

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Intraventricular hemorrhage (IVH) is a cause of neonatal morbidity and mortality and is strongly associated with adverse neurological outcomes (12). The incidence of severe IVH (grade 3 or 4) has persisted despite the overall decline in IVH because the survival rate of very-low-birth-weight (VLBW) infants has consistently increased (34). According to multicenter studies, the incidence of IVH varies inversely with gestational age with an overall incidence of 15%-42%, while severe IVH develops in 7%-16% of VLBW infants (56789). Approximately 35% of VLBW infants with IVH develop post-hemorrhagic hydrocephalus (PHH), and 15% of VLBW infants with IVH require intervention (25810). In Korea, however, no nationwide data for the incidences of IVH and PHH have been reported to date. IVH is graded based on the Papile classification system (11), but the grading of PHH is not yet standardized. Although some studies have suggested using the criteria for ventricular dilatation (1213), there is currently no commonly accepted grading system. The decision to treat PHH has typically been made in clinical situations of increasing ventricular width from serial brain imaging. To date, only a few studies have addressed the risk factors for or outcomes of PHH in VLBW infants with IVH (141516). Identifying the associated risk factors for PHH would assist the decision-making process for serial brain imaging or procedures to remove cerebral spinal fluid (CSF) from VLBW infants who develop PHH after IVH.
The objective of the present study was to report the distribution of IVH and the associated risk factors for PHH among VLBW infants in Korea. For this objective, we first investigated the incidence of IVH in VLBW infants as well as the IVH induced mortality rate according to gestational age at birth and birth weight. Second, we evaluated the incidence of clinically significant PHH after IVH and the associated risk factors for procedures used to remove CSF in VLBW infants. Finally, we compared the Korean nationwide data to those in other national databases. The present study is to describe nationwide data of the incidence and mortality of IVH and PHH among VLBW infants in Korea.
MATERIALS AND METHODS
Study population
We performed a cohort study using prospectively collected data from 55 Korean Neonatal Network (KNN) centers. A total of 2,386 VLBW infants born between January 2013 and June 2014 and registered in the KNN were reviewed. We excluded 63 VLBW infants who did not have documented brain ultrasonography (BUS) results, and among them, 60 infants were expired within 7 days after birth. Finally, the remaining 2,323 were included in the present study. The infants were grouped according to the most severe IVH grade reported on BUS documents during neonatal intensive care unit hospitalization.
Data collection and analysis
Informed consent was obtained to access the KNN database. Neonatology staff members or trained research coordinators prospectively gathered maternal, delivery, and neonatal data until the first patient discharge according to the KNN manual of operational procedure (17). For infants with persistent hospitalization, limited data were collected to postnatal day 365. Gestational age was determined by the best obstetric estimate using the date of the last menstrual period and/or ultrasonography. Antenatal corticosteroid exposure was defined as the maternal receipt of one or more doses of any corticosteroid. Pulmonary hemorrhage was defined as massive and significant pulmonary hemorrhage that destabilized vital signs. Hypotension referred to the hypotension that developed within the first week of life that required medication including cardiotonics or steroids. Infants who received medication or surgery to treat patent ductus arteriosus (PDA) for therapeutic and/or prophylactic purposes were identified as PDA medication or PDA ligation. The most severe stage of IVH of all BUS findings until first discharge was recorded irrespective of the time of first observation or occurrence as this information was not collected. IVH staging was made according to Papile's classification (11). PHH was defined as IVH-induced hydrocephalus that required spinal tapping, external ventricular drainage, and/or a shunt operation. Mortality that occurred before the first discharge was termed in-hospital death, while mortality that was primarily related to IVH was defined as death of which primary cause was severe grade IVH and its sequelae in the KNN dataset. Bronchopulmonary dysplasia (BPD) was defined by the use of the National Institutes of Health Workshop severity-based diagnostic criteria (18). We analyzed the gestational age- and birth weight-dependent incidence of IVH and compared the IVH incidences of the KNN to other national registry datasets including the Canadian Neonatal Network (CNN) (19), Australian and New Zealand Neonatal Network (ANZNN) (20), European Neonatal Network (EuroNeoNet) (21), and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) (4). IVH grade-dependent incidences of PHH in surviving infants and mortality with time of death were assessed. Among surviving infants with IVH grades 3-4, we grouped them according to PHH occurrence (PHH and non-PHH groups) and compared the maternal demographics and neonatal characteristics between groups.
Statistical analysis
Unadjusted comparisons of maternal demographics and neonatal characteristics between the non-PHH and PHH groups among IVH grade 3-4 infants were performed using the chi-square or Fisher exact test for categorical data and Student's t-test for continuous variables. A binary logistic regression was performed for the adjusted analysis. P values<0.05 were considered statistically significant. SPSS version 18 (IBM Corp., Chicago, IL, USA) was used for all of the statistical analyses.
