

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In 2010, approximately 15 million babies were born preterm, 11.1% of all live births, in the world, with about one million premature babies dying after birth. Preterm birth is the main cause of infant death, with reliable trend data showing an increase in preterm birth rates in most countries (1). Because preterm births contribute to infant mortality rates, many countries have reported the incidence and mortality rate of preterm birth in population-based, multicenter studies (234). An analysis of the factors associated with the mortality of preterm babies is a necessary medical service and will assist treatment developments to improve outcomes for preterm babies. There have been many studies on the risk factors for mortality in preterm babies in the neonatal intensive care unit (NICU) with the aim of improving preterm survival (56789).
Over the past several decades, advances in perinatal and neonatal care have improved the survival of even the most immature infants, increasing and diversifying our knowledge of the causes of death in preterm babies (1011). However, many studies have only focused on the mortality or risk factors for mortality of preterm babies. Research on the categorical causes of death is extremely rare, especially for the risk factors for each categorical cause of death (12).
We aimed to investigate the categorical cause and timing of death with respect to postnatal age and gestational age (GA) and assess the risk factors that affect cause-specific mortality of very-low-birth-weight (VLBW) infants registered in the Korean Neonatal Network (KNN) using a case-control study.
MATERIALS AND METHODS
Subjects
In this cohort study, we reviewed VLBW infants (birth weights, BWs <1,500 g) born alive and admitted to 55 NICUs of KNN participating hospitals between January 2013 to June 2014 (n= 2,386). These births were registered in the KNN database. A standardized data form was used to collect medical information on ORIGINAL ARTICLE Pediatrics pregnancy complications and care, conditions and assistance at birth, morbidities and treatments in the NICU, outcome at discharge from hospital, and time and cause of death.
For the purposes of this study, 4 infants less than 22 completed weeks of GA, 337 infants more than 31 completed weeks of GA, 82 infants with lethal congenital anomalies, 2 infants with accidental death or an inborn error of metabolism, 192 infants with unknown maternal factors, 2 infants with stays of more than 365 days in the hospital, and 118 infants transferred to other hospitals or other wards were excluded (Fig. 1).
Maternal and neonatal variables
Maternal variables were parity, maternal age, abnormal amniotic fluid volume, maternal nationality, hypertension, chorioamnionitis, preterm premature rupture of membranes (PPROM), use of antenatal steroids, mode of delivery, multiple gestation, and place of birth.
Neonatal variables were the gender of the infant, mean GA, mean BW, small for gestational age (SGA; <10th percentile of a standard BW curve for GA by gender), Apgar score ≤3 at 1 min, Apgar score ≤3 at 5 min, neonatal cardiopulmonary resuscitation in the delivery room.
Maternal hypertension was defined if there is any maternal diagnosis of pregnancy induced hypertension or chronic hypertension. SGA was defined according to the definitions published by Lim et al. and alexander et al. (1314). Delivery room (DR) resuscitation was defined when cardiac compression was done or medication was administered in the DR.
Neonatal morbidities and interventions were pneumothorax, massive pulmonary hemorrhage, pulmonary hypertension, respiratory distress syndrome (RDS), multiple use of surfactant, duration of ventilator care, treatment of bronchopulmonary dysplasia (BPD), pharmacological or surgical treatment for patent ductus arteriosus (PDA), hypotension, neonatal seizure, intraventricular hemorrhage (IVH; grade 3 or 4 in the classification by Papile), posthemorrhagic hydrocephalus, periventricular leukomalacia (PVL), congenital infection, sepsis, meningitis, necrotizing enterocolitis (NEC, ≥stage 2), packed red blood cell transfusion, and average length of hospital day.
BPD was defined by supplemental oxygen dependence at 36 weeks' PMA (15). Moderate BPD was defined as the need for oxygen for >28 days plus <30% oxygen at 36 weeks PMA using the National Institute of Child Health and Human Development (NICHD) Workshop severity-based diagnostic criteria. Severe BPD was defined as the need for oxygen for >28 days plus ≥30% oxygen and/or positive pressure at 36 weeks PMA by NICHD criteria (16). NEC is defined according to a modified Bell' staging classification stage ≥2 including one or more of the following clinical signs: bilious, gastric aspirate or emesis, abdominal distention, or occult or gross blood in stool. In addition, this classification includes one or more of the following radiographic findings: pneumatosis intestinalis, hepatobiliary gas, or pneumoperitoneum.
