

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although the actors engaged in Official Development Assistance (ODA) have evolved in terms of diversity and the scale of financial resources entering ODA for health has increased tremendously, developing countries are still suffering from epidemics, barely showing improvement in health outcomes. This has brought about debate on aid effectiveness, which raised attention to governance failures in recipient countries as one of the causal factors for such ineffectiveness of ODA efforts. Now, the so called, "good governance" of developing countries became one of the goals as well as the conditions of aid. The effectiveness of governance on ODA for health has been proved in various empirical studies (12).
However, like all other factors, governance does not work independent of other factors. Some countries such as Moldova, Belarus, showed a significant improvement in health outcome even if their governance has been poor. This invited a need to review other background factors that may interplay with governance on health outcomes.
Similarly, since the "combat with HIV/AIDS" became one of the Millennium Development Goals (MDGs) in the year of 2000 and financial supports to fight against HIV/AIDS through ODA has increased dramatically, importance of contextual determinants of HIV/AIDS aid effectiveness has been drawing attentions from HIV/AIDS researchers (34). For example, Bor argued that an HIV/AIDS outcome is a result of interaction of governance factors such as regimes type, stability, and bureaucratic capacity with other contextual factors such as level of economic development, cultural factors and gender inequality (2).
However, most of the researchers only focused on independent effect of causal factors using quantitative method of analysis (1567) or case studies which have some limitations to be generalized because it is in-depth stories of specific cases (4589).
In fact, an econometric analysis and case studies have been dominant methodologies in social science even though a lot of researchers have recognized their limitations. Fuzzy-set Qualitative Comparative Analysis (Fs/QCA) appeared as an eclectic approach, playing a bridging role between the two methods and it is the only method in social science that can identify which combination of factors determines an outcome. In addition, Fs/QCA recognizes variations in explanatory variables differently according to whether those variations of explanatory variables affect the outcome variable or not while econometric analysis deals with all variations across all the ranges of explanatory variables equally (10).
Control of corruption and democratic accountability in effectiveness of HIV/AIDS aids
Corruption is known to have the negative effects on health outcome via various pathways. It raises the cost of health care services, deterring accessibility to health services (11). In addition, corruption decreases government revenue, lowering the quality of public healthcare service, which in turn discourages people to use the public service and decreases the willingness to pay the tax. Low tax revenue then again, weakens the government's ability to provide the quality service. This situation occurs also in ODA for health. Corruption diminishes the actual amount of fund for execution of program, deteriorating outcomes, which in turn lowers the willingness of donor countries to donate.
Corruption occurs in various forms, both in HIV/AIDS treatment and prevention programs. However, it is known to be more frequent in treatment of HIV/AIDS than the prevention due to high price of treatment medicine. Corruption can occur in any stage through production, procurement and distribution of the medicine (12). The magnitude of disease prevalence, stigmatization attached to the disease, and high treatment cost further raise the possibility of corruption in HIV/AIDS aid. Therefore, the HIV/AIDS aid budget expansion without proper mechanism for controlling corruption would do nothing but to increase the possibility of corruption.
The kinds of corruption committed by higher-level officials are to embezzle money assigned for HIV/AIDS program or siphon off medicine itself and resell them in informal market. Patients sometimes prefer informal market because they can purchase HIV/AIDS drugs at a lower price without stigmatization and the need to wait. However, in informal market, they can scarcely get proper information about dosage, side effects, and combination therapy. As a result, treatments become invalid, making patients fall into a more serious danger from adverse effects and heightening viruses' resistance to drugs.
Staffs at middle-level commit corruption such as demanding or accepting of bribes. Some HIV/AIDs patients exercise economic or political leverage to be enrolled onto fully or partly supported treatment program, making more severe and more urgent patients excluded from treatment (13). Like these, all corruptive activities can lead to exacerbated outcomes.
In addition to controlling corruption, promoting accountability is also currently being emphasized in developmental assistance as an important aspect of the good governance. Among all dimensions of accountability, democratic accountability which government should hold toward its own people is considered critical.
