

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Neonatal care has advanced, improving the survival of very-lowbirth-weight (VLBW) infants. However, such patients remain at a high risk for sepsis (1). Up to 20% of mortalities in VLBW infants are caused by sepsis, and infants with sepsis are at a nearly-threefold risk of mortality than those without sepsis (23). Moreover, neonatal sepsis is a major cause of morbidity and poor neurodevelopmental outcomes among VLBW infants (4).
Early-onset sepsis (EOS) typically caused by organisms transmitted vertically before or at the time of birth, is present in approximately 2%-7% of infants. EOS has been associated with significantly increased odds for mortality, intraventricular hemorrhage (IVH), retinopathy of prematurity (ROP), and bronchopulmonary dysplasia (BPD) (567). Factors that were found to significantly increase the risk of EOS were low gestational age, low birth weight, low Apgar score, and maternal chorioamnionitis (7). Late-onset sepsis (LOS), occurring after 7 days of life, may be caused by pathogens acquired during delivery or during the course of hospital care (1). The risk factors of LOS include prematurity, a need for central venous access, and prolonged hospitalization (1). Patent ductus arteriosus (PDA), BPD, necrotizing enterocolitis (NEC) were significantly associated with increased rate of LOS (2).
Pathogens causing neonatal infections and their antibiotic susceptibility patterns may change over time and differ among countries. It is therefore important to monitor the epidemiology of neonatal infections to make decisions on policy and clinical practice (8). However, until the Korean Neonatal Network (KNN) was established, Korea did not have a national longitudinal neonatal infection surveillance system. Thus, only limited data on neonatal sepsis in Korea were reported (910).
This study was undertaken to determine the current incidences of EOS and LOS, the distribution of infecting pathogens, and the impact of infection on co-morbidities in VLBW infants cared for in the KNN.
MATERIALS AND METHODS
Study population
Data on EOS and LOS, infecting organisms, maternal and infant demographic data, and clinical data were analyzed using KNN registry. A total of 2,386 VLBW infants who were born from January 1, 2013 to June 31, 2014 in or transferred to one of the 55 KNN centers within 28 days of life were enrolled. Trained staff collected data on mothers and infants from birth to hospital discharge or death. External audits were done periodically to review the quality and reliability of data extracted from patient records in the KNN.
Outcomes
EOS was identified by clinical symptoms and a positive blood culture drawn in the first 7 days of life, and LOS was defined as infection occurring thereafter. Proven sepsis was defined as a positive result for one or more bacterial or fungal cultures obtained from blood of the infants with clinical signs of infection or treated with appropriate antibiotics for 5 or more days or until death without sign of infection (11). Series of samples that were repeatedly positive for the same organism within 7 days were considered as part of the same episode. If a different organism was noted in a subsequent culture, this was considered another episode. KNN registry included up to three episode of bacteria sepsis and up to two episodes of fungal sepsis.
Gestational age was determined by obstetric estimates. We defined antifungal prophylaxis as when the systemic antifungal agents for the prevention of fungal infections were administered shortly after birth. Congenital infection was confirmed via TORCH evaluation. Meningitis was defined as a positive spinal culture for infants treated with more than 5 days of antibiotic medication. IVH was graded according to the method of Papile et al (12). NEC was classified according to the system of Bell et al. (13). BPD was defined by NIH classification (14). The main cause of death was collected for all infants who died, according to the doctor's documentation.
