

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
In April 2014, the 7th meeting of the Strategic and Technical Advisory Group (STAG) for neglected tropical diseases (NTDs) was held at the World Health Organization (WHO) in Geneva, Switzerland. The STAG coordinates global activities of NTD control and endorses recommendations by related Working Groups on specific diseases. Conclusions of the STAG meeting in 2014 include 6 main issues of concern (1): 1) support for countries to increase coverage with integrated interventions; 2) establishing principles and processes of verification, validation, and certification; 3) positioning NTDs in the post-millennium development goals (MDGs) 2015; 4) mobilizing resources for yaws eradication; 5) accelerating the work to control neglected zoonotic diseases; and 6) responding to the dengue epidemic. These issues are major ongoing topics of NTDs in view of global health.
NTDs are characterized as a wide range of infectious diseases of the poorest population in the tropics. There are many NTDs in the tropics but some of them are targets for control, elimination, and eradication by WHO when the MDGs included them with malaria and AIDS by 2015. Thanks to the MDGs initiative, many private or public international funds have supported control activities of NTDs over the world. The 2012 London Declaration committed to implement global control activities on 10 NTDs: lymphatic filariasis (LF), trachoma, soil-transmitted helminths (STHs), onchocerciasis, schistosomiasis, leprosy, guinea worm disease, visceral leishmaniasis, Chagas disease, and human African trypanosomiasis (2). The global efforts to achieve MDGs have recognized that NTDs are becoming less neglected but it is not enough. Still, the global efforts have covered 36% of people who are in medication need for NTDs (3). It is almost the end of the MDGs and time to start post-MDGs 2015 (SDGs: Sustainable Development Goals). That is why the STAG meeting 2014 concluded to anchor the control of NTDs in the SDGs.
NTDs are diseases of the poor, vulnerable, and voiceless people. Furthermore, most of the victims are children in the tropics. Over one billion people are suffering from or at risk of NTDs. NTDs are still neglected diseases of neglected people over the world although there are many on-going control programs in the world.
In Korea, intestinal helminths, mostly STHs, were highly prevalent in the past, which were one of public health concerns of priority. The Korean society and influential decision makers agreed systematic control of intestinal parasites, control of tuberculosis, and family planning as priorities of the national health agenda. The nationwide programs of the 3 health agendas had been implemented together in 1960s-1980s.
The present article briefly introduces NTDs control programs by Korean initiative and reviews global status of NTDs.
KOREAN PERSPECTIVES FOR NTDs CONTROL
Elimination of STHs in Korea
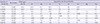
In 1965, the Korean government passed the law for "Prevention of Parasitic Diseases," which declared compulsory nationwide screening of STHs and mass chemotherapy in schools. Based on the law, systematic nationwide control activities had been implemented by targeting school age population over the country from 1969 to 1994 (4). In addition, the status of intestinal parasite infection was monitored by nationwide statistical sampling every 5 to 8 yr since 1971 (5). Twenty years have passed since the stopping of mass chemotherapy but the status of STHs remains extremely low in Korea (Table 1). According to the national survey on the prevalence of intestinal parasitic infections in 2012, egg positive rates of A. lumbricoides, T. trichiura, and hookworms were 0.03%, 0.41%, and 0% in Korea (5).
The success was achieved within 20 yr of systematic control activities. Several factors may be considered for the success (46): 1) systematic anthelminthic medication covered whole students over the country until egg positive students disappeared; 2) social agreement of its priority by the specific legislation strongly supported the control; 3) synergy by social campaigns of 'Saemaul Undong' (New Village Initiative) and educations with other health affairs and self-driven movement boosted the control activities; and 4) economic development and increased income had fastened the success by expanding social infrastructures.
The successful experience of Korean parasitologists in STHs control has been transferred to China, Tanzania, Myanmar, and Fiji (789). The Korea-China collaborative project of control strategies for helminthiases was undertaken from 2000 to 2004 with financial support from the Korea International Cooperation Agency (KOICA) (7). The aims of this collaborative project were to support the development of nationwide project of control strategies for parasitic infections in China and to build up the capacity of Chinese institutions to control parasitic infections. This project for STH control was performed in nine villages, four high endemic villages (prevalence of A. lumbricoides of 41%-49%) and five moderately endemic villages (21%-29%), in Jiangxi Province (7). Mass chemotherapy with albendazole (400 mg, single dose) once a year produced the highest reduction rate (86.1%) of ascariasis in high endemic areas, while selective chemotherapy twice a year showed a reduction rate of 69.3% in moderate endemic areas after four years of intervention.