The main mechanisms to achieve democratic accountability are election, surveillance, public deliberation, petitions of a civil society, and mass media. A strong and active civil society can create an environment where citizens can engage in making a policy and deliver their complaints through various ways such as mass protest or civil disobedience about governmental corruption. Civil society can also have an impact on HIV/AIDS outcomes by contributing to HIV/AIDS fund-raising and thereby, making it possible to perform more comprehensive and diverse projects. Similarly, the media with autonomy can monitor governmental activities about HIV/AIDS and force a government not to neglect those activities (141516).
On the other hand, some argue that there is reverse relationship between democratic accountability and HIV/AIDS outcomes. For example, HIV/AIDS disease destroys not only the society's technical infrastructure by lowering productivity but also the capability to secure people's welfare, which in turn, impairs the governance system of a country (17). As such simultaneous effects between HIV/AIDS diseases and democratic accountability create a vicious cycle (18), the importance of democratic accountability should be emphasized further (19).
Based on these backgrounds, this study was conducted for three purposes. First, we tried to answer the question on whether the good governance of a recipient country, measured by the control of corruption and democratic accountability, is a necessary condition for low HIV/AIDS prevalence in the recipient country. Secondly, we examined what other factors are combined with governance to explain low HIV/AIDS prevalence in recipient countries. Thirdly, this study provided empirical evidences on combinational conditions in each country such as Belarus, Moldova, and Bolivia.
MATERIALS AND METHODS
Data
Analysis was performed with a dataset of 47 countries which have received HIV/AIDS ODA between 2002 and 2010, when the international society has started to take an interest in aid-effectiveness and began more systematic efforts for eradication of HIV/AIDS (202122).
Average values over the 9 yr in each factor were calculated and used in the data analysis due to the reasons as follows. Although properties of causal conditions and outcomes are scored in figures, Fuzzy-set analysis requires capturing qualitative information of those data. If the data on specific time point were used, outliers from exceptional situation which can't be seen as a qualitative property were likely to be included. An averaging of values for a longer period could smooth out this unusual effect. Indicators for causal conditions and outcome, and their data source are shown in (Table 1).
Analysis framework and variables
In this study, we identified nine potential attributes for a causal configuration for HIV/AIDS outcomes through a review of previous studies (Fig. 1).
Governance factors were already explained in detail above. Regarding the cultural factors, Muslims inhibit extramarital sexual relationship, alcohol consumption, encourage circumcision, all of which serve as the suppressing factors of HIV/AIDS (23). Ethnic fractionalization tends to trigger conflicts of opinions among policy makers impeding economic development and damaging governance. These conditions give negative impacts on HIV/AIDS outcomes (24). According to Hughes (25) who argued that rent-seeking behavior was the most severe between different ethnics, corruption was also more frequent in ethnically-fractionalized country.
As the socio-economic factors, a high rate of unemployment and low wage increase the number of population working in sex trade, which facilitates the spread of HIV/AIDS (26). Previous studies showed that the gender gap in income level also had relevance to HIV/AIDS outcomes (7). Women in economic vulnerability have a better chance of working in sex trade for financial purpose than the men under the identical conditions where they can be exposed to un-protective environment from HIV/AIDS infection. In this study, the difference in enrollment rate on essential education was used as proxy variable for gender economic inequality. People in advanced economic condition might have better access to information technology, especially to internet, giving them better chance to obtain HIV/AIDS-related information. Lack of proper information about safe sexual culture, or refusal skill against risky sexual activity increases probability of HIV/AIDS infection. Proportion of internet user was used to represent to this concept. Overall economic inequality may have relationship with a high HIV/AIDS prevalence for several reasons. From an economic perspective, in economically-polarized country, low-income people are vulnerable to infection due to high possibility to be exposed to risky sexual culture while high-income people also raise prevalence through another route such as purchasing sexual partners using their wealth (27). An explanation from social perspective emphasizes the role of social capital and social convergence. Unequal distribution of income might disrupt social cohesion, which can make a society difficult to communicate each other with mutual trust and prevent from mobilizing human capital and resource necessary for pursuing common goal of controlling HIV/AIDS (28). In terms of a political perspective, an unequal society has a poor-functioning public system for controlling HIV/AIDS disease (29).
As a last factor affecting people's general health status, the variables related to health behavior and clinical care were included. Because HIV/AIDS is mainly transmitted through sexual contacts, safe sex behavior is considered important. The share of condom use was used to represent this concept. Clinical care means accessibility to treatment and preventive medical service for which healthcare expenditure can be proxy measure as it may have an effect on supply of overall healthcare service including HIV/AIDS (30).