Statistical analysis
Analyses were performed using Stata version 12.0 (StataCorp, College Station, Texas).
Study I
We compared maternal and neonatal variables of infants who died in NICU (n=236) with infants discharged alive (n=1,413) as a control. Groups were compared using the independent-samples Student t-test and Chi-squared tests, where appropriate. The Kaplan-Meier method was calculated to estimate survival curves of VLBW infants. Infants discharged alive were considered to have survived to postnatal age of 364 days. The effects of GA and BW on survival were studied by Kaplan-Meier survival estimators for each category using the log-rank test.
Study II
We studied the proportional mortality for major causes of death with respect to postnatal age and the cause of death with respect to GA. To reduce the differences in mean GA between infants dying in NICU (n=236) and infants discharged alive (n=1,413), controls and cases were frequency matched by GA categories (22-24, 25-26, 27-28, or 29-31 weeks). A total of 472 (236:236) VLBW infants were identified. Groups were compared using the independent-samples Student t-test and Chi-squared tests, where appropriate. Multivariable Cox proportional hazard models were used to examine the relationship between prenatal characteristics, infant characteristics, interventions in the delivery room, and cause-specific mortality. Independent variables for the models were selected from variables significantly related to death in a univariate analysis or those shown by previous follow-up studies to be associated with a poor outcome (17).
The cause of death was categorized according to Korean Standard Classification of Diseases, based on the International Classification of Diseases (10th revision, Clinical Modification). The following mutually exclusive categories were considered: cardiorespiratory, including hyaline membrane disease or RDS, pulmonary hypoplasia, pulmonary hemorrhage, air leak syndrome, BPD or chronic lung disease, and other cardiorespiratory disease; neurological, including hypoxic-ischemic encephalopathy or asphyxia, severe IVH and its sequelae, and other neurological diseases; infection, including congenital infection, acquired infection, and other infectious diseases; gastrointestinal, including NEC or spontaneous intestinal perforation, and other gastrointestinal diseases; and others, including trauma or accident, inborn errors of metabolism, multisystemic failures of unknown etiology, and other abnormalities. P<0.05 was considered statistically significant.
RESULTS
Study I
In 2013, 436,455 babies were born in Korea, of which 2,961 were VLBW infants. Of these VLBW infants, 1,398 were entered into the KNN database. In the first half of 2014, 988 VLBW infants were registered in the KNN for a total of 2,386 preterm babies. After application of the inclusion and exclusion criteria, the study cohort comprised of 1,649 infants. Of which 1,413 babies were discharged alive and 236 babies died in the NICU.
Clinical characteristics of death and survival groups at NICU discharge
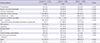
A comparison of the clinical characteristics of mothers in the survival and death groups is shown in Table 1. Mothers of VLBW infants in the death group were more likely to have abnormal amniotic fluid (oligo- or polyhydramnios) and foreign nationality than mothers in the survival group. Mothers of VLBW infants in the survival group were more likely to have PPROM, receive antenatal corticosteroids, and deliver by c-sec than mothers in the death group.
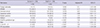
The neonatal characteristics and perinatal interventions in the survival and death groups are compared in Table 2. Compared to infants in the survival group, VLBW infants in the death group were more likely to have SGA (15.7% vs. 22.9%), lower GA (27.8±2.1 vs. 25.3±2.2 weeks), lower BW (1,064.4±265.9 vs. 761.7±248.5 g), and an Apgar score ≤3 at 1 and 5 min. Resuscitation efforts in the delivery room were more common among VLBW infants in the death group compared with the survival group. In the death group, 97.9% infants underwent PPV, 94.5% underwent intubation; 17.4% underwent cardiac compression; and 13.1% received endotracheal or intravenous epinephrine in the delivery room.
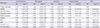
Table 3 shows the results of the comparison of neonatal morbidity and hospital course in the survival and death groups. VLBW infants in the death group were more likely to have a pneumothorax, massive pulmonary hemorrhage, pulmonary hypertension, RDS, multiple surfactant use, long duration under ventilator care, hypotension, neonatal seizures, IVH (grade ≥3), post-hemorrhagic hydrocephalus, PVL, sepsis, NEC (stage ≥2), and idiopathic bowel perforation than infants in the survival group. In contrast, VLBW infants in the death group had a lower frequency of BPD due to early death.