RESULTS
Incidence of IVH
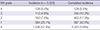
A total of 2,386 VLBW infants were enrolled in the KNN registry during the study period. Of these infants, 2,323 with documented BUS were included in the analysis. The overall incidence of IVH in the VLBW infants registered in the KNN was 42.5% (987 of 2,323) (Table 1). Severe (grade 3-4) IVH occurred in 10.3% (240 of 2,323) of VLBW infants (Table 1). Among infants with any grade IVH, the incidence of grade 1, 2, 3, and 4 disease was 59.2% (584), 16.5% (163), 11.3% (112), and 13.0% (128), respectively. Fig. 1 shows the gestational age- and birth weight-dependent incidence of IVH by grade. Overall and severe (grade 3-4) IVH were more common in smaller and more immature infants (Table 2).
Incidence of PHH
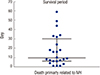
IVH grade-dependent incidence of PHH is described in Table 3. In the IVH grade 3-4 infants who expired in the early period (the median survival time of IVH grade 3-4 infants was postnatal day 12; Fig. 2), there is a limitation to assessing accurate occurrence of PHH because it usually requires therapeutic intervention in the later period. Thus, incidences of PHH or death in all registered infants or PHH in only survived infants were displayed. PHH did not develop in survived infants with IVH grade 1, and it occurred only in 3.5% of survived infants with grade 2 IVH. However, the incidence significantly increased in infants with grades 3-4 IVH. Moreover, incidence of PHH or death also showed IVH grade dependent pattern and it occurs in the 52.7% and 86.7% of all infants with grade 3 and grade 4 IVH, respectively (Table 3).
Mortality primarily related to IVH
Total and primarily IVH-related mortality rates are displayed in Table 3. None of the infants with grade 1-2 IVH expired because of IVH. However, 3.6% and 15.6% of infants with grade 3-4 IVH expired, respectively, due primarily to IVH (Table 3). As per the KNN dataset, of the 110 infants who had died, 24 (22%) had a primary cause of death as severe IVH and its sequelae. The median time of death in infants who expired primarily because of IVH was on the 10th postnatal day and ranged from the 3rd to the 124th postnatal day (25-75 percentile, 6th-32nd postnatal day) (Fig. 2).
Factors related to PHH development
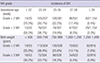
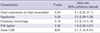
To assess the factors associated with PHH development in the surviving infants with grade 3-4 IVH, the maternal demographic findings and neonatal characteristics were compared between the PHH and non-PHH groups (Table 4). Factors found to be significantly higher in the PHH group than in the non-PHH group included the chest compressions at initial resuscitation, significant pulmonary hemorrhage destabilized vital signs, significant hypotension requiring medication within the 1st week of life, PDA ligation, and IVH grade 4. After logistic regression adjustment for above factors, only the incidence of IVH grade 4 was significantly higher in the PHH group than in the non-PHH group with an adjusted odds ratio (OR) of 3.1 and a 95% confidence interval (CI) of 1.35-6.91 (Table 5). Although the use or non-use of chest compressions at initial resuscitation did not reach statistical significance (P=0.05), it showed a high adjusted OR of 5.1 (95% CI, 0.97-27.1).
National comparisons of IVH incidence
The incidences of IVH grades 2-4 in the KNN (January 2013-June 2014) were compared with those in the ANZNN (2012), CNN (2013), and NICHD (2003-2007), and the incidence of IVH grades 3-4 in KNN was compared with that in EURONET (2011) based on the annual report of each registry or published papers (Fig. 3). In VLBW infants born at ≤24 gestational weeks, KNN appears the trend of having a higher incidence of IVH grades 2-4 or 3-4 than the ANZNN, CNN, NICHD, and EuroNeoNet networks. Among infants born at 25-28 gestational weeks, the incidence of IVH grade 2-4 or 3-4 in the KNN seemed similar to those in the other networks.
DISCUSSION
This study reported the Korean nationwide incidences of IVH and PHH requiring a procedure to remove CSF after IVH. This population-based study suggests that IVH is a common problem in VLBW infants in Korea, with 42.5% of VLBW infants developing IVH of any grade and 10.3% developing IVH grade 3 or 4. The more immature infants were at greater risk of severe IVH and subsequent PHH. The finding in the present study is consistent with previous reports derived from CNN (19), NICHD (4), and EuroNeoNet (21) data (Fig. 3). A comparison of the KNN and other national registry datasets revealed that the incidence of IVH in infants who were ≤24 gestational weeks at birth in the KNN seemed to be higher than those in the other national registries, while ANZNN appeared to show a trend of a lower incidence of IVH compared to other registries. One possible explanation might be that the KNN registry contains population-based data whereas the ANZNN registry includes data from only tertiary centers.