Analytical approach
Data calibration to fuzzy-set scores
To begin with, the three qualitative breakpoints such as full membership, full non-membership, and crossover point should be specified to calibrate degree of membership in a outcome fuzzy-set. While Ragin suggested that this process should be based on researcher's theoretical and substantive knowledge rather than data structure, many of the cases did not often have well-established theoretical criteria indicating what level of causal condition would belong to the outcome fuzzy-set or not (10). Even decisions based on ample knowledge were always subject to external criticism for subjectivity. Thus, many of the previous fuzzy-set studies had used statistical information based on data structure rather than researcher's qualitative knowledge. This study used either one of author's knowledge or statistical information of the variable, depending on appropriateness for each condition. Calibration and establishment of a truth table were conducted using Fs/QCA 2.0. In addition, Stata/SE 11 was used for probabilistic tests of necessary and sufficient conditions for low prevalence of HIV/AIDS.
Low prevalence of HIV/AIDS
Classification of HIV/AIDS epidemics suggested by World Health Organization (WHO) & The Joint United Nations Programme on HIV/AIDS (UNAIDs) was referenced for calibration (Table 2). When this classification is applied, a group of hyper-endemic countries accounts for top 5% of 47 countries. So countries with above the 15% prevalence were fully out of the set of low-prevalence countries. 1% of prevalence separating low-level from generalized epidemic was set as a crossover point. This value was approximately equal to 0.84%, the median value of HIV/AID prevalence in this dataset. On the other hand, there was no information about a cut-off value for fully-in to the low-prevalence of HIV/AIDS set. Based on statistical information, 0.1% of prevalence rate, a lower 5% level of prevalence of HIV/AIDS in the dataset was selected for cut-off value for fully-in.
Governance factor
Governance factor was comprised of two variables which were the control of corruption and voice & accountability of recipient countries and each one was weighed equally. The Worldwide Governance Indicator (WGI) data of World Bank showed an almost normal distribution between the scores of -2.5 and 2.5 and there was no specific standard on which level can be considered as good or bad governance. Therefore, the maximum value of the dataset was set to criteria for fully-in to a good governance country set, the minimum value of the dataset for fully-out, and the median value for the cross-over point. In this case, 0.95 of the weighted value was applied to the maximum and minimum values so that data could be distributed more diffusely toward both extremes (31).
Cultural factor
Ethno-linguistic fractionalization index measures the probability that two randomly selected individuals from a population would belong to different ethno and linguistic groups. The breakpoints for fully-in, cross-over, and fully-out for the high fractionalized country set were determined in the same way as assigning the values for the set of governance factor.
The share of Muslims showed an uneven distribution, with high concentration in specific part of the countries. Although about 46% of countries had below 1% of share of Muslims, the median value was almost the same as the 50%-level of dataset. Therefore, the maximum value was chosen as the cut-off point for fully-in, the minimum value for fully-out, and the median for cross-over point.
Socio-economic factor
From the purely theoretical perspective, Gini coefficient for a completely unequal country should be 100 and for completely equal society to be 0 (The original value of Gini coefficient ranges from 0 to 1. The World Bank presents the Gini-coefficient as multiplied by 100). However, such a country does not exist in the real world. The Gini coefficient of the most equal country in this dataset was 27.8 and the most unequal one was 65.8. The maximum and minimum values were set as the cut-off points for fully-in and fully-out for the set of unequal countries.
In approximately 40% of countries, the number of girls enrolling in primary and secondary education was higher than that of the boys. Although we cannot pinpoint what ratio is the gender equality status, we certainly know that a higher figure apparently indicated a narrower economic gap between male and female. Therefore, the maximum, minimum, and median values were determined as fully-in, fully-out, and the cross-over thresholds for a set of economically-equal country between men and women.