Survival and mortality
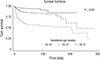
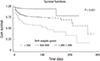
Survival curves from birth to 364 days after birth for the 1,649 liveborn VLBW infants by GA and BW are shown in Fig. 2 and 3. Survival to 100 days and 300 days rose with increasing GA and BW. For lower GAs and BWs, because deaths occurred early in the neonatal period, there are large differences in survival to 100 days and 300 days (P<0.001).
Fig. 4 shows the number of major causes of death at each postnatal age interval for VLBW infants in the death group. More than half of the deaths occurred in the first two weeks of life, mainly due to cardiorespiratory and neurologic problems. From 14 to 59 postnatal days, cardiorespiratory problems were a reduced but steady cause of death, while infectious and gastrointestinal problems became more prevalent. After 60 days, infectious and gastrointestinal problems became the predominant cause of death.
Fig. 5 shows the mortality rate, which is the number of deaths of infants per 100 live births, of causes of death according to GA in the study group. Cardiorespiratory problems were most commonly identified as the cause of death for all infants born between 22 and 31 weeks of gestation. Among infants born at 22-24 and 28-31 weeks of gestation, infections were the second leading major cause of death. For those born at 25-27 weeks of gestation, gastrointestinal problems were the second major cause of death. Among VLBW infants born at 22 to 31 weeks of GA, cardiorespiratory problems were the commonest cause of death (5.7%) followed by infections (2.5%), gastrointestinal problems (2.4%), neurologic problems (2.0%), others (1.7%). Survival increased as GA increased.
Study II
Factors associated with death
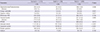
VLBW infants in the survival group were matched according to GA with a case group of infants from the death group. Relevant variables were compared between the cases (n=236) and controls (n=236) by Cox proportional hazards regressions. Simple comparison and adjusted hazard ratios (HRs) for these variables are shown in Table 4. Four risk factors were found to be significantly associated with increased risk for mortality: foreign nationality (HR, 2.50; 95% confidence interval, CI, 1.42-4.40), SGA (HR, 1.55; 95% CI, 1.11-2.16), Apgar score ≤3 at 5 min (HR, 1.62; 95% CI, 1.14-2.31), and DR resuscitation (HR, 1.80; 95% CI, 1.23-2.62). Concerned about neonates from multiple gestation, a trend toward statistical significance is sometimes noted with increased risk for mortality (HR, 1.31; 95% CI, 0.99-1.72). In contrast, PPROM (HR, 0.71; 95% CI, 0.54-0.94) and antenatal steroid (HR, 0.67; 95% CI, 0.50-0.91) were found to decrease mortality risk.
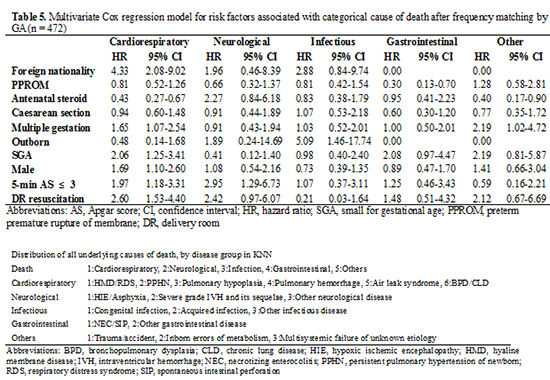
Multivariable Cox proportional HRs of the probable factors associated with cause-specific mortality of VLBW infants are presented in Tables 5 and 6. Infants of foreign mothers had a significantly higher risk of death due to cardiorespiratory problem than of death due to other major causes of death. Similarly, multiple gestation (HR, 1.65; 95% CI, 1.07-2.54), SGA (HR, 2.06; 95% CI, 1.25-3.41), male gender (HR, 1.69; 95% CI, 1.10-2.60), an Apgar score ≤3 at 5 min (HR, 1.97; 95% CI, 1.18-3.31), and DR resuscitation (HR, 2.60; 95% CI, 1.53-4.40) were significant risk factors for cardiorespiratory death. An Apgar score ≤3 at 5 min was also associated with neurological death (HR, 2.95; 95% CI, 1.29-6.73). Outborn status was associated with death due to infection in the NICU (HR, 5.09; 95% CI, 1.46-17.74). Maternal PPROM and the use of antenatal steroids appeared protective. VLBW infants born to mothers who received antenatal steroid and those born to mothers with a history of PPROM had a reduced risk of cardiorespiratory mortality (HR, 0.43; 95% CI, 0.27-0.67) and gastrointestinal mortality (HR, 0.30; 95% CI, 0.13-0.70), respectively.
