

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Respiratory syncytial virus (RSV) is the most common virus of causing lower respiratory tract infections in infants (12) and accounts for 74.8% of admissions for bronchiolitis (3). Although infections caused by RSV usually have a mild and self-limiting course, it can be severe enough to require hospital admission of high risk infants. Bronchopulmonary dysplasia (BPD), congenital heart disease, and premature birth are known risk factors for complications from an RSV infection, such as hospital admission, need for intensive care, and a poor prognosis (45).
The monoclonal antibody, palivizumab (Synagis®; MedImmune LLC, Gaithersburg, MD, USA) is currently being used for prophylaxis of severe RSV infection in preterm infants (67). Palivizumab is also indicated in Korean infants who are diagnosed with BPD within 6 months and are < 2 yr of age, or are born at < 32 weeks' gestation and < 6 months of age at the beginning of the RSV season.
Several reports have been published on readmission of preterm infants with RSV in Korea (8910). However, they were not multicenter-based studies or did not evaluate the effect of palivizumab prophylaxis on the readmission with RSV in Korea.
Hence, the aim of this study was to evaluate the rate of RSV related readmissions (RRR) and risk factors in preterm infants less than 34 weeks gestational age (GA) within 1 yr following discharge from the neonatal intensive care unit (NICU) in Korea.
MATERIALS AND METHODS
This study was performed as part of a project "Retrospective Study to Evaluate Rehospitalization & Health Care Utilization after NICU Discharge in Preterm Infants (less than 34 weeks' gestation) II" (RHANPI II) conducted by the Committee on Data Collection and Statistical Analysis of the Korean Society of Neonatology.
Patient population
The cohort of RHANPI II included all preterm infants less than 34 weeks' gestation who were born and survived to discharge at the NICUs of 46 hospitals in Korea from April 2012 to September 2012 (n=1,867). The overall readmission rate of this cohort was 28.4% after discharge from the NICU. Out of the cohort, the infants who were followed up for >1 yr after discharge from the NICU, or who were readmitted after discharge from the NICU were enrolled in this study (n=1,140) (Fig. 1).
Data collection
The Committee on Data Collection and Statistical Analysis of the Korean Society of Neonatology chose the 46 Korean NICUs. The data were collected by the neonatologists of the 46 NICUs retrospectively through chart review based on standard study formats accompanied with a manual defining the variables. All data were entered electronically into a central database during the study period from January to March 2014. The data were checked repeatedly for quality and completeness. Missing information or errors were returned to the neonatologists to verify the data. We modified the database of RHANPI I that was created in collaboration with the Clinical Research Center of Samsung Medical Center, which used the Oracle Korea electronic case reporting system (Oracle corp., Seoul, Korea). The data included perinatal and neonatal characteristics such as major morbidities in the NICU, and data obtained at readmission including the cause for the readmission, need for oxygen supplementation, need for ventilator support, and need for intensive care. Readmission included the events of readmission in each hospital or another hospital stated in the medical records.
Definitions of variables
BPD was defined as the need for supplemental oxygen for at least 28 days after birth and severity was graded according to the respiratory support required at 36 postmenstrual weeks or discharge, whichever came first (11). Necrotizing enterocolitis was defined as Bell's stage II or greater (12). Stage III or IV intraventricular hemorrhage (13) and cystic periventricular leukomalacia on a cranial ultrasonogram based on the Papile grading system. Sepsis was defined according to the Centers for Disease Control and Prevention/National Nosocomial Infection Surveillance definitions for infants ≤12 months (14). Palivizumab prophylaxis was defined as to whether the protective effects of injecting palivizumab were noted at the time of RRR.