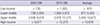
For calibration of the set of economically developed countries, the income classification by GNI per capita of World Bank was consulted. To begin with, an average of each endpoint at year 2002 and 2010 were calculated (Table 3). When these standards were applied to our dataset, only 1 country (about 2%) belonged to the high-income group, 32% to the upper middle one, 53% to the lower middle one, and 13% to the low income group while more than 30% countries would fall under the high-income group if it is applied to the entire countries of the world. This was due to the fact that the incomes of the countries were located in the lower part of entire countries' income distribution since the data in this study was consisted of recipient councountries of HIV/AIDS aids. For this reason, we decided that the cut-off value for fully-in to the set of high income countries needed to be lower than criteria suggested by World Bank. The highest income country in our dataset was Chile, which showed $13,243 (International Dollar, Purchasing Power Parity [PPP]) of a GNI per capita. However, it was presumed to be an abnormal outlier because there was difference of more than $300 from the second highest country. Therefore, the second highest value was selected as the cut-off value for fully-in to the set of high income countries. The median and the minimum values were selected as the cross-over and fully-out thresholds.
Any criteria widely accepted by academia or working field could not be found regarding the share of the household with TV. Therefore, the maximum, the minimum, and the median values were selected for fully-in, fully-out and cross-over points.
Health-related factor
The share of health expenditure out of Gross Domestic Product (GDP) of a country and the contraceptive prevalence had no particular theoretical grounds for setting the threshold. Therefore, information about relative distribution of the data was used as criteria for creating the sets.
Analyses
Three cut-off values in each factor were converted to fuzzy-set scores by a direct method which was automatically applied in Fs/QCA 2.0 program. Once all measures are calibrated, the next step of the analysis involves creating a "truth table," a data matrix summarizing the property space occupied by our nine theoretical attributes (28). A truth table lists all logically possible combinations of conditions and outcomes, so called 'corner' (10). In this study, there were total of 256 corners in the truth table because the number of causal condition was 9 (29=256). All the cases were distributed across those 256 corners and more than 0.5 fuzzy-set score was considered to belong to each pertinent corner.
Corners with no or extremely few cases can be interpreted as indicating that a country with those combination of conditions is rare in the reality and therefore, it can be excluded from the analysis. This is called "remainders." Researchers can set frequency-threshold determining whether certain combination is a "remainder" or not (which is called "relevant"). In this study, combinations of conditions having more than 2 cases were considered as relevant and as a result, 7 combinations of conditions were left after remainders were excluded. Total 19 cases which fell under 7 relevant combinations were analyzed by probabilistic tests for necessary and sufficient conditions for low prevalence of HIV/AIDS countries.
Set-theoretic consistency measures "the degree to which the cases sharing a given combination of conditions agree in displaying the outcome in question" (10). In other words, consistency can be interpreted like significance in statistical analysis. In this study, benchmark for consistency was set to 0.65 ('usually necessary'), indicating that when the number of combination of causal conditions with its score higher than fuzzy-set score of outcome is above 65% statistically at P value 0.05, that combination would be considered to be 'necessary'.
The evaluation of sufficiency is a test on whether the cases displaying the causal combination of conditions form a subset of the cases displaying the outcome of low prevalence of HIV/AIDS. The pathway for a low HIV/AIDS prevalence can be more than two (32). Benchmark for consistency was 0.8.
RESULTS
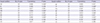
A result of test for the necessary condition, which was the first objective of this study, showed that good governance, low ethno-linguistic fractionalization, high level of economic development, low income inequality, low gender inequality in economic status, and the low share of health expenditure of GDP were the "usually necessary" conditions for the low prevalence of HIV/AIDS in recipient countries. It is important to note that the result of 'necessary' condition does not always mean that there is a causal relationship between the variables. It is just a product of ex-post facto process of extracting common causal conditions from the real data (Table 4).
The probabilistic sufficiency test for identifying combination of causal factors, which was the second objective of this study, produced two combinations of conditions for low prevalence of HIV/AIDS (Table 5). The first one showed that a low level of governance can lead to low HIV/AIDS prevalence when it is combined with low ethno-linguistic fractionalization, a high level of economic development, low income inequality, low gender inequality, a high share of household with TV, a high percentage of health expenditure, high contraceptive prevalence, and a low share of Muslim, which was observed in the two countries, Belarus and Moldova. This combination showed 0.95 of consistency and 0.21 of coverage.
A second pathway to low prevalence of HIV/AIDS differed from the first one that economic inequality and governance were included in opposite direction to the ones in the first combination, and the high health expenditures factor was not included. This combination showed 0.95 of consistency and 0.32 of coverage.