Statistical analysis
For analyzing the rates of sepsis/1,000 hospital days and incidences of sepsis, gestational age was categorized as 4 groups; 24 weeks' gestation or less, 25-28 weeks' gestation, 29-32 weeks' gestation, and 33 weeks' gestation, and birth weight was categorized as 5 groups; less than 500 g, 500-749 g, 750-999 g, 1,000-1,249 g and 1,250-1,499 g. Infection rates were expressed as the rates of sepsis, EOS and LOS per 1,000 hospital days and percentage of all live births in each categories. Univariate analyses for continuous variables were performed using Student's t-test. Categorical variables, including the primary outcome, were examined using a chi-square analysis. Data are presented as mean and standard deviation, as the data were found to be normally distributed. Multivariate analyses were used to identify the independent association of EOS or LOS with neonatal outcome variables. Multivariate analysis adjusted for the significant factors through univariate analysis was done. Kaplan-Meier plotting was used to estimate the occurrence of the first LOS episode from lifetime data. Log-rank test was done for compare the probability among the categorized group divided by the birth weight (less than 500 g, 500-999 g, and 1,000-1,499 g) and gestational age (24 weeks' gestation or less, 25-28 weeks' gestation, and 29 weeks' gestation or more). Comparison of 1, 2, and 3 quartile estimated time for occurring first episode of LOS among the birth weight groups and gestational age groups using F-test was done. Calculations were performed with SPSS software version 21.0 (IBM Corp., Chicago, IL, USA) and SAS version 9.2 (SAS Institute, Cary, NC, USA). P values less than 0.05 were considered sta-tistically significant.
RESULTS
Incidence of EOS and LOS and demographic characteristics
Sepsis was found in 21.1% of 2,386 VLBW infants. The risk of sepsis was inversely related to birth weight and gestational age (Table 1). The rates of all sepsis episodes per 1,000 hospital days were also comparable for birth-weight and gestational-age categories. The rate of sepsis decreased with increasing birth weight to 7.35 for infants 500 to 749 g, 4.66 for infants 750 to 999 g, 4.14 for those 1,000 to 1,249 g, and 2.58 for those 1,250 to 1,499 g. Similarly, the infection rate was inversely related to gestational age. This rate of infection declined to 7.92 at ≤24 weeks, 5.63 at 25 to 28 weeks, 3.62 at 29 to 32 weeks, and only 1.65 for infants born at 33 weeks or more (Table 1). Among 2,386 VLBW infants enrolled in KNN, 85 infants had positive blood cultures in the first 7 days; thus, the incidence of EOS was 36 per 1,000 live births (Table 2). Among the 2,281 VLBW infants who survived until 7 days of age, 442 infants showed positive blood cultures after 7 days of age, and 632 microorganisms were noted due to multiple sepsis episodes. The overall incidence of LOS was 194 per 1,000 live births (Table 3). Only 23 infants (1%) had both EOS and LOS. The majority of infants (72%) had a single episode of LOS; 21% had two episodes, 5% had three episodes, and 1% had four or more episodes. The majority of episodes (60%) occurred in extremely low birth weight infants (96% were born at ≤32 weeks gestation). Infants with lower birth weights were more likely to have multiple episodes (<500 g, 29%; 500-749 g, 39%; 750-999 g, 20%; 1,000-1,249 g, 9%; 1,250-1,499 g, 3%; P<0.001).
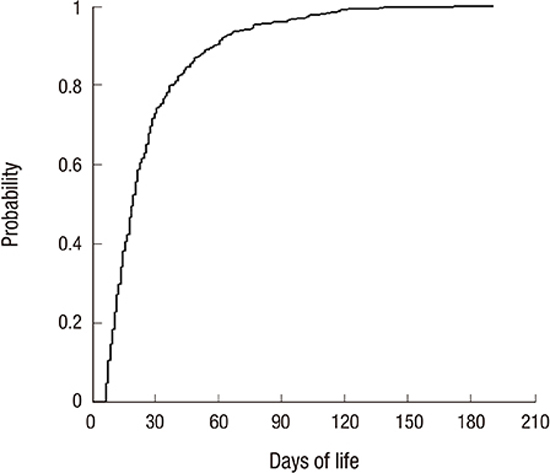
The first LOS episode based on lifetime data was estimated to occur at a median age of 20 days (range 7-198 days; 25th percentile: 12 days; 75th percentile: 33 days; Fig. 1). Using a log-rank test, we calculated the expected number of LOS episodes as time progressed in each group by dividing by the gestational age and birth weight. When the VLBW infants were divided into three groups according to birth weight (<500 g, 500-999 g, and ≥1,000 g), there were significant differences in the occurrence of the first LOS sepsis episode (P<0.001). The infants were also divided into three gestational age groups: ≤24 weeks, 25-28 weeks, and ≥29 weeks. Significant differences among the groups versus gestational age were found (P<0.001) (Fig. 2). Comparison of quartile estimated time among three groups according to the birth weight, showed no significance difference, using F-test. Comparison of 25 percent of LOS episode estimated time among three groups according to the gestational age, showed significant difference (P=0.012) (Table 4).
