review, on the basis of standard study formats and a manual defining the variables. All data were entered electronically into a central database during the study period between August and December 2011. Collected data were checked repeatedly for quality and completeness. Information with suspected errors or missing data was fed back to the neonatologists for verification. The mean value and SD of the follow-up duration of total infants after discharge from the NICU was 425±237 days. Cumulative percent of total infants according to follow-up duration after discharge from NICU is shown in Fig. 2. The database was created in collaboration with the Clinical Research Center of Samsung Medical Center on the basis of the electronic case reporting system of Oracle Korea (Oracle Corporation, Seoul, Korea). Data variables were composed of baseline characteristics; perinatal and neonatal characteristics such as major morbidities in NICU; visits to outpatient pediatric and other departmental clinics; visits to emergency centers; and readmission factors including cause of readmission, need for oxygen and ventilator support. Regular visits were defined as pre-scheduled visits for monitoring growth and development or vaccinations, and irregular visits were defined as non-scheduled visits for solving various health problems. Readmission was defined as readmission to any hospital when it was stated in the patient's medical records. Visits to emergency centers and outpatient clinics were confined to events at the participating hospital.
Definitions of variables
BPD was defined as the need for supplemental oxygen for at least 28 days after birth and its severity is graded according to the respiratory support required at 36 postmenstrual weeks or discharge whichever comes first (9). NEC was defined as Bell's stage II or greater (10). Stage III or IV intraventricular hemorrhage (IVH) (11) and cystic periventricular leukomalacia (PVL) on cranial ultrasonogram were based upon the Papile grading system. Sepsis was defined according to the Centers for Disease Control and Prevention/National Nosocomial Infection Surveillance definitions for infants ≤12 months (12).
Statistical analysis
Categorical data are presented as numbers (%), and continuous data are presented as the mean±SD. Fisher's exact test was used to compare categorical variables and Student t-test or the Wilcoxon rank sum test was used to compare continuous variables according to normality of the data. The readmission rate was estimated by using the Kaplan-Meier product-limit method. To compare the rate of readmission among categorized gestational age groups; 25 weeks' gestation or less, 26-27 weeks' gestation, 28-29 weeks' gestation, 30-31 weeks' gestation, and 32 weeks' gestation, the log-rank test with Bonferroni's correction for post hoc testing of pair-wise comparisons was used. All statistical tests were 2-sided and P<0.05 was considered statistically significant. Data were analyzed with SAS software version 9.3 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Frequency of visits to outpatient clinic
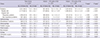
Of the total infants, 94.5% (2,221/2,351) visited pediatric outpatient clinics after discharge from the NICU. Mean value and SD of frequency of visits to the pediatric clinics was 11.5±9.8. Specifically, 92.3% of the total infants (2,170/2,351) visited pediatric clinics regularly for check-ups on growth and neurodevelopment or periodic vaccination, 42.9% (1,008/2,351) visited pediatric clinics irregularly for respiratory problems, and 38.3% (901/2,351) visited irregularly for non-respiratory problems (Table 2).
Among the total infants, 77.2% (1,815/2,351) visited ophthalmology, 37.8% (889/2,351) visited rehabilitation medicine, 19.1% (450/2,351) visited otolaryngology, and 8.5% (199/2,351) visited pediatric surgery clinics (Table 2).
Compared with infants ≥30 weeks' gestation, infants <30 weeks' gestation had more regular visits to pediatric clinics (10.5 ±7.0 vs. 6.8±5.3, P<0.001) and irregular visits to pediatric clinics for respiratory problems (5.2±6.2 vs. 4.5±7.2, P<0.001) (Table 2).
Visit to emergency center
Of the total infants, 31.1% (725/2,332) visited emergency centers after discharge from the NICU. Mean value and SD of frequency of visits to emergency centers was 2.1±1.8.
Specifically, 11.2% (170/1,516) of total visits to emergency centers resulted in the need for oxygen supplementation, and 24.7% (375/1,520) resulted in admission (Table 3); 50.8% (785/1,544) of emergency visits were due to respiratory problems.
