

 PDF
PDF Citation
Citation Print
Print



India has the dubious distinction of having the highest prevalence of underweight and ranks 7th in stunting prevalence among children below five years (1). According to the 2005-2006 National Family Health Survey (NFHS) of India (2) (no national survey has reported results since then) the prevalence of childhood stunting and underweight was 48% and 42.5%, respectively. India accounts for 38% of the global burden of stunting with more than 61 million children having abnormally low height-for-age (3).
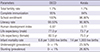
A pertinent characteristic of the levels of child undernutrition in India has been its persistence. While prevalence of underweight among children aged 0 to 35 months decreased from 49% to 40% between 1992 and 2005, the decrease in stunting was only 7 percentage points over the same period (4). This aspect of persistence is particularly borne out when we examine Kerala (Fig. 1), a state that has received considerable appreciation for remarkable accomplishments on social and health indicators (5). While Kerala compares favorably on a number of key population health indicators (Table 1) with the member countries of the Organization for Economic Cooperation and Development (OECD) (which are approximately 11 times richer in terms of per capita gross domestic product [GDP]), it fails considerably on measures of child nutritional status, as captured through anthropometric measures (67). Childhood underweight and stunting are virtually absent in OECD countries, however, about a quarter of children in Kerala are either underweight or stunted. In fact, prevalence of stunting remained unchanged in Kerala between 1992 and 2005, while underweight prevalence dropped by a mere 8 percentage points over that 13-yr period.
The sluggish decline in child undernutrition in India, ironically, was accompanied by a period of bullish and sustained economic growth. India experienced growth rates greater than 7% between 1994 and 1997 and about 8% or greater rate in 2004 and 2005 (8). It is not an exaggeration to state that in countries with low levels of per capita income, such as India, increasing the rate of economic growth is often justified as a key policy instrument to improving population health and nutrition (910).
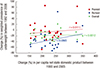
Although increased economic growth could play a role in reducing child undernutrition, unfortunately there is no compelling evidence to support that. On the contrary, in a recent study that comprehensively examined the role of economic growth in explaining even the small decline in child undernutrition in India, the correlation was close to zero (11). The essentially null association between increases in state economic growth and reductions in child undernutrition was, by and large, true across all socioeconomic groups (11) and particularly evident among the poorest wealth group (Fig. 2) (12).
The evidence from India that macroeconomic growth at the state level did not contribute to the (slow) reduction in child undernutrition has also been corroborated at the global level. In an analysis of 121 Demographic and Health Surveys in 36 low- and middle-income countries, the association between macroeconomic growth and reductions in childhood measures of anthropometric failure was zero to quantitatively very weak (1314). This finding was found to be consistent across a wide range of statistical specifications (14).
If policies to address child undernutrition are to be based on "evidence", it is clear that a "growth-mediated" strategy is unlikely to yield desirable results, at least in the short run. Indeed, upon reflection, it is not at all surprising that macroeconomic growth over the last couple of decades has not translated into substantial improvements in children's nutritional status in India. For instance, it is now largely agreed that the benefits of economic growth did not "trickle down" to the poor, let alone the poor being participants of such growth (15). Interestingly, the very widespread use of the phrase "trickle down" implies that even in the best case scenario one can expect only a "trickle" and not a "flood." Thus, even if it were the case that economic growth led to increases in incomes of individuals, and especially those of the poor (where the majority of the burden of child undernutrition exists) (4), this would still impact very few of the proximal risk factors that causally affect undernutrition, such as access to sufficient food and micronutrients. Indeed, in India, where food inflation has been rampant, there is no evidence that income improvements have vastly outstripped the food inflation, especially for the poor (16). In fact, the evidence suggests a decline in calorie consumption in India (17). Importantly, reduction in child undernutrition is dependent on other risk factors that are unlikely to automatically improve as a consequence of increases in household incomes. These include access to clean water and sanitation, as well as to treatments that reduce recurring morbidities and prevention of infection through immunization. Improvements in these conditions are influenced by robust public investments, which often depend more on the policy and political priorities than on the availability of resources. And if not evaluated rigorously these public investments can present an erroneous picture of success. For example, even though India appears to have met the Millenium Development Goal on access to water, a recent analysis found alarmingly high contamination rates of water from the "improved" water sources in India (18). In addition to these proximal risk factors, it is well known that there are social and intergenerational factors that influence child undernutrition, critical ones being paternal and maternal height (19202122).
In conclusion, before advocates of growth-mediated strategy extol the role of macroeconomic growth as a policy instrument to reducing child undernutrition it is critical to first recognize the etiology and mechanistic connections. If economic growth is actually "pro-poor" and the increased public revenue as a consequence of such growth is invested in mitigating the proximal and distal risk factors that matter for child undernutrition, such growth can have an impact on child undernutrition. Sadly, the evidence thus far appears to be the contrary.

 XML Download
XML Download