In summary, most people were infected, realized the serious health impacts of STHs and paid attention to them. This self-awareness prepared a stable and strong background for the social agreement and forceful implementation.
Elimination of lymphatic filariasis in Korea
Lymphatic filariasis (LF) by Brugia malayi had been endemic in several southern islands of the Korean peninsula causing elephantiasis (10). Continuous screening and mass chemotherapy could have eliminated LF in previous endemic areas. The screening of residents by night blood smear was a serious obstacle for case detection, while mass chemotherapy with diethylcarbamazine was too toxic to be completed. Although both screening and chemotherapy of LF were difficult, the LF elimination program was achieved successfully through aggressive surveys by heath workers covering remote islands and voluntary or active chemotherapy of microfilaremia positive residents with diethylcarbamazine.
In addition to this effort, the improved living standards of residents by modernization and economic development in 1970s with heightened health awareness of people in avoiding mosquito bites by using bed nets or mosquito repellents greatly contributed to the decreased exposure to mosquitoes and prevented the propagation of the disease. Finally, the elimination of filariasis in Korea has been declared in 2008 (1011).
Korean initiatives to control NTDs over the world
During 1950s and 1960s, Korea was one of poorest countries in the world. Since many communicable diseases were seriously prevalent in all of Korea, various overseas donation programs supported control activities of communicable diseases including NTDs as well as solving other health related problems and socioeconomic development. The overseas donations aided survival of Korea and contributed greatly to disease control and socioeconomic development. The successful control of NTDs in Korea was supported by the overseas donation at the beginning.
Since Korean experts have successful experience in elimination of STH and lymphatic filariasis, NTD is a familiar agenda for international collaboration. There are many developing countries that require international donation and collaboration for control of NTDs and other diseases. In 1995, Korea became a member of the Organization of Economic Cooperation and Development (OECD) and started overseas donations to support developing countries. Several overseas programs on NTDs control have been implemented by many Korean organizations.
Two governmental and several non-governmental organizations have been running many projects. KOICA is the main representing donor in Korea for developing countries to support official development assistance (ODA). KOICA is affiliated to the Ministry of Foreign Affairs and covers the whole scope of ODA programs. KOICA has implemented a few projects on NTDs: 'Pilot Project for Control of Soil-Transmitted and Food-Borne Helminthiases in China (2000-2003)'; 'Building an NTD Hospital in Tanzania (2009-2011)'; 'Control of Malaria in DR Congo (2010-2012)'; 'Capacity Building for Communicable Disease Control in Uzbekistan (2011-2012); 'Capacity Building Program for Communicable Disease Control in Myanmar (2011-2014)'; and 'Combating Schistosomiasis in Sudan (2010-2014).'
The Korea Foundation of International Health (KOFIH) is another governmental funder for medical and health programs under supervision of the Ministry of Health and Welfare. KOFIH supported 'Control of Opisthorchiasis in Lao PDR (2006-2013)' and the 'Seoul Project in Lao PDR (2013-present).' The Seoul Project is an ongoing program of teaching young faculty members of the University of Health Science, Lao PDR, to upgrade research activity and clinical performance.
Several non-governmental organizations (NGOs) are executing multiple programs as well. Good Neighbors implemented surveys and mass drug administration for NTDs in Tanzania (2009-2014). The Korea Association for Health Promotion (KAHP) managed the 'Health Promotion in School Children in Mongolia (2005-2009)', 'Intestinal Parasite Control in Cambodia (2008-2012)', 'Health Promotion Project for the Elementary School Children of the Vulnerable Areas around Yangon, Myanmar (2013-2015),' and 'Health Promotion of School Children in Indonesia (2013-2016).' The Nanum International is running a program of rehabilitation for handicapped children in Ecuador (2013-2016) and began a new program in Peru (2014). The JW LEE Center for Global Medicine of Seoul National University supported a collaboration program of STH control in Fiji (2013-2014). These programs may include care or control of NTDs with priority of public health in the involved areas.
