

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Because of the improvement of perinatal care, the mortality rate of very-low-birth-weight (VLBW) infants has been decreasing, and there has been an increase in the survival rate of extremely low birth weight (ELBW) and extremely preterm infants (123). Consequently, neonatal morbidities relating to prematurity has been increasing. Antenatal steroid therapy and early postnatal surfactant administration were considerably successful in overcoming pulmonary immaturity due to surfactant deficiency (45). However, pulmonary structural development of alveolarization and microvascular growth has been difficult to control by current treatment modalities. Therefore, bronchopulmonary dysplasia (BPD) presently remains the most prevalent and serious chronic lung problem in neonatal intensive care units (NICUs). Infants born at ≤26 weeks of gestation are especially at risk of severe BPD development in addition to mortality (126).
The significance of BPD is that it is a representative chronic lung disease in the NICU, which results in higher mortality and prolonged hospitalization. BPD is also associated with an increased risk of cardiovascular impairment, long-term pulmonary sequela, growth failure, and neurodevelopmental delay (678).
The aim of this study was to investigate the incidence and related characteristics of BPD in VLBW infants who were prospectively registered in the Korean Neonatal Network (KNN) database (9) from January 2013 to June 2014. We hypothesized that the incidence of BPD has been increasing due to the decreasing mortality in VLBW infants. To verify the recent trend in the increasing BPD rate, we also compared data related to BPD and the mortality rate of the present study with those of a previous nationwide retrospective survey on BPD that was conducted from 2007 to 2008 (10).
MATERIALS AND METHODS
Subjects
In total, 2,386 VLBW infants who were born and registered in the KNN database from January 2013 to June 2014 were included in this study. Data of VLBW infants born or transferred within 28 days of birth were registered prospectively from 55 NICUs of KNN participating hospitals.
BPD definition
BPD was defined as the need for supplemental oxygen or positive pressure support at 36 weeks postmenstrual age (PMA), corresponding moderate to severe BPD using the severity-based definition for BPD from the National Institutes of Health consensus (1112). Severe BPD was defined as the need for oxygen for >28 days plus ≥30% oxygen and/or positive pressure at 36 weeks PMA. The overall incidence of BPD was investigated.
The three possible outcomes at 36 weeks of PMA
Because we diagnosed BPD at 36 weeks PMA, the possible outcomes of VLBW infants would have been one of the following: 1) death before 36 weeks PMA, 2) survival with BPD (moderate or severe BPD group) or 3) survival without BPD (non-BPD group). Each rate of the three possible outcomes was investigated according to gestational age (by 1 week) and birth weight groups (by 250 grams). Considering the higher mortality rate among extremely preterm and low birth weight infants before 36 weeks PMA, we also determined the combined rate of BPD or death before 36 weeks PMA according to the previous gestational age and birth weight groups.
The overall mortality rate of VLBW infants in the NICU is shown separately from the death rate before 36 weeks PMA.
Characteristics and outcomes of the BPD group
We assessed the clinical characteristics and neonatal outcomes of the BPD group and compared them with the non-BPD group among surviving VLBW infants at 36 weeks PMA.
First, perinatal variables, including the maternal age, gestational diabetes, maternal hypertension, Cesarean section, histologic chorioamnionitis, and antenatal steroid treatment, were examined. Demographic characteristics and initial neonatal conditions including the gestational age, birth weight, sex, and Apgar score at 5 min, were examined. The acute perinatal lung problem of respiratory distress syndrome (RDS), pulmonary hypertension, air leak and massive pulmonary hemorrhage, and patent ductus arteriosus (PDA) were assessed. RDS was defined as the presence of clinical respiratory distress and compatible chest X-ray findings (13). A diagnosis of PDA was established in patients whose hemodynamic results warranted medical or surgical treatment. The perinatal characteristics and neonatal outcomes were compared using the chi-square and t-tests.
Second, multivariate logistic regression analyses were used to investigate whether specific perinatal conditions were associated with either an increased or decreased risk of BPD.
Finally, several important treatment outcomes of the BPD group were investigated and compared with those of the non-BPD group. The total duration of non-invasive and invasive positive pressure ventilation, total duration of oxygen administration and the PMA of the weaning date, discharge outcomes, and mortality after BPD diagnosis to discharge were examined using univariate and multivariate logistic regression analyses.