Among the total infants, 12.4% (288/2,332) visited emergency centers for non-respiratory problems and 18.7% (437/2,332) visited emergency centers for respiratory problems. Out of 437 infants who visited emergency centers for respiratory problems, 43 infants (9.8%) were diagnosed with respiratory syncytial virus (RSV) infection (Table 3). RSV accounted for 32.4% of etiologic viruses that were confirmed on laboratory tests at the time of emergency center visits.
Infants <30 weeks' gestation, compared with infants ≥30 weeks' gestation, had more visits to the emergency centers (2.3 ±2.1 vs. 1.9±1.5, P=0.027), more frequent need for oxygen (103/763 [13.5%] vs. 67/753 [8.9%], P=0.003), and a higher probability of admission (206/769 [26.8%] vs. 169/761 [22.5%], P=0.049). However, the number of visits to emergency centers where RSV infection was diagnosed did not differ between the 2 groups (infants <30 weeks' gestation vs. infants ≥30 weeks' gestation: 23/964 [2.4%] vs. 20/1,368 [1.5%], P=0.422) (Table 3).
Readmission
Of total infants, 33.6% (788/2,346) were readmitted at least once, and the mean and SD of frequency of readmissions was 1.8±1.5. Additionally, 25.3% (333/1,314) of total readmissions needed oxygen supplementation, and 8.5% (113/1,322) needed ventilator care (Table 4).
18.4% (431/2,346) of the total infants were readmitted with respiratory problems at least once, and the mean and SD of frequency of readmissions was 1.7±1.2. Specifically, 3% (70/2,346) of total infants were diagnosed with RSV infection (Table 4). Out of the infants who were readmitted with respiratory problems, 83.9% (362/431) of them had laboratory tests done for confirming RSV infection, and RSV accounted for 30.3% of etiologic viruses that were confirmed with laboratory tests at the time of readmission.
Infants <30 weeks' gestation, compared with infants ≥30 weeks' gestation, had a higher frequency of total readmissions (2±1.7 vs. 1.7±1.2, P=0.009) and readmissions for respiratory problems (1.8±1.2 vs. 1.5±1.1, P=0.027), need for oxygen supplementation (211/733 [28.8%] vs. 122/581 [21.0%], P=0.001), and need for ventilator support (77/741 [10.4%] vs. 36/581 [6.2%], P=0.007). However, the number of readmitted infants diagnosed with RSV infection did not differ between the 2 groups (infants <30 weeks' gestation vs. infants ≥30 weeks' gestation: 37/964 [3.8%] vs. 33/1,368 [2.4%], P=1.000) (Table 4).
In the first 360 days after discharge from the NICU, 28.1% of total infants were readmitted, and 15.0% of them were readmitted for respiratory problems. At 720 days, 33.2% of total infants had been readmitted and 17.9% of them were readmitted for respiratory problems (Table 5). The younger the gestational age at birth, the higher the probability of total readmissions and readmissions for respiratory problems (log-rank test for trend P<0.001; Fig. 3). Infants born at 25 or less, and 26-27 weeks' gestation had a significantly higher probability of total readmissions and readmissions for respiratory problems following discharge from the NICU than infants 30-31, and 32 weeks' gestation (Fig. 3A and B). Infants born at 28-29 weeks' gestation had a significantly higher probability of total readmissions following discharge from the NICU than infants 30-31, and 32 weeks' gestation but did not have a higher probability of readmissions for respiratory problems than infants 30-31, and 32 weeks' gestation (Fig. 3A and B). Readmission rates at the time-point after discharge from the NICU and their 95% confidence intervals 0.001are shown in Table 5.
Of the total infants, 0.6% (14/2,351) was reported as mortality cases. Of the total mortalities, 78.6% (11/14) occurred within 12 months after discharge from the NICU.
DISCUSSION
Of the total infants in this study, 33.6% required at least 1 episode of readmission. Ralser et al. (4) reported that 40.1% and 24.7% of preterm infants born at <32 weeks' gestation were readmitted in the first and second years of life, respectively. Underwood et al. (3) also reported that 15% of preterm infants <36 weeks' gestation were readmitted at least once in the first year of life. Considering the differences in enrollment of criteria and follow-up duration with these studies, the rates of readmission in this study were similar to those in previous studies.