Overcome self-neglect
The disease elimination begins when the NTDs are no longer neglected. Who neglects NTDs? Why are they neglected? NTDs have been neglected by all: governments, health policy makers, fund donors, physicians, pharmaceutical companies, and even the victims. Self-neglect by victims is the core of the neglect. When the victims know about NTDs, early detection and active treatments are achievable. Furthermore, it is essential for prevention of the disease. When infected people ask for disease control with a big voice and do their best to prevent the infection, the diseases may be eliminated much earlier. Although more global resources are shared among NTDs programs now, many people still remain neglected and out of their coverage due to limited resources. Furthermore, self-neglect makes the programs less effective, that is why the overcome of self-neglect is important.
Comprehensive and sustainable program
In the control programs of NTDs, it is recommended to implement the programs with comprehensive intervention and sustainability. Otherwise, the control effect is transient and the NTDs will resurge as before. It is easy to lower the prevalence of NTDs with effective anthelminthics within a short period; however, the key point in programs of NTDs is keeping lowered prevalence by prevention of reinfection. In this context, all NTD programs should prepare sustainable strategies of reinfection prevention for its success.
GLOBAL STATUS OF NTDs AND CONTROL
Lymphatic filariasis
LF is caused by lymphatic dwelling filarial worms, Wuchereria bancrofti, Brugia malayi, and Brugia timori, which are transmitted by mosquitoes (Culex, Anopheles, and Aedes spp.). Currently, 1.39 billion people are at risk of the disease in 73 countries and about 80% of these people are living in 6 countries in South-East Asia and 4 countries in Africa (12). Over 120 million people are infected, and about 40 million suffer from morbidities of the disease such as hydrocele and elephantiasis (12).
Acute filarial disease accompanies episodic attacks of malaise, fever, chills, and enlarged painful lymph nodes (13). The painful and disfiguring manifestations of the disease, lymphedema, elephantiasis, and scrotal swelling, occur later in life and lead to permanent disability (12). The patients are not only physically disabled, but also suffer mental, social, and financial losses resulting in stigma and poverty (12). The disease is diagnosed by observation of microfilariae in thick smear of blood, which is collected at midnight. Immunodiagnostic tests, PCR, and ultrasonography can also be used for diagnosis (13).
The Global Programme to Eliminate Lymphatic Filariasis (GPELF) was launched in 2000 by WHO with two aims: interruption of transmission of LF and morbidity management and disability prevention (14). Large-scale treatment by mass drug administration (MDA) involves a single dose of two drugs, albendazole (400 mg) together with ivermectin (150-200 mg/kg) or with diethylcarbamazine (DEC) (6 mg/kg), given annually to entire population in endemic areas (12). MDA should be implemented annually for at least five years, which can reduce microfilaremia in infected persons to prevent the spread of transmission to mosquitoes (14). It has been shown that the transmission of LF in at-risk populations has dropped by 43% since the beginning of the GPELF (12). A minimum package of health care is provided to every affected persons in endemic areas for morbidity management and disability prevention (14). Surgery can alleviate most cases of hydrocele. Simple measures of hygiene, skin care, exercise, and elevation of affected limbs can improve clinical severity of lymphedema and acute inflammatory episodes (12).
Mosquito control is another supplemental strategy supported by WHO. It is used to reduce transmission of LF and other mosquito-borne infections. Insecticide-treated nets or indoor residual spraying may help protect people from infection (12).
The activities of GPELF are estimated to have prevented 6.6 million new LF cases in children between 2000 and 2007, and to have stopped the progression of the disease in another 9.5 million already infected people (15). According to the progress report on the elimination campaign for LF by WHO, 53 countries have implemented MDA, and 37 have completed five or more rounds in some areas among 81 countries with endemic LF (16).
Soil-transmitted helminthiasis
STHs are caused by intestinal nematodes such as Ascaris lumbricoides, Trichuris trichiura, and hookworms (Ancylostoma duodenale and Necator americanus), and are transmitted through soil contaminated with eggs of these nematodes. It is the most common parasitic disease of humans and about one fourth of global population is infected (17). It affects the poorest and most deprived areas in tropical and subtropical areas of sub-Saharan Africa, Latin America, Southeast Asia, and China. Children are more vulnerable to STHs than adults, and the nutritional impairment caused by STHs has a significant impact on growth and physical development in children (18); therefore, they are in need of treatment and preventive interventions for STHs (19).