Fig. 2 is a scatter plot representing fuzzy-set scores of combined causal conditions on X axis and fuzzy-set scores of outcome variable on Y axis of each 47 countries. Most of the cases were located in upper-left area above the diagonal in both pathways, meaning that the consistency is high. Although a large proportion of country was located above the diagonal, the distribution, especially in first pathway, was skewed to the left indicating that the cases contributed to explaining the fact that their combinations of conditions are sufficient for outcome, but the coverage of explanation is low. A few countries which were situated below the diagonal can be said to be an evidence against the conclusion that those pathways are the sufficient conditions for the outcome. However, because they are not far from the diagonal, they don't have explanatory power that can reverse the conclusion.
Interpretation and exemplifying-based discussion
This study was performed for mainly two purposes. The first was to identify the necessary conditions for low prevalence of HIV/AIDS. The second was to analyze configuration relationship between several factors including governance and low prevalence of HIV/AIDS in HIV/AIDS ODA recipient countries.
One notable finding from the first analysis was that the low share of health expenditure turned out to be a necessary condition for a low prevalence of HIV/AIDS, contrary to findings in previous studies (30). Possible explanation for this is that the causal relationship between high health expenditure and improvement of health does not necessarily happen in all disease areas.
We identified two possible pathways for reaching the low prevalence of HIV/AIDS from the second analysis. The first combination exemplified in Belarus and Moldova consisted of individual conditions which had been proved in the previous studies to decrease HIV/AIDS prevalence apart from low governance and a low share of Muslim. In other words, even a country with low share of the Muslims and not-good quality of governance can keep a low HIV/AIDS prevalence if the rest of conditions in the country were favorable for low prevalence of HIV/AIDS. However, it is difficult for the country with rapid economic growth to distribute its benefit evenly across all the citizens in such a short time. Indeed, this combination appeared only in two countries.
Each pathway would be understood better by reviewing the example countries. The first example country for the first combination of conditions is Belarus which has performed a joint project called "Prevention and treatment of HIV/AIDS in the Republic of Belarus" from 2004 to 2009. It focused on counseling and preventive activities for the main source of infection and vulnerable group such as intravenous drug users (IVDU) and sex workers. This program has been regarded as very successful and promised to be funded until 2015. The country's economy has grown rapidly since 2000, showing 8.2% of average growth rate from 2002 to 2005 and even reaching 10% at 2006. Good economic condition like this also enabled people to be better equipped with various tools to access the information about disease. In addition, Belarus showed income inequality as low as advanced post-socialist countries in Central Europe. This was possible due to several reasons. First of all, most of the Belarusians had relatively homogenous skills and educations during the transition to market system. Secondly, Belarus government retained much of comprehensive social security system, especially in healthcare and education since the collapse of a former Soviet Republic regime. Finally, many Belarusians could get a stable wage because they did not privatize the biggest companies of Soviet Republic regime (33). The low inequality not only kept poor people from working in sex-trafficking but also made it possible for poor patients to have access to treatment.
However, compared to these favorable conditions for keeping low HIV/AIDS prevalence, Belarus had relatively weak governance. There has been widespread corruption, a lack of political freedom, and an absence of mechanism through which civic society can raise their voices (34). Especially, in mid-2000s, the governance became even worsened as they did not conduct re-arrangement of public organization even after the key high-level officials were sent to prison due to corruption. Independent civil societies disappeared gradually due to the pressure from government. Not only were the 56 leading NGOs abolished, but also 90% of newly created NGOs were rejected for registration. The situation of media was the same as well. A few top independent newspapers were prohibited from publication. The government-owned press did not have any willingness to express fair opinions (35). Result from this analysis showed that despite the poor governance like this, fast-growing economy, relatively fair income distribution, and comprehensive provision of public service combined with successful implementation of HIV/AIDS strategy could result in low prevalence of HIV/AIDS in a country.
Moldova also had similar conditions. Corruption was a long-standing problem which had started from the 1980s and kept spreading in contagious way ever since. At the initial transition period to a free market system, the number of corrupted individuals was low while its scale was large. However, at later stage, the number of illegal transaction in market also increased significantly. In fact, there have been various corruption-encouraging factors in Moldova.