Comparison with the 2007-2008 nationwide survey
To investigate recent changes in the incidence of BPD among VLBW infants, we compared the BPD rate in the present study with the latest nationwide retrospective survey from 2007 to 2008 (10). The published results and partial available raw data from the survey (10) were used. Because the previous data were limited to only infants at 23-31 weeks of gestation (n=3,841), we also selected the same limited conditions of infants at 23-31 weeks of gestation (n=1,990 of 2,386) for comparison.
At 36 weeks PMA, three possible outcomes of the VLBW infants were compared between the two studies: 1) death before 36 weeks PMA, 2) survival with BPD (moderate and severe), or 3) survival without BPD. The overall rate of the three possible outcomes and each rate according to the birth weight groups (by 250 grams) were analyzed. The distribution of the three possible outcomes at 36 weeks PMA were compared between the two studies using the chi-square test. The combined rate of BPD or death before 36 weeks PMA and the rate of severe BPD are also shown.
The comparison of the overall mortality rate of VLBW infants in the NICU between the two studies is described separately.
RESULTS
The overall incidence of BPD
Among our study population of VLBW infants (n=2,386), 689 were diagnosed with BPD, and the overall BPD rate was 28.9%. Among the 689 BPD VLBW infants, 257 had moderate BPD (37.3%) and 432 had severe BPD (62.7%).
The overall mortality rate in the NICU was 11.9%. In the subgroup of infants with a birth weight <1,000 g (n=929), the overall BPD rate and overall mortality rate in the NICU were 42.7% and 24.2% respectively; among infants with ≤28 weeks of gestation (n=1,222), the rates were 41.4% and 20.0% respectively.
The incidence of BPD according to the gestational age and birth weight
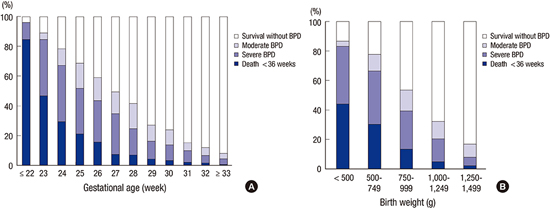
The three possible outcomes (death before 36 weeks PMA, moderate or severe BPD, or survival without BPD) of the VLBW infants at 36 weeks PMA are illustrated in Fig. 1.
BPD rates according to the gestational age groups were as follows: 11.5% at ≤22 weeks of gestation, 42.2% at 23 weeks, 48.9% at 24 weeks, 47.5% at 25 weeks, 43.1% at 26 weeks, 42% at 27 weeks, 34.3% at 28 weeks, 22.8% at 29 weeks, 20.5% at 30 weeks, 13.0% at 31 weeks, 10.3% at 32 weeks, and 7.1% at ≥33 weeks. The combined rates of BPD or death before 36 weeks PMA were as follows: 96.1% at ≤22 weeks of gestation, 88.9% at 23 weeks, 78.5% at 24 weeks, 68.7% at 25 weeks, 58.9% at 26 weeks, 49.5% at 27 weeks, 41.7% at 28 weeks, 26.9% at 29 weeks, 24% at 30 weeks, 15.2% at 31 weeks, 12% at 32 weeks, and 7.9% at ≥33 weeks (Fig. 1A).
BPD rates according to the birth weight groups were as follows: 42.4% for <500 g, 47% for 500-749 g, 39.9% for 750-999 g, 27.3% for 1,000-1,249 g, and 14.5% for 1,250-1,499 g. The combined rates of BPD or death before 36 weeks of gestation were as follows: 86.5% for <500 g, 77.5% for 500-749 g, 53.6% for 750-999 g, 32.4% for 1,000-1,249 g, and 16.8% for 1,250-1,499 g (Fig. 1B).
Characteristics and perinatal risk factors for BPD
In total, 250 infants (10.5%) died before 36 weeks of gestation, which was when BPD was diagnosed. Among the surviving 2,136 VLBW infants at 36 weeks PMA, perinatal demographic and initial neonatal characteristics of BPD are shown in Table 1. Mean gestational age and mean birth weight were lower in infants with BPD compared to non-BPD infants. There were more male infants and infants whose Apgar scores were <7 at 5 min in the BPD group than in the non-BPD group. All the frequencies of surfactant treatment, initial acute pulmonary diseases such as extrapulmonary air leaks, pulmonary hypertension or massive pulmonary hemorrhage, and significant PDA were higher in the BPD group.
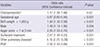
Using multivariate logistic regression analysis, histologic chorioamnionitis, a lower gestational age, birth weight <1,000 g, male sex, an Apgar score <7 at 5 min, surfactant treatment, initial acute pulmonary diseases, and PDA were associated with an increased risk of BPD (Table 2).