DISCUSSION
This is the first case-controlled multicenter study to identify risk factors for cause-specific mortality of VLBW infants after frequency matching by GA. GA and BW have a significant impact on the mortality of VLBW infants (18). We attempted to reduce these effects by frequency matching of the two groups by GA to identify other risk factors. We excluded congenital anomalies, as there was a high mortality rate in the congenital anomaly group (30.5%) compared to a group without defects (16.7%), with the causes of death very different between the two groups.
Foreign mothers have an increased mortality risk, especially due to cardiorespiratory death. There were 49 (2.97%) foreign mothers, with most being Asian (17 Vietnamese, 14 Chinese, 7 Filipino, 2 Cambodian, 1 Japanese and 1 Mongolian), although there were 7 others (1 American and 6 others). The number of neonates in multi-cultural families in Korea is rising steadily due to the increase in international marriages (19). But, this result has limitation because there is a very small number of foreign mothers, and we do not know the socioeconomic status of foreign mothers. The Apgar score at 1 min reflects how well the baby tolerated the birth process, and the Apgar score at 5 min reflects how well baby is doing after birth (20). The Apgar score at 5 min, in particular, acts as a prognostic precursor for neonatal mortality and neurological outcome. This was also seen in our study, where there was an increase in mortality with an Apgar score ≤3 at 5 min (HR, 1.62), consistent with results of other studies that the Apgar score is a risk factor in NICU mortality (212223).
The longer the intensive resuscitation, the higher the mortality and poorer the neurological outcome (24). Until now, there have been no prospective analyses or placebo-controlled clinical trials on epinephrine (25). We found that DR resuscitation increased mortality due to cardiorespiratory problems (HR, 2.60). Cardiorespiratory problems occurred mainly within two weeks after birth, indicating that DR resuscitation may play a bigger role in early death due to asphyxia. We found that early resuscitation after birth was closely related to the prognosis and mortality of VLBW infants.
Initial temperature at NICU admission, initial pH, and BE were excluded during Cox analysis for the following reasons. After frequency matching there was no statistical significance between the two groups in the mortality rate in accordance with initial temperature. Also, although there was statistical significance in pH and BE at initial ABGA in 1 hr, there were more than 60 cases of missing data. Nevertheless, above factors are believed to act as important risk factors of death, and additional research including initial temperature will be necessary in the future when collection of data has increased.
In addition to foreign nationality, an Apgar score ≤3 at 5 min, and DR resuscitation, other factors that increased the risk of cardiorespiratory death were multiple gestation (HR, 1.65), SGA (HR, 2.06), and male gender (HR, 1.69). Pregnancy complications such as pregnancy-induced hypertension, gestational diabetes mellitus, PPROM, and preterm labor are associated with multiple births (2627). Qiu et al. (28) reported that it is not multiple gestation itself that is important, but the associated increased risk of preterm delivery, low BW, and other high-risk morbidities. Nielsen et al. (29) reported there was no significant difference in survival to NICU discharge between multiples (79%) and singletons (81%) at 24-26 weeks or multiples (98%) and singletons (96%) at 30-32 weeks. Multiple gestation could be a risk factor in cardiorespiratory-specific mortality or multi-systemic failure of unknown etiology after frequency matching (HR, 2.19).
Infants born with SGA had higher mortality compared to those with an appropriate for gestational age (AGA) and had increased mortality and, in the case of lower GA, more severe growth restriction. SGA infants had significantly higher incidences of BPD, pulmonary hemorrhage, and postnatal corticosteroid therapy compared to infants with AGA (3031). There was significant difference in the incidence of SGA between the survival and death groups (P=0.006) and the risk of death (HR 1.87) from cardiorespiratory causes was higher. Therefore, better planning of regular antenatal care is needed to reduce the precipitating factors of SGA, such as hypertensive disorders in pregnancy, gestational DM, infection, and malnutrition.