In the present study, infants born at ≤22 gestational weeks had a strikingly high incidence of IVH (70%), while those with a birth weight ≤500 g had a similar incidence of IVH as those with a birth weight of 500-999 g. In the development of IVH, gestational age seems to be a more significant factor than birth weight, although both gestational age and birth weight influence IVH development. Consistent with previous studies, the present study also demonstrated that IVH incidence and severity in VLBW infants decreases gradually as gestational age or birth weight increases (1622) and that infants born after 29 gestational weeks or weighing>1,250 g at birth are at a low risk of IVH.
PHH is a major consequence of IVH (23). PHH is thought to cause white matter injury by multiple mechanisms, such as disturbing periventricular fibers, increasing intracranial pressure, introducing iron-induced hydroxyl free radicals, and eliciting cytokine responses (232425). Although the precise mechanism has not been completely delineated, the pathogenesis of IVH-induced PHH has been explained to be related with multiple small blood clots partially occlude the channels of CSF circulation or blood induced inflammation within subarachnoid spaces and ensuing obliterative arachnoditis which reduces CSF resorption (26272829). Previous studies suggested that PHH induces ischemia, oligodendrocyte and axonal injury in the white matter, and eventually motor or cognitive dysfunction (153031). In the present study, 8.5% of survived infants with IVH of any grade showed progression of PHH and underwent spinal tapping, external ventricular drainage, and/or a shunt operation to remove the CSF. In the infants with severe IVH (grade 3-4), PHH or death developed in the 52.7% and 86.7% of infants with IVH grade 3 and 4, respectively. The incidence of PHH requiring a procedural intervention among survived VLBW infants with grade 3 or 4 IVH was similar to those of previous studies (214). One previous study suggested that the incidences of PHH and shunt operations have been increasing over time (15), a finding that might be related to an increased survival rate of VLBW infants with severe IVH and, thereby, an increased risk of PHH.
The optimal treatment strategy for PHH is not yet known, and the clinical management for PHH varies considerably among centers (28). There have been only a few arguments for early intervention to remove the CSF prior to the development of clinically significant PHH (323334353637). We noted inconsistency in the interpretations among radiologists as well as variability in the PHH procedure rates among medical centers, indicating the need to establish a standardized guideline for the diagnosis and treatment of PHH (16). To date, only a few studies have reported the risk factors of PHH development after IVH (1415). Most suggested that IVH severity would be the most important predictive factor for a shunt operation. Consistent with above findings, the present study also showed that about 3 fold higher development of PHH in infants with IVH grade 3 than infants with IVH grade 4. We also investigated the presence of other clinical factors affecting PHH development in VLBW infants with IVH grade 3 or 4. On univariate analysis, variables related with circulation, such as chest compressions at initial resuscitation, pulmonary hemorrhage, hypotension, and PDA operation differed significantly between the PHH and non-PHH groups. Although all factors except IVH grade 4 were no longer significant after adjustment, it is interesting that chest compressions at initial resuscitation occurred more frequently in the PHH group (P=0.05) and showed a high OR of 5.1 even after adjustment.
Mortality is a major consequence of severe IVH or PHH. Recent studies have reported that the mortality rate is approximately 30% in infants with IVH grade 3 and 60% in infants with IVH grade 4 (1538), and the results of the present study support these findings. Furthermore, we analyzed the mortality rate primarily related to IVH and found that it was 3.6% in infants with grade 3 IVH and 15.6% in infants with grade 4 IVH. Because the KNN registry collected data about the primary cause of death, the present study could show the mortality rate that was primarily related to IVH. However, a possible limitation of the study could be that the combined diseases such as disseminated intravascular coagulopathy, BPD, PDA, and other mortality-associated variables could not be considered. The present study showed that the median time of death caused primarily by IVH was the 10th postnatal day, indicating that infants with severe IVH are in a generally deteriorated state. Another issue requiring consideration is that the withdrawal of life-sustaining treatment is often discussed with the parents of infants with severe IVH, although it is not clear whether this affected the survival time recorded in the KNN registry.
A major limitation of the present study is that the KNN registry has various criteria for the diagnosis of PHH as well as different guidelines for its treatment. However, this is a global problem that needs to be addressed. Because of the absence of a definite criteria, the KNN registry collected data for only PHH cases in which procedures to remove CSF were needed; therefore, we could not determine the overall incidence of PHH including non-treated cases.
In this context, early expired VLBW infants with severe IVH were excluded from the analysis for associated factors with PHH development. In addition, infants with IVH grade 2 were also excluded from this analysis because of the potential bias stems from infrequency of PHH development in survived infants with IVH grade 2.
In conclusion, the present study shows that IVH is a common problem in VLBW infants and that infants with severe IVH tend to develop PHH that requires procedures to remove the CSF. The present study is the first to report the incidence and mortality rates of IVH and PHH based on a Korean nationwide dataset. A subsequent study of the long-term neurodevelopmental outcomes of the infants in our study should be conducted.




 XML Download
XML Download