BPD outcomes
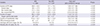
Among the surviving 2,136 VLBW infants at 36 weeks PMA, several clinical outcomes and treatment characteristics of BPD are shown in Table 3.
Among the 689 BPD infants, the total positive pressure ventilation was used for 66.8±43.5 days, and the proportion of non-invasive ventilation to total positive pressure ventilation was 0.45±0.29. Oxygen weaning was possible at 39+6±5+4 weeks of gestation after 86.4±43.8 days of treatment. The mortality rate of BPD infants after 36 weeks PMA and until discharge from the NICU was 4.6%. Their discharge was feasible at 42+0±5+3 weeks, and 24.7% of patients needed oxygen at discharge.
The association of variables (related to treatment and outcome) with the occurrence of BPD is also shown in Table 3: data were adjusted for gestational age, birth weight, male sex, the Apgar score at 5 min, surfactant treatment, PDA, and histologic chorioamnionitis.
Changes in BPD and the mortality rate compared to 2007-2008
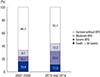
In total, 1,990 VLBW infants were born at 23-31 weeks of gestation among our total study population (n=2,386). At 36 weeks PMA, each rate of the three possible outcomes of the VLBW infants was as follows: 1) the rate of death before 36 weeks PMA was 11.3%; 2) the rate of survival infants with BPD was 33.0% (12.2% with moderate and 20.8% with severe BPD); and 3) the rate of surviving infants without BPD was 55.7% (Fig. 2). The distribution of the overall rate of the three possible outcomes at 36 weeks PMA were different (P<0.001) from those in the previous nationwide survey from 2007-2008 (10), which were 15.9%, 17.8%, and 66.3% respectively (Fig. 2). The incidence of BPD increased by 85% (from 17.8% to 33.0%) compared to that from 2007-2008 (10). The rate of severe BPD also increased by 157% (from 8.1% to 20.8%) compared to that from 2007-2008. However, the rate of death before 36 weeks PMA decreased by 28.9% (from 15.9% to 11.3%) compared to that from 2007-2008. The overall combined rate of BPD or death before 36 weeks PMA was higher compared to that from 2007-2008 (from 33.7% to 44.3%) (Fig. 2).
Separately, the overall mortality rate of VLBW infants during the entire hospitalization in the NICU decreased by 31.4% (from 18.8% to 12.9%) compared to that from 2007-2008.
At 36 weeks PMA, the three possible outcomes of the VLBW infants according to the birth weight subgroups in the present study and data from 2007-2008 (10) are shown in Table 4. The number of infants in every subgroup of birth weight by 250 g was indicated. The distribution of the three possible outcomes at 36 weeks PMA was different (P<0.001) between the two studies. The proportion of infants with a birth weight <1,000 g was higher in the present study (44.3% vs. 37.6%) than in 2007-2008. In addition, changes in the combined rate of BPD or death before 36 weeks PMA according to the birth weight are shown. The combined rate of BPD or death before 36 weeks PMA was lower in the present study than in 2007-2008 among infants with a birth weight <500 g, which was similar among infants with a birth weight 500-999 g. Among infants with a birth weight ≥1,000 g, the combined rate of BPD or death before 36 weeks PMA increased. The rate of BPD and severe BPD increased compared to those from 2007-2008 in every birth weight group (Table 4). In contrast, the rate of death before 36 weeks PMA decreased compared to that from 2007-2008 in every birth weight group.
DISCUSSION
Current data indicate an increasing number of high-risk pregnancies and simultaneously increasing rate of preterm infants (126). Further, by virtue of improvements of perinatal and neonatal care, more extremely premature infants have been surviving compared to those in the past. The risk of BPD is inversely proportional to gestational age and birth weight, so as a result, an increased incidence of BPD has been reported in other developed countries (141516). A sizeable increase of surviving premature infants has resulted in those with severe BPD (17). According to the NICHD database in 2003-2007, which used the same severity-based classification of BPD as in our study (11), the incidence of BPD and severe BPD was 41% and 18% respectively (14). In our study population, BPD developed in 28.9% and severe BPD developed in 18.1% of the total 2,386 VLBW infants.