Of the total infants, 18.4% were readmitted with respiratory problems at least once, and respiratory problems were the most common cause for readmission. Resch et al. (13) reported that 14% of preterm infants born at 29-36 weeks' gestation were readmitted because of respiratory problems during the first 2 yr of life. Rasler et al. (4) reported that the leading cause of readmission was respiratory infection, accounting for 42.1% and 47.4% of total readmissions in the first and second years of life, respectively. A similar trend was observed for respiratory readmissions in this study.
The readmission rate for RSV infection was 3% in this study. The readmission rate for RSV in Korea has been reported to be approximately 3.1%-9.3% (14151617). The readmission rate for RSV in Korea for those studies as well as ours could be underestimated because of limited indications for laboratory tests to prove viral etiologies taking into consideration health insurance coverage. Readmission rates for RSV in preterm infants following discharge from the NICU have varied widely, from 2.7 to 37% (1819202122). This could be a result of differences in the study populations and criteria in each study. Although younger gestational age is known to be a risk factor of readmission for RSV in preterm infants (23242526), no difference in readmission rate for RSV between infants ≥30 weeks' gestation and infants <30 weeks' gestation observed in this study. In previous studies, palivizumab prophylaxis reduced severe RSV infection and readmission for RSV in preterm infants with BPD (24272829). Therefore, variations in readmission rates for RSV in preterm infants might have resulted from palivizumab prophylaxis during the study period as it was indicated for infants diagnosed with BPD within 6 months and less than 2 yr of life at the beginning of RSV season in Korea. In this study, RSV was the most common confirmed virus at the time of readmission and other respiratory viruses including rhinovirus, parainfluenza, influenza, and adenovirus were also confirmed in some cases. Drysdale et al. (30) also reported that RSV related lower respiratory tract infection (LRTI) was associated with increased readmission and other viral etiologies of LRTI were enterovirus, parainfluenza, adenovirus, human metapneumovirus, parechovirus, human bocavirus, and influenza.
Among total infants in our study, 31.1% visited emergency centers at least once and 24.7% of all emergency visits resulted in readmission, with 50.8% of those visits being due to respiratory problems. Rhein et al. (5) reported that 22.2% of infants born at <32 weeks' gestation visited the emergency centers during the first year of life. In contrast to our study, most of the visits were due to respiratory problems. This divergence might have resulted from differences in the study populations and criteria for follow-up at high-risk pulmonary or neurodevelopmental clinics in that study.
In this study, many preterm infants visited various outpatient clinics, such as pediatrics, ophthalmology, rehabilitation medicine, otolaryngology, and pediatric surgery clinics. Among the total infants, 42.9% visited pediatric clinics irregularly for respiratory problems, and 38.3% visited irregularly for non-respiratory problems. Infants <30 weeks' gestation had more regular visits to the pediatric clinic as well as more irregular visits for respiratory problems than infants ≥30 weeks' gestation. Gray et al. (31) reported that very preterm infants <32 weeks' gestation and/or had birth weight <1,500 g, had higher rate of visits to an outpatient clinic for special health care over the first 2 yr than full term infants. Korvenranta et al. (32) reported that the number of visits to an outpatient clinic during the first 3 yr of life decreased with increasing gestational age at birth in the very preterm infants <32 weeks' gestation or in those who had a birth weight of <1,501 g.
This study had some limitations, such as variable duration of post-discharge follow-up, absence of consideration of long-term complications, and retrospective design. Nevertheless, it has value as the first nation-wide study on the use of medical resources by preterm infants after discharge from the NICU in Korea. Therefore, further prospective studies on this subject are indicated.
The use of medical resources, such as outpatient clinics, emergency centers, and readmission, was common in this study population. Respiratory problems were the leading cause for the use of medical resources following discharge from the NICU. Total readmissions and readmissions for respiratory problems were more frequent in infants <30 weeks' gestation, than in infants ≥30 weeks' gestation. However, the frequency of readmissions for RSV infection was not different between the 2 groups. Therefore, optimal strategies to manage the use of medical resources are necessary in preterm infants after discharge from NICU.





 XML Download
XML Download