People with light infections usually have no symptoms, but heavy and/or chronic infections can cause diarrhea, abdominal pain, general malaise, and weakness. Hookworms cause chronic intestinal blood loss, resulting in iron-deficiency anemia.
Control measures of STH include periodic drug treatment (deworming), health education, and improved sanitation (17). In endemic areas, deworming is performed to entire population regardless of symptoms, which is often done among school-age children (2021). This intervention reduces morbidity by reducing the worm burden. WHO recommends annual drug treatment in areas where between 20% and 50% of people are infected, and a twice a year treatment if it is over 50%. In low risk areas with less than 20% prevalence, only infected individuals are treated (22).
Broad-spectrum benzimidazoles such as mebendazole and albendazole are recommended for deworming by WHO. Mebendazole can be given with a single dose twice a day for three consecutive days and albendazole is given at a single dose. The drugs are effective, inexpensive and easy to administer by non-medical personnel (e.g. teachers) (17).
The global target is to eliminate morbidity due to STHs in children by 2020 (17). This will be obtained through regularly treating at least 75% of the children in endemic areas (an estimated 873 million). In 2012, 285 million children in need of treatment received anthelminthics for STHs corresponding to a global coverage of 32.6% (17).
Recently, control activity for STHs has been initiated in Fiji to promote health of primary school children by Korean parasitologists. This project includes training the personnel for parasitological diagnosis, building up the capacity of Fiji to control STH, and finally establishing the central reference laboratory for parasitic diseases in Fiji for control of STH in Pacific Islands.
Onchocerciasis
Onchocerciasis (river blindness) is a disease caused by Onchocerca volvulus. Humans are infected by repeated bites of infected blackflies, Simulium sp. Onchocerciasis occurs mainly in tropical areas and more than 99% of infected people live in 31 countries in sub-Saharan Africa (23). The disease is also found in Yemen and 5 countries in Latin America. About 123 million people are at risk of infection with O. volvulus and at least 25 million people are infected worldwide (24).
Skin lesions occur when the adult worms in the skin undergo destruction, and itching and rash are the early manifestation of skin lesions (13). Subcutaneous nodules (onchocercoma) develop through tissue reaction around the adult worms. Some infected people develop eye lesions, leading to visual impairment and permanent blindness (23). River blindness is the one of the two most common causes of blindness due to infection, together with trachoma (25). Approximately 0.8 million people experience visual impairment and 300,000 are blind due to onchocerciasis (24).
There are no vaccines or drugs to prevent infection with O. volvulus (23); therefore, the only prevention is through avoiding bites by blackflies using insect repellent and proper clothing (13). Vector control is also important in reducing the transmission of parasites to humans.
WHO recommends treating onchocerciasis with ivermectin at least once a year for about 10 to 15 yr. Efforts to eradicate the disease by treating entire groups of people twice a year with ivermectin are ongoing in endemic areas (23). Community-directed treatment with ivermectin is the core strategy in Africa, while biannual large-scale treatment with ivermectin is the strategy used in the Americas (23). The Onchocerciasis Control Programme in West Africa (OCP) was launched in 1974 (26). This program successfully protected 40 million people from infection and prevented blindness in 0.6 million people through vector control and ivermectin treatment (23). The Onchocerciasis Elimination Program of the Americas (OEPA) began in 1992 to eliminate ocular morbidity and transmission throughout the Americas by 2012. Transmission was interrupted in 10 of 13 foci in this region by the end of 2011. In 1995, the African Programme for Onchocerciasis Control (APOC) was launched for control of onchocerciasis in the remaining endemic countries in Africa. In 2010, ivermectin for nearly 76 million people was distributed in 16 APOC countries. In 2013 and after a verification process, WHO declared Colombia free of onchocerciasis. Colombia became the first country in the world to be verified and declared free of onchocerciasis by WHO (23).