The BPD rates showed an inverse correlation with gestational age and birth weight in infants with ≥24 weeks of gestation or a birth weight ≥500 g (Fig. 1). A lower incidence of BPD in the subgroup of infants at <24 weeks of gestation and with a birth weight <500 g is thought to result from a higher mortality rate among extremely preterm and low birth weight infants before 36 weeks PMA. Thus, the combined rate of BPD or death before 36 weeks PMA can show more accurate and objective outcomes than the BPD rate alone, especially for the tiny infant group. In the present study, the combined rate of BPD or death before 36 weeks PMA showed an inverse correlation with the gestational age and birth weight in every gestational age and birth weight group.
A comparison of the BPD rate in the present study with the latest nationwide survey from 2007 to 2008 (10) showed an increased BPD rate (from 17.8% to 33.0%) and decreased mortality (from 18.8% to 12.9%) in VLBW infants. This trend in the increasing BPD rate due to increasing surviving premature infants corresponds with results from many previous results (126141516). However, the increase in the ratio of the BPD rate was much higher than the decreased ratio of mortality. Thus, some credible speculation is needed to explain this gap.
Importantly, the distribution of gestational age among the infants of the two different studies must be considered because gestational age is most likely the strongest risk factor for BPD (18). Unfortunately, information about the distribution ratio according to the gestational age in the previous study (10) was not available, so direct statistical comparison of the outcomes with the current study was limited. Despite the limited information, we can suggest a few reasons for the possibility that the frequency of extremely preterm infants is higher in our study population. First, the proportion of infants with a birth weight <1,000 g was higher in the present study (44.3% vs. 37.6%) than in the 2007-2008 study (Table 4). Second, there was a significant increase in the incidence of severe BPD. Among the VLBW infants at 23-31 weeks of gestation, 20.8% of our total study population was diagnosed with severe BPD compared to 8.1% in 2007-2008 (Fig. 2). Third, the possible changes of perinatal characteristics such as maternal hypertension (19); fetal growth restriction (20); antenatal inflammatory conditions including chorioamnionitis (21); and failure to receive antenatal steroid treatment (22) may contribute to BPD development and severity. Possible favorable effects of antenatal chorioamnionitis and steroid treatment are decreased RDS, whereas, adverse effects include alterations in lung development and innate immune responses for the development of BPD (5). In our study, chorioamnionitis was associated with an increased risk of BPD (Table 2).
The combined rate of BPD or death before 36 weeks PMA was lower than in 2007-2008 among infants with a birth weight <500 g, which was similar among infants with a birth weight 500-999 g. Among the VLBW infants with a birth weight ≥1,000 g, the combined rate of BPD or death before 36 weeks PMA was higher in our study than in 2007-2008, which showed the opposite in infants with a birth weight <1,000 g (Table 4). This suggests that the increased range of survival rate of infants in the ≥1,000 g birth weight subgroup was not as broad as that for infants in the <1,000 g birth weight subgroup. Because BPD is a multifactorial disease in the relatively less premature subgroups, a different genetic predisposition, pathophysiology, or the contribution of associated factors to BPD may be different (23). A further separate study is required to investigate the risk factors for the development of BPD in infants with a birth weight ≥1,000 g, a BPD-uncommon subgroup.
Differences in the data collection method between the two studies should be considered. The previous study was a retrospective survey that mailed questionnaires (10), and it had limitations of data collection and quality control. The KNN data of the present study was based on a national prospective registry of VLBW infants. The quality of the data are guaranteed by data management, audit and monitoring. In case that informed consent was omitted, data could not be registered, especially if the patient was in a bad condition or had died. According to the KNN 2013 annual report, there was a discrepancy between Type I (n=1,398) and Type II (n=1,503) mortality rates (10.0% vs. 11.4%) (24) because patients without informed consent (n=105) were considered in the Type II mortality rate. To ensure that the KNN mortality rate reflects true mortality in VLBW infants, strict control and monitoring should be continued.
The comparison with the 2007-2008 nationwide survey (10) is significant in that, the 2007-2008 survey represents recent data at a relatively large scale despite the several limitations mentioned previously. As a baseline for future KNN studies, we described in detail the incidence and related characteristics of BPD in VLBW infants registered in the KNN database from January 2013 to June 2014, as well as recent changes in BPD compared with that in the previous study (10). Using the current data as baseline, the true trend of BPD in VLBW infants in Korea will be revealed.
In conclusion, the current incidence of BPD in Korea is increasing as the result of the increasing survival rate of extremely premature babies. Our KNN data and the precise comparison with other international neonatal network systems is the first step to establish an outstanding treatment modality for extremely preterm infants that will effectually decrease the mortality rate even further among BPD patients in the near future (1415161825).



 XML Download
XML Download