Specifically, legal factors such as disputable and behind-the-times law, the institutional factors including lack of willingness to tackle corruption and policies inducing rent-seeking, economic factors such as low and delayed payment of wage to civil servants, and finally, social factors such as low morality of public officials, lack of media activity were all working for triggering corruption. Corruption siphoned off money that was supposed to go into healthcare, giving direct effect on health outcome. However, despite of corruption and poor democratic accountability, Moldova has maintained low HIV/AIDS prevalence due to other advantageous conditions as below (36).
Economy in Moldova has been showing significant growth since the independence from the Soviet Union in 1991, mainly due to the contribution by remittance from emigrant workers. This led to increase in overall budget and health expenditure, which could in turn lower the infant mortality rates and maintain relatively high life expectancy (37). Although inequality increased during 1990s from unemployment, corruption, and illegally acquirement of fortunes which appeared in the wake of reforms after independence, they recovered again and could maintain quite equal status during 2000s. In addition, Moldova started 'AIDS control project' funded by International Development Association (IDA) in 2003 for scaling up prevention, treatment and management of HIV/AIDS, and building institutional capacity for HIV/AIDS control. This effort stabilized the life expectancy of HIV/AIDS patients, decreased mother-to-child transmission of HIV more than 90%, and slowed the spread of the disease among youth and IVDU (38). Moldova case implies that a high economic growth accompanied with quite even economic status among people can offset negative impact of poor governance on HIV/AIDS outcomes. But, these two countries, which showed rapid economic growth after market transition and kept level of inequality low at the same time, were rare cases and not common in the real world.
On the other hand, the second pathway for low prevalence of HIV/AIDS consisted of the same conditions as the first pathway except for the two factors. That is, directions of Gini-coefficient and governance were reversed and the condition of healthcare expenditure was dropped from the configuration. In the light of the first combination of conditions, this can be interpreted that, if governance is good, they can keep HIV/AIDS prevalence low, regardless of a level of share of healthcare expenditure, and even when inequality is high.
Bolivia, Chile, Costa Rica, Peru, and El Salvador were example countries for second sufficient condition. Bolivia showed a significant improvement in macro-economic performance due to their ample natural resources such as hydrocarbon and rare minerals. However, it showed unequal economic status. Accessibility to social security was uneven and poverty rate was unusually high in specific group (39). In fact, governance level of Bolivia was not high but just modest, showing that its fuzzy-set score barely managed to go over the cross-over point. Especially, corruption has been more prominent problem compared to the democratic accountability and the fact that country's economy depended mainly on natural resource was one of the factors encouraging this corruption. However, Evo Morales who began his term as president in 2006, has made an enormous effort to improve transparency, declaring "zero tolerance for corruption" and then making solid institutional and legal framework. As a result, WGI score climbed from bottom 20% level in early 2000s to bottom 40% level in late 2000s. On the other hand, the democratic accountability has been kept in high level ever since early 2000s. There were many chances for civil society to participate in policy-making process and local authorities showed fast responsiveness to the needs of civil society (40).
Bolivian government's initial response to HIV/AIDS had not been so successful. Resource going into HIV/AIDs program was neither evenly distributed nor sustainable because the coverage of healthcare system in Bolivia was low. Nevertheless, Bolivian government has made an incessant effort for HIV/AIDS control such as joint signing of several state department on implementation of the "Adoption of Attitudes and Practices" to prevent HIV/AIDS in 2007. When evaluated overall, Bolivia's conditions such as modest level of governance, steady efforts of government for control of HIV/AIDS, and economic growth could keep low HIV/AIDS prevalence, offsetting adverse effect of high economic inequality.
HIV/AIDS prevalence in Costa Rica was low and has decreased further due to improved accessibility to treatment drug of HIV/AIDS. It was the only country in the Central America sub-region with a universal access to anti-retroviral therapy. They have enjoyed relatively high quality of life for quite a long time from good economic condition. They also had good governance. Due to a electoral democracy, average accountability score of WGI ranked at top 75% level during 2002-2010. Media and activities of NGOs were free of intervention from government and there was no restriction to the accessibility of the internet. Freedom of assembly was protected by constitution (41). Appropriate and effective investment in healthcare reform for several decades enabled Costa Rica to establish health system based on values of universalism, solidarity and equity, which had become solid foundation for success of HIV/AIDS program. Costa Rica passed the general law on HIV/AIDS, approved legislation for protecting HIV patients against stigmatization and discrimination in 1988 and has continuously developed and adapted treatment protocol and guidelines for clinical care of HIV/AIDS. Likewise, the government made an effective and well-balanced effort between the treatment and prevention with high political commitment (42). However, Costa Rica could not avoid high economic inequality mainly because their economic model had been based on mercantilist system which tends to be biased toward certain favored sectors of the economy (exports, tourism) at the expense of the poor (43). In summary, a combined effect of stable economic status and quality of life, strong democratic accountability and less corruption, appropriate and effective investment in healthcare and political leadership, and continuous effort of government could result in low HIV/AIDS prevalence, offsetting ill effect from high economic inequality. Other case countries such as Chile, Peru and El Salvador had a similar history.