Schistosomiasis
Schistosomiasis is caused by blood flukes of Schistosoma sp. and there are two major forms of schistosomiasis: intestinal (Schistosoma mansoni, S. japonicum, S. mekongi, S. intercalatum) and urogenital (S. haematobium). People are infected by exposure to cercariae of Schistosoma spp. in water during domestic, agricultural, occupational and recreational activities. The disease is especially common among children in developing countries because of inadequate hygiene and play habits such as swimming or fishing in infested water (27).
Schistosomiasis is prevalent in 78 countries in Africa, Asia and South America and about 700 million people are at risk of infection (27). It affects 210 million people worldwide and at least 90% of those requiring treatment for schistosomiasis live in Africa (27). It is prevalent in tropical and sub-tropical areas, especially in poor communities without access to safe drinking water and adequate sanitation. Chronic schistosomiasis may affect people's ability to work and in some cases can result in death. In sub-Saharan Africa, it has been estimated that schistosomiasis is the cause of more than 200,000 deaths per year (27). Schistosomiasis is second only to malaria as a cause of death by parasitic disease (28).
Symptoms are caused by immune reactions to eggs than adult worms. Intestinal schistosomiasis is shown by abdominal pain, diarrhea and blood in the stool (29). Liver enlargement and cirrhosis are common in advanced cases. The classic sign of urogenital schistosomiasis is hematuria. Fibrosis of the bladder and ureter, and kidney damage are sometimes diagnosed in advanced cases. Bladder cancer is the most serious complication in the later stages. Urogenital schistosomiasis is also considered to be a risk factor for HIV infection, especially in women (27). In children, schistosomiasis can cause anemia, poor growth, and learning difficulty, although the effects are usually reversible with treatment (27).
Schistosomiasis is diagnosed by detection of eggs in stool or urine. Children with S. haematobium almost always have microscopic blood in their urine (27). Serological tests may be useful in non-endemic or low-transmission areas. Praziquantel is the recommended drug for treatment of schistosomiasis. If treatment is initiated and repeated in childhood, the risk of developing severe disease is diminished and even reversed (27).
The control strategies of schistosomiasis include large-scale treatment of at-risk populations, access to safe water, improved sanitation, hygiene education, and snail control. The WHO strategy for schistosomiasis control focuses on reducing disease through periodic, targeted treatment with praziquantel (preventive chemotherapy) (27). Preventive chemotherapy for schistosomiasis is only required in 52 endemic countries with moderate to high transmission and the frequency of treatment is determined by the prevalence of infection in school-age children (27). In high transmission areas, treatment may have to be repeated annually for a number of years and the impact of interventions should be monitored. However, the availability of praziquantel is a major limiting factor for schistosomiasis control. At least 249 million people required preventive treatment in 2012, but 31 countries received preventive chemotherapy and only 14.4% of people requiring treatment were reached in 2012 (27).
Schistosomiasis control has been successfully implemented over the past 40 yr in several countries, including Brazil, Cambodia, China, Egypt, Mauritius and Saudi Arabia (27). There is evidence that schistosomiasis transmission was interrupted in Morocco. In Burkina Faso, Niger, and Yemen, it was possible to scale up schistosomiasis treatment to the national level and this has had an impact on the disease in a few years.
Korean parasitologists have been contributing to control activities for schistosomiasis in Sudan and Tanzania since 2005 by the support of KOICA and Good Neighbors respectively (89). The project on schistosomiasis in Sudan included comprehensive approach to lower the prevalence of genitourinary schistosomiasis by MDA, health education, and filtered water supply (Fig. 1) (30). By the experience, the prevalence of urogenital schistosomiasis was reduced to half of baseline a year after praziquantel administration; however, the comprehensive approach was more effective than praziquantel therapy only (30). Also, the project faced serious shortage of budget for water supply system due to national economic crisis and high inflation. The budget shortage was overcome by the community leaders' efforts pushing and persuading their local government. The project is a recent successful model of NTDs control by self-support of the infected community people in Sudan (30).
Dracunculiasis (Guinea worm disease)
Dracunculiasis is an infection by the guinea worm, Dracunculus medinensis and is called guinea worm disease. Humans are infected exclusively by drinking water contaminated with infected water fleas (Cyclops). The infected person has no clinical symptoms until a painful blister forms in the skin, usually on the lower leg, a year after exposure to infection. The person experiences burning feeling as the female worm comes out of the skin in over a few weeks (31), and becomes crippling for months. A diagnosis of the disease can usually be made based on the signs and symptoms of the disease (13).