Statistical analysis
Statistical analysis for readmission rate including RRR, Comparison of RRR based on GA, and risk factors for RRR were performed targeting all infants (n=1,140) and infants who were diagnosed with BPD which is a well-known high risk morbidity (n=326). Categorical data are presented as numbers (%), and continuous data are presented as the mean±standard deviation. The cumulative probability of first RRR was calculated with the Kaplan-Meier product limit method and the trend for rate of RRR according to categorized GA was estimated with the log-rank test. The multivariable logistic regression was used for assessing association between risk factor and the RRR following discharge from the NICU. The risk factors were selected for adjusting potential confounding effects of clinically plausible and statistically reasonable covariates (GA, birth weight, elder siblings, BPD, palivizumab prophylaxis). To compare RRR and analyze risk factors of RRR based on GA, subgroups were categorized as; 25 weeks' gestation or less, 26-27 weeks' gestation, 28-29 weeks' gestation, 30-31 weeks' gestation, and 32-33 weeks' gestation. All statistical tests were two-sided and P<0.05 was considered significant. Data was analyzed with SAS software ver. 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Characteristics of study population
Mean weeks of GA for all infants (n=1,140) was 30+5±2+5 weeks, and mean birth weight was 1,502±474 g. Of all infants that include eight infants whose data on BPD were unavailable, 28.6% (326/1,140) were diagnosed with BPD in the NICU. Mean weeks of GA for the infants with BPD (n=326) was 27+6±2+3 weeks and mean birth weight was 1,069±324 g. The perinatal and familial characteristics and major outcomes of enrolled infants in the NICU are shown in Tables 1 and 2. A total of 47.5% of the infants and 89.3% of the infants with BPD were put on a course of palivzumab.
Overall readmission, respiratory readmission, and RSV related readmission
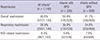
Out of all infants (n=1,140), 531 (46.6%) experienced overall readmission. Three hundred thirty (28.9%) experienced respiratory readmission that accounted for 58.8% of the infants who experienced overall readmission. Ninety-six infants (8.4%) experienced RRR that accounted for 29.1% of the infants who experienced respiratory readmission.
Out of the infants with BPD (n=326), 195 (59.8%) experienced overall readmission. 130 (39.9%) experienced respiratory readmission that accounted for 66.7% of the infants who experienced overall readmission. Thirty-two infants (9.8%) experienced RRR that accounted for 24.6% of the infants who experienced respiratory readmission. A summary of the readmission rates following discharge from the NICU is shown in Table 3.
Out of the infants who experienced respiratory readmission, 50% had laboratory tests for confirming etiological viruses. RSV accounted for 58.2% of respiratory readmissions of infants who had laboratory tests for confirming etiological viruses.
The mean frequency of RRR in all infants was 1.0±0.1. Intensive care was required for 15.5% of the infants with RRR, and ventilator support was required for 6.2% of the infants with RRR.
Comparison of RSV related readmission based on GA
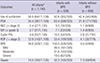
No significant difference in RRR was observed when the GA was divided into five groups in all infants (P=0.159, Log-rank test for trend) (Fig. 2A) and in the infants with BPD (P=0.445, Log-rank test for trend) (Fig. 2B). The rates of RRR and 95% confidence intervals at the time-points after discharge from the NICU are shown in Table 4.
Risk factor of RSV related readmission
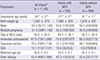
Compared with the infants 25 or less weeks' gestation, the infants 32-33 weeks' gestation had a decreased risk of RRR (odd ratio, [OR], 0.11; 95% confidence interval [CI], 0.02-0.53; P=0.006) but the infants 26-31 weeks' gestation did not differ in the risk of RRR. Compared with the infants who were not diagnosed with BPD, the infants with BPD had an increased risk of RRR (OR, 2.95; 95% CI, 1.44-6.04; P=0.003). Living with elder siblings increased the risk of RRR (OR, 2.68; 95% CI, 1.68-4.28; P<0.001); however palvizumab prophylaxis decreased the risk of RRR (OR, 0.06; 95% CI, 0.03-0.13; P<0.001) (Table 5).
In an analysis of infants with BPD, living with elder siblings increased the risk of RRR (OR, 5.82; 95% CI, 1.95-17.32; P=0.002); however, palivizumab prophylaxis decreased the risk of RRR (OR, 0.03; 95% CI, 0.01-0.008; P<0.001). GA, birth weight, and severity of BPD did not influence the risk of RRR (Table 5).
DISCUSSION
In this study, 8.4% of preterm infants less than 34 weeks' gestation were readmitted with an RSV infection within 1 yr following discharge from the NICU. Living with elder siblings or BPD increased the risk of RRR but birth at 32-33 weeks' gestation (vs. birth at <26 weeks' gestation) or palivizumab prophylaxis significantly decreased the risk of RRR.