Although this study took useful first step toward identifying configurational conditions for good HIV/AIDS outcomes in HIV/AIDS ODA recipient countries, it is also subject to a few limitations that we hope other research can take as a starting point for future studies. First, although securing good quantity and quality of data is an essential for reliable result, there were non-negligible amount of missing data in our study because all of the target countries belonged to developing countries. Those countries do not have systematic support system for collecting information. This study used the average value of each variable between 2001 and 2010 to reflect not temporary variation but country's essential attribute. But due to data insufficiency, in some variables of some countries, only values of a few years were averaged.
Second, although there were more conditions determining the HIV/AIDS outcomes, it was impossible to consider all of them because the number of combination of them would become so huge and unmanageable. We tried to categorize them into smaller number of higher level of concepts but there was no solid theoretical background to do so. We thus encourage future research to consider more variables by merging them into smaller number of higher level of categories based on more reliable theoretical background.
Finally, there is no much theoretical explanation about interaction between factors while their independent effects on HIV/AIDS outcome have been discussed a lot. If inter-wined effects of these nine factors are further analyzed through qualitative study in example countries, the result of this study will be a more practical guideline for political measure. For these reasons, the result of this study should not be overly generalized when interpreted.
CONCLUSION
Researchers' view on diseases has been increasingly stressing a holistic perspective that emphasizes the effects of social factors and their interaction on disease, shifting from only bio-medical perspective. HIV/AIDS is the disease which is influenced by social contexts more than any other disease. It means that there is no country where a single factor can keep low HIV/AIDS prevalence and various elements work jointly. Therefore, it would be more realistic to identify the effect of combination of factors on HIV/AIDS outcome rather than the effect of each separate factor as in econometric analysis. To our knowledge, this study is the first to explore the effect of combinations of relevant factors on HIV/AIDS outcome in recipient country using Fuzzy-set QCA and has the following implications in this regard.
The result of this study implies that the policy measure focusing on only specific, narrow area would have no or very little impact on HIV/AIDS outcome. Increasing health expenditure cannot necessarily be linked to low HIV/AIDS prevalence because funding invested in health can be leaked by corruptive activities. Also, no matter how affluent the country is, if there is a high economic inequality, some poor people will not be able to have access to the treatment and become source of infection to other people. Thus, comprehensive and simultaneous approaches are necessary to control HIV/AIDS.
Component factors worthy of notice are governance, economic inequality, and share of health expenditure. While other six conditions were included the same in both two pathways, these three showed a kind of "tradeoff". More specifically, good governance can compensate a high level of economic inequality of a country. As explained before, even if there is pathway to achieve relatively low prevalence of HIV/AIDS without good governance, it is not easy in the reality to achieve fast economic growth and to distribute benefit from growth equally at the same time. For this reason, enhancing governance is more practical and key policy measure. In addition, there are increasing evidences that good governance can have strong egalitarian effects. Recent cross-country study found that good governance can reduce poverty and improve the distribution of income (44).
Strengthening accountability can have a ripple effect on the control of corruption because accountability is more comprehensive concept than any other dimensions of governance and therefore, it is worthy of more attention and effort. Democratic accountability is entrenched in each country's contexts such as their own political situation, incentive scheme, and formal as well as informal balance of power. Therefore, for raising democratic accountability, in-depth understanding of governance context of a recipient country and motivation factors related as well as non-related to aid are essential. All the actors should make a collaborative effort along with recipient government because all the activities of them play a certain role in shaping governance of recipient country.





 XML Download
XML Download