There are no vaccines or drugs to treat the disease (32). Because humans are the principal host for D. medinensis, identifying and treating all cases as well as modifying human behavior can control the disease (32). Other efforts include an improving access to clean water or filtered water through a cloth if it is not clean (3132). Contaminated drinking water may be treated with a chemical called temefos to kill the larva (32).
The Centers for Disease Control and Prevention (CDC) of USA began the global campaign to eradicate Guinea worm disease in 1980, and the Carter Center, in conjunction with CDC, UNICEF, and WHO, has been in the forefront of the global campaign since 1986 (32). During the mid-1980s, 3.5 million cases were reported in 20 countries worldwide, including India, Pakistan, Yemen and 17 countries in Africa (32). However, as a result of eradication activities, the annual incidence of the disease in 2013 has dramatically decreased by more than 99% compared to the mid-1980s. Among 20 countries, only 4 countries in Africa, Chad, Ethiopia, Mali and South Sudan, are endemic and 148 cases were reported in 2013, most of which occurred in South Sudan (3233). Therefore, dracunculiasis will likely be the first promising parasitic disease to be eradicated.
Visceral leishmaniasis
Visceral leishmaniasis (VL or kala-azar) is caused by two causative agents, namely Leishmania donovani and Leishmania infantum and is characterized by irregular fever, weight loss, enlargement of the spleen and liver, and anemia. Leishmaniasis is transmitted through phlebotomine sandflies. L. donovani infections are restricted to the (sub-)tropics of Asia and Africa while L. infantum occurs in the drier parts of Latin America as well as in the Mediterranean climate regions of the Old World, with domestic dogs serving as the main reservoir host (34). The prevalence of VL caused by L. infantum has been declining where living standards have improved. In contrast, infections of L. donovani continue to cause VL epidemics in Indian subcontinent and in East Africa (35). An estimated 200,000 to 400,000 new cases of VL occur worldwide each year. In East Africa and on the Indian subcontinent, where up to 50% and 5%-10% of patients with kala-azar, respectively, develop the Post kala-azar dermal leishmaniasis (PKDL) (34).
Leishmaniasis is a treatable and curable disease, thus prompt and complete treatment is important. AmBisome (Gilead, Foster, CA, USA), a liposome formulation of amphotericin B, is now a standard treatment for VL (35) (http://www.who.int/tdr/news/2013). However, there is a resistant strain, L. donovani, in some areas. Drug combinations can shorten therapy as well as reducing toxicities. There have been some promising Phase III trials of combinations of AmBisome, miltefosine, and paromomycin in India and of sodium stibogluconate with paromomycin in Sudan (3536).
The first human case reported in the Republic of Korea was by Heu in 1952 with 3 cases of VL among returnees from northern China (37). Thereafter, two more imported cases of VL were reported; one from a man returning from Saudi Arabia (38) and another from a one-year old girl who traveled to Argentina (3940). Recently, the first autochthonous case of canine leishmaniasis was reported (41). This finding suggested that there is a possibility of presence of indigenous human VL in Korea as well. It is necessary to pay attention to this neglected disease in Korea in the future.
Chagas disease
Chagas disease (American trypanosomiasis) is caused by the protozoan parasite, Trypanosoma cruzi and transmitted by triatomine bugs, known as 'kissing bugs'. They usually bite an exposed area of the skin, and the bug defecates close to the bite. The parasites in the feces enter the body through any skin break when the person instinctively smears the bug feces (42). About 8 million people are estimated to be infected worldwide, mostly in Latin America. Persons can rarely be infected through blood transfusion, congenital transmission, and organ transplantation.
Clinically, there are two phases in Chagas disease. In the initial, acute phase (about 2 months after infection), a number of parasites circulate in the blood and generally, symptoms are absent or mild. Fever, headache, enlarged lymph glands, pallor, muscle pain, difficulty in breathing, swelling and abdominal or chest pain are all common symptoms. A purplish swelling of the lids of one eye can be a characteristic first visible sign. During the chronic phase, the parasites are hidden mainly in the heart and digestive muscle. Up to 30% of patients suffer from cardiac disorders and up to 10% suffer from digestive symptom (typically enlargement of the esophagus or colon). The infection can lead to sudden death or heart failure caused by progressive destruction of the heart muscle in late stage (42).