Male gender was not a risk factor in this study after frequency matching, but cardiorespiratory-specific mortality in males was higher compared to females (HR, 1.69; 95% CI, 1.10-2.60). Some studies showed that a higher incidence of RDS in male infants is due to late lung maturation (32), though the biological mechanisms are poorly understood. In this study, the incidence of RDS after matching was 95.47% in males and 93.89% in females, with no statistically significant differences. However, males had a higher mortality rate, lower Apgar scores, and poorer neonatal outcomes, as seen in other studies (733).
This study shows that both maternal PPROM and antenatal steroids lowered the mortality rate of VLBW infants. In the case of PPROM, there is an increased risk of premature birth, leading to higher neonatal mortality due to an increased incidence of early neonatal sepsis and pneumonia from intra-amniotic infection (34). However, the presence of an infection is more critical than PPROM, and infections are related to chorioamnionitis, duration of membrane rupture, and neurodevelopmental impairment (35). Several other studies have reported that, with PPROM, antibiotics and corticosteroids have a strong effect in reducing adverse neonatal outcomes such as RDS and IVH (36). This study also revealed that, with PPROM, the mortality rate of the control group decreased to a HR of 0.71. The rate of PPROM was significantly high in the survival group upon a simple comparison of all studied VLBW infants. There was no difference in chorioamnionitis between the two groups, suggesting that there is chorioamnionitis-independent protective effect with PPROM. Further research with larger numbers is required to verify the significant drop in gastrointestinal-specific mortality due to PPROM shown in this study.
Antenatal steroid injections for the pregnant women are widely known to lower the incidence of RDS and mortality rate of premature infants by inducing lung maturation. According to the 2006 Cochrane Database, antenatal steroid injections also lowered the incidence of IVH and NEC by influencing the circulatory stability of preterm infants (37). Analogous to preceding reports, this study also revealed a decrease in overall mortality after frequency matching (HR, 0.67), particularly in the risk of death from cardiorespiratory problem (HR, 0.43) among the various major causes of death.
A cesarean section (c-sec) delivery had a lower risk of death, but there were no statistically significant differences after frequency matching and a Cox regression analysis. Previous studies reported that c-sec lowered the risk of death, probably due to the full preparation required when performing a c-sec rather than the direct effect of the delivery method itself (38). There were only 30 deliveries (1.8%) outside the hospital in the study, but their risk of death (HR) from infection was 5.09 times higher. To lower the mortality rate of deliveries outside the hospital, aggressive handling is required for emergency transfer and infection management.
In this study, we found that the cause-specific risk of death in VLBW infants varied by postnatal age and GA. The predominant causes of mortality were cardiorespiratory and neurological problems in the first week, infections between the first week and first month, and gastrointestinal problems between the second week and second month of life. Cardiorespiratory problems were the most common cause of death in all infants born at 22-31 weeks. Infections were the second most common cause of death at 22-24 and 28-31 weeks and gastrointestinal problem were the second most common cause of death at 25-27 weeks of GA. These findings are consistent with other studies, which found that about half of all deaths of premature infants occurred within two weeks of age and respiratory morbidity is the most common cause of death in premature infants (12).
This study was limited by its small size, lack of comparison of inter-NICU outcome, and lack of evaluation of the long-term outcome of surviving infants after NICU discharge. However, this is the first study using KNN data to examine the risk factors for cause-specific mortality of VLBW infants. KNN has taken the first steps in gathering knowledge on the outcomes of preterm infants and the risk factors for mortality and morbidities in Korea. More data will be collected in the future.
We conclude that, according to a Cox proportional hazards regressions analysis, foreign mother, SGA, AS ≤3 at 5 min and DR resuscitation were associated with increase in mortality and PPROM and antenatal steroid were associated with decreased mortality. Based on categorical causes of death, foreign mother, multiple gestation, SGA, male gender, Apgar score ≤3 at 5 min, and resuscitation in the delivery room are associated with cardiorespiratory mortality of VLBW infants in NICU. An Apgar score ≤3 at 5 min and outborn status are associated with neurological and infection mortality, respectively.





 XML Download
XML Download