Distribution of pathogens causing EOS, LOS and direct mortality
The majority of EOS events were caused by Gram-positive organisms (56.5%). Coagulase-negative staphylococcus (CONS) was the most common pathogen, accounting for 30.6% of all infections. Gram-negative pathogens accounted for 40.0% of infections, with most common E. coli occurring in 11.8% of patients. Fungal pathogens were relatively rare compared to bacteria (3.5%).
The majority (72.0%) of LOS episodes were caused by Gram-positive organisms. CONS was the most common late-onset pathogen (38.3%) of all infections, comprising 53.2% of Gram-positive infections. Gram-negative pathogens accounted for 15.3% of all microorganisms. Klebsiella and Enterobacter species were the most common Gram-negative pathogens. Fungal organisms were responsible for 12.0% of LOS episodes (Table 5).
Overall, 100 of the 504 infants with sepsis died (19.8%). The main cause of death was confirmed as infection for 13 of 85 VLBW infants with EOS (15.3%). Death rates of EOS differed significantly by pathogen type; interestingly, 38.2% of Gram-negative organisms noted mortality, while all infants with Gram-positive organisms and fungal infections remained alive. The overall mortality rate for infants with EOS, regardless of cause of death, was 34.1% compared to 11.1% for infants with negative cultures (P<0.001; Table 7).
Overall, 16.0% of the infants with LOS died. The mortality rate of LOS for each pathogen indicated that infection was the most common cause of death, including infection due to Gram-negative organisms (9.3%), followed by Candida (6.6%), and Gram-positive organisms (2.4%). The mortality rate of CONS sepsis was only 1.2% (Table 5).
Twelve percent of infants died on the same day as when the blood culture was taken; 35% died within 3 days, and 40% died within 7 days. Infants infected with Gram-negative organisms were more likely to die acutely within 3 days of the positive blood culture (58%).
Patient characteristics and co-morbidities associated with EOS and LOS
The mean gestation, mean birth weight, and mean Apgar score were significantly lower in the EOS group than in the control group. Vaginal delivery and initial resuscitation were more common in the EOS group than in the control group (Table 6). Multivariate analyses for the major morbidities and mortality with EOS were adjusted for the gestation and initial resuscitation. After adjusted the gestation and initial resuscitation, VLBW with EOS were at an increased risk of IVH (≥G3) (OR 2.10 ,95% CI 1.27-3.48) and BPD (≥mod) (OR 1.96, 95%CI 1.16-3.30) (Table 7). In the LOS group, the mean gestation, birth weight, and Apgar score were significantly lower. Antenatal steroid use, and initial resuscitation were found to be significantly more common in the LOS group (Table 6). After adjusted the gestation, antenatal steroid use, and initial resuscitation to determine major morbidities and mortality of infants with LOS, VLBW with LOS were at an increased risk of IVH (≥G3) (OR 1.97, 95% CI 1.51-2.57), PVL (OR 2.06, 95% CI 1.50-2.83), BPD (≥mod) (OR 2.55, 95% CI 2.01-3.24), and NEC (≥G2) (OR 2.37, 95% CI 1.67-3.37) (Table 7).