Chagas disease can be treated with benzmidazole and nifurtimox. Both medicines are almost 100% effective in the acute phase. However, the efficacy of both diminishes at chronic phase. There is no vaccine for Chagas disease. Vector control is the most effective method of prevention in Latin America. Blood screening is necessary to prevent infection through transfusion and organ transplantation. Since the 1990s, there have been important successes in parasite and vector control in Latin America; yet, there are still some challenges in preventing the spreading of the disease mainly due to increasing population mobility between Latin America and the rest of the world (42). Chagas disease has not been reported in Korea yet, it is necessary to pay attention to this neglected disease due to the increasing number of visitors to Latin America these days.
Human African trypanosomiasis
Human African trypanosomiasis (HAT, sleeping sickness) is caused by protozoan parasites belonging to the genus Trypanosoma and transmitted by tsetse fly (Glossina genus). Tsetse flies are just found in sub-Saharan Africa (43).
Currently, over 98% of reported cases of sleeping sickness are caused by Trypanosoma brucei gambiense and 2% are by another species, T. brucei rhodesiense. T. b. gambiense is found in 24 countries in west and central Africa and causes chronic infection, whereas T. b. rhodesiense causing an acute infection is reported in 13 countries eastern and southern Africa. Only Uganda is present with both forms of the disease. Animals can host T. b. rhodesiense as well as T. b. gambiense, thus domestic and wild animals are important parasite reservoirs. Its prevalence has grown to an estimated 300,000 cases by 1998 from a position of near control in the 1960s (4445). Now, there is a steady decline in incidence by enhanced surveillance, distribution of free drugs and implementation of several clinical trials. According to the efforts, there is a hope of elimination by 2020 (36).
Clinically, in the first stage, the trypanosomes multiply in the subcutaneous tissues, blood and lymph. This stage induces fever, headache, joint pains and itching. In the second stage the parasites cross the blood-brain barrier to infect the central nervous system. In this neurological phase, changes in behavior, confusion, sensory disturbances and poor coordination appear. Disturbance of the sleep cycle is an important feature in this stage. A person can be infected for months or years without major signs or symptoms of the disease in the case of T. b. gambiense infection. When more evident symptoms emerge, the patient is often already in an advanced disease stage where the central nervous system is affected (43).
Serological tests and checking for clinical signs - generally swollen cervical glands are useful for screening the infection. Examining cerebrospinal fluid obtained by lumbar puncture is also used to determine stage and the outcome of treatment.
Current drugs for HAT are unsatisfactory due to varying degrees of toxicity, a need for parenteral administration and resistance (36). Pentamidine is used for the first stage of T. b. gambiense sleeping sickness and suramin for T. b. rhodesiense. These drugs have lower toxicity and are easier to administer. Drugs for second stage are toxic and complicated to administer because they should be able to cross the blood-brain barrier to reach the parasite. Four drugs are registered for the treatment of sleeping sickness. Melarsoprol is used in both forms of infection, but it has many undesirable side effects. Eflornithine is less toxic than melarsoprol, but only effective against T. b. gambiense. A combination treatment of nifurtimox and eflornithine has been accepted and included in the WHO List of Essential Medicine (43).
The emergence of Product Development Partnerships including the Geneva-based Drugs for Neglected Diseases initiative (DNDi) and the US-based Consortium for Parasitic Drug Development and Institute for One World Health (IoWH) provided formats to enable progression of compounds through clinical trials thus filling a gap created by the abandonment of these areas by the Pharmaceutical industry (36).
CONCLUSION
NTDs are neglected diseases of neglected people, which form a vicious cycle of disease and poverty. It is definite and essential to break the vicious cycle by giving priority to the neglected people and NTDs. Although resources are limited, implementing sustainable national programs is a key for the control of NTDs. Fortunately, more resources and programs are allocated for NTDs recently than before, which may give more chances to the neglected people who are actively seeking to overcome NTDs. No more self-neglect is the beginning to eliminating the diseases and upgrading the quality of life of the neglected people.

 XML Download
XML Download