RRR of preterm infants in previous studies varied considerably (151617). Resch et al. (18) analyzed 18 previous studies and reported the mean RRR rate of 9.3% in preterm infants without BPD. The rate of RRR of preterm infants was 3.1%-9.3% in Korean studies (89101920). The rate of RRR of this study was 8.4% and was similar with other Korean studies. The variations in the readmission rates among these studies may be due to seasonal fluctuations in RSV infection, RSV virulence, compliance to palivizumab prophylaxis or variable indications of laboratory tests for diagnosing RSV infection during admission. In this study, only 50% of infants who were readmitted with respiratory problems had laboratory tests done for diagnosing RSV infection during their readmission. Paes et al. (21) reported that 20.9% of preterm infants who had laboratory tests for RSV during their readmission were diagnosed with RSV infection. In this study, 58.2% of preterm infants who had laboratory tests for RSV infection were confirmed to have an RSV infection. The difference between Paes's and this study may be due to because in this study, laboratory tests were done mainly on infants who presented with a more serious condition.
In this study, 46.6% of enrolled infants experienced overall readmission, 28.9% were readmitted due to respiratory problems, and 8.4% experienced RRR. These rates of readmission may seem to be higher than previous studies (891019222324). However, if the infants (N=727), who dropped out from this study were included in readmission calculation, the rates of overall readmission, respiratory readmission, and RRR would have been 28.4%, 17.7%, and 5.1%, respectively, and these rates of readmission would have been comparable with previous studies.
Prematurity is a known risk factor of RRR (2526). The risk results from characteristics of their lung, such as a small lung volume, a reduced lung surface area, small airway and increased air space wall thickness (27). In addition, they have insufficient humoral and cellular immunity to clear viral load (28). Carbonell-Estrany et al. (29) reported that the risk of RRR decreased with older GA (OR, 0.85; 95% CI, 0.72-0.99; P=0.047). Joffe et al. (16) reported that infants 23 to 32 weeks' gestation were at greater risk of RRR than those 33-36 weeks' gestation (OR 2.6; 95% CI, 1.4-5; P=0.003). In contrast, GA was not a significant independent risk factor of RRR in the study of Paes et al. (21). In this study, there was no significant difference of RRR among the infants according to categorized GA except the comparison between infants <26 weeks' gestation and infants 32-33 weeks' gestation. The differences among these studies may be due to differences in the enrolled study population or grouping of categorized GA.
Resch et al. (18) reported that the rate of RRR of infants with BPD was 19.8% in the analysis of eight studies of RRR. Since the Impact-RSV (5), many studies have reiterated that BPD is a risk factor of RRR. Carbonell-Estrany et al. (2) reported that BPD was an independent risk factor of RRR in study populations who were born at <33 weeks' gestation (OR, 1.86; 95% CI, 1.22-7.91; P=0.048). This study also showed a similarity in analysis between the RRR and BPD with previous studies.
In a subgroup analysis, 9.8% of infants with BPD were readmitted with RSV and 89.1% of them were administered with palivizumab. Additionally, living with elder siblings increased the risk of RRR; however, palivizumab prophylaxis decreased the risk of RRR, significantly. GA at birth, birth weight, and BPD severity did not influence the risk of RRR in infants with BPD. Chang et al. (9) reported that the rate of RRR was 12.6% in infants with BPD who were not administered with palivizumab and 4.0% in infants with BPD who were administered with palivizumab in a single center study in Korea. Lacaze-Masmonteil et al. (30) reported that the rate of RRR was 8.1% in a French cohort study where 81% of infants were diagnosed with BPD. Palivizumab prophylaxis reduced the rate of RRR in infants with BPD from 12.8% to 7.9% in Impact-RSV Study (5).
Paes's et al. (21) reported that infants who lived with siblings had a higher risk of RRR than infants who did not (hazard ratio 2.1; 95% CI, 1.4-3.3; P<0.001). In this study, living with elder siblings was also an independent risk factor of RRR. This study was conducted in a retrospective design that aimed at preterm infants during one RSV season which may be a limitation to represent the epidemiological characteristics associated with RRR in Korea.
The main outcome of this study is that it is the first multicenter-based, nation-wide study to evaluate the readmission rate and associated risk factors of RSV in preterm infants less than 34 weeks' gestation within 1 yr following discharge from the NICU in Korea. This study suggests that preterm infants with BPD or those living with siblings should be supervised closely and considered for administration of palivizumab to prevent RRR following discharge from the NICU.




 XML Download
XML Download