DISCUSSION
This was the first large-scale study of neonatal sepsis in VLBW infants from 55 neonatal intensive care units (NICUs) in South Korea. The KNN was established in April 2013 as an infrastructure for NICU quality improvement, with the goal of improving the survival rate and decreasing the number of sepsis episodes. Before the KNN was established, there were only limited reports about neonatal sepsis in Korea, due to the small number of enrolled NICUs and the short duration of studies and retrospective studies (910).
There have been several nationwide epidemiological studies of infections among NICUs in other countries such as the Neonatal Research Network of the National Institute of Child Health and Human Development (NICHD) in the USA and the neonatal networks in Canada, Australia, New Zealand, and Japan (14151617). There has been considerable variability in the reported incidence of sepsis (2). VLBW infants born in the Neonatal Research Network (NRN) Centers of Japan in 2012 demonstrated an overall 8% incidence rate of sepsis (18). Among 5447 VLBW infants born at NICHD centers in the USA between 1998 and 2000, sepsis was present in 22% of all patients (3). Infants at less than 32 weeks of gestation in Level III NICUs of the Australian and New Zealand neonatal network (ANZNN) in 2012 showed a 12% rate of sepsis (17). In this study, during the 18 months of collection from January 2013, the overall incidence of sepsis was 21% of infants. The incidence of sepsis in the KNN was higher than that of the Japanese NRN and similar to those of the NICHD and other networks.
Early onset sepsis is variably defined as either occurring within 7 days after birth or within 48-72 hr of birth. EOS, defined as occurring within 7 days in Japan, was 3.6% (18). In the NICHD study, EOS was defined as occurring within 72 hr of birth and was noted in 1.5% of infants (3). From the data of ANZNN, EOS was defined as occurring within 48 hr of birth and was reported for 0.9% of infants (17). Sepsis was diagnosed more frequently at the low gestational age. The rate of EOS was 6% at 22 weeks and 1% at 28 weeks (19). In our study, EOS occurred in 3.6% of infants, with rates of 10.3% and more than 28 weeks.
The incidence of LOS showed variable range according to country and hospital. From the NICHD study, LOS was present in 22% of infants, and the rates of LOS were 58% at 22 weeks and 20% at 28 weeks (20). In our study, the incidence of LOS was shown to be 19.4% among the 2,281 infants who survived for more than 7 days after birth. In a report from the Netherlands, the incidence of LOS in VLBW infants was 14.9 per 1,000 patient days. In the German study, in their first year of reporting LOS incidence in VLBW infants, the rate was 8.3 per 1,000 patient days, and the overall incidence of sepsis was 4.7 per 1,000 patient days (21). In the NICHD study, the rate of the first episode of LOS was 3.8 per 1,000 patient days (11). In this study, the rate of LOS episodes was 3.1 per 1,000 patient days. The infection rate was inversely related to birth weight and gestation. Infants below 500 g found to have a short duration of hospitalization due to high mortality; thus, rates per hospital day for infants below 500 g were lower than those for infants between 500 and 749 g.
The patterns of pathogens responsible for neonatal sepsis have changed with time and vary from place to place (22). In the United Kingdom, organisms causing EOS are predominated by group B streptococcus. However, in the NICHD, a marked reduction in group B streptococcal sepsis (from 5.9 to 1.0 per 1,000; P<0.001) and an increase in Escherichia coli sepsis (from 3.2 to 6.8 per 1,000; P=0.004) were noted (23). Infants with EOS were more likely to die than uninfected infants (37% vs. 13%; P<0.001), especially if they were infected with Gram-negative organisms (11). In a recent study from Canada, however, CONS was found to be the most common organism identified in EOS among both full-term and preterm infants. However, mortality rate due to CONS was low in infants with EOS (6). In our study, Gram-positive organisms were the most predominant organisms of EOS in Korea. Coagulase-negative Staphylococcus was noted as the highest at 31%, followed by Staphylococcus aureus.
Microorganism populations isolated in infants with LOS were dominated by Gram-positive cocci, predominantly CONS (62.5%) (142425). In the NICHD study, CONS was the most common LOS pathogen (48% of all infections). Infections caused by yeast-like fungi constituted 7.9% of all the cases (1421). Gram-negative pathogens (35%) and fungi (35%) were the pathogens most associated with mortality in LOS, followed by CONS (18%). In our study, CONS (38%) was the most common pathogen of LOS, and Staphylococcus aureus appeared in 11% of cases. The mortality rate of CONS sepsis was only 1.2%, and that of Staphylococcus aureus sepsis was 5.6%. The mortality rate of Gram-negative sepsis was 9.3%, and that of fungal sepsis was 6.6%. According to a previous report, methicillin-resistant Staphylococcus aureus (MRSA) accounts for 80% of isolated Staphylococcus aureus cases in intensive care units and has become a threat to critically ill populations in Korea, including neonates. Kim et al. reported that LOS due to MRSA in Korea comprised 18.8% of cases (26). In this study, it has limitation about no information of LOS due to MRSA.
Neonatal sepsis is associated with increased mortality and morbidity among premature infants. From the data collected by the Israel Neonatal Network, EOS was associated with significantly increased odds of severe IVH (OR: 2.24), severe ROP (OR: 2.04), and BPD (OR: 1.74). EOS was also associated with an increased risk of death and/or severe neurologic morbidity (OR: 2.92) (5). The percentage of infants with EOS was higher among those with PROM >48 hr than among those with PROM<48 hr (P<0.001) (25). In our study, mean gestation, birth weight, mean APGAR score, cesarean section and initial resuscitation were significantly different between the EOS group and the control group. In analyzing the risk factor of EOS, gestational age was strongly associated with the risk of EOS (OR: 0.72). In accord with other studies, VLBW with EOS were at an increased risk of IVH (≥G3) (OR 2.10) and BPD (≥mod) (OR 1.96). However, there was no significant association with increased risk of death.
From the data collected by the Polish Neonatology Surveillance Network, the occurrence of LOS was significantly associated with increased length of mechanical ventilation (OR: 2.65) and continuous positive airway pressure (OR: 2.51), as well as the duration of antibiotic use (OR: 2.98) (27). Surgical procedures and lower gestational age were significantly associated with the risk of LOS (21). Infants who developed LOS were significantly more likely to develop BPD. In the NICHD study, infants with PDA (OR: 1.2), BPD (OR: 1.3), and NEC (OR: 2.7) had a higher incidence of LOS. There was no association between LOS and RDS, severe IVH, or PVL. In our study, VLBW infants with LOS were at an increased risk of IVH (≥G3) (OR 1.97), PVL (OR 2.06), BPD (≥mod) (OR 2.55), and NEC (≥G2) (OR 2.37). It is quite similar to other studies.
A large multicenter study from the German Neonatal Network showed that SGA was a risk factor of LOS (OR: 1.31; 95% CI: 1.02-1.68; P=0.03) (11). In contrast, a Norwegian population-based study on ELBW infants found no association between SGA and sepsis (28). In our study, SGA showed no significant risk of sepsis.
The majority of extreme low birth weight (ELBW) survivors in our study (65%) had at least one infection during their NICU birth stay. The occurrence of more than one infection was observed frequently among those with ELBW and LOS. However, no significant difference was noted in the occurrence of the timing of the first LOS episode among the birth weight groups and gestation groups.
Our study had several limitations. Differences of policy and treatment between the NICUs still remained. No more than five episodes of infection were collected, although these included most of the episodes of sepsis. Data regarding antenatal antibiotics use and antibiotics sensitivity were not collected.
This study provides a recent nationwide epidemiology of sepsis in VLBW infants in Korea. Based on this study, successful strategies to reduce infections among VLBW infants would improve survival and reduce neonatal morbidity. International comparisons and efforts for quality improvement will be needed.








 XML Download
XML Download