

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Active surveillance (AS) is an emerging treatment strategy for low-risk prostate cancer (PCa) in response to high rates of over-diagnosis using prostate-specific antigen (PSA) levels as a biomarker (1, 2). AS programs are designed to identify patients with clinically indolent tumors and to avoid or delay definitive treatment in these men (3, 4). While AS appears to be a reasonable approach for insignificant tumors, its widespread acceptance remains limited by a lack of consensus in defining appropriate candidates (5). Inclusion criteria for currently used AS guidelines are usually based on the maximum Gleason score, PSA levels and/or PSA density, clinical stage, number of positive biopsy cores, and percentage of single core involvement (6, 7). Currently, various criteria predicting potentially insignificant disease have attempted to strike a balance between maximizing the number of patients who can avoid treatment and minimizing the number of aggressive cases (3, 4, 8, 9). While considerable effort has been devoted to identifying an optimal AS criteria in a clinical practice, adverse pathological features at radical prostatectomy have been reported in 11%-33.5% of potential candidates for AS (10, 11). In addition, most of AS studies do not yet have emphasized the risk of unintended exclusion of actual insignificant PCa. To address these questions, we compared the discriminative performance of contemporary AS criteria to determine whether contemporary AS protocols could sufficiently discriminate clinically significant from indolent tumors in a cohort of low-risk PCa. Specifically, we also assessed the clinical and biopsy characteristics of pathologically insignificant PCa patients who are not eligible for any criteria of published AS protocols.
MATERIALS AND METHODS
Study design
We retrospectively analyzed 312 patients with low-risk PCa treated with radical prostatectomy by a single surgeon at Severance Hospital between January 2007 and December 2013. Low-risk PCa was defined as clinical stage T1c/T2a, PSA levels of 10 ng/mL or less, and a Gleason score of 6 or less on a multi-core biopsy according to the D'Amico classification. After exclusion of patients with fewer than 10 cores taken at biopsy and who received neo-adjuvant treatment, 205 subjects satisfied the final inclusion criteria. We identified patients' eligibility for the inclusion criteria using five AS protocols: Johns Hopkins Medical Institution (JHMI) (12), Memorial Sloan-Kettering Cancer Center (MSKCC) (13), Prostate Cancer Research International Active Surveillance (PRIAS) (14), University of California, San Francisco (UCSF) (15), and University of Miami (UM) (16). Adverse findings were Gleason score upgrade (score 7 or greater) and non-organ-confined cancer on surgical pathology. Pathologically insignificant PCa was defined as being organ-confined with a Gleason score less than or equal to 6 (no Gleason pattern 4/5) and a tumor volume less than 0.5 cm3 (8).
Statistical analysis
Continuous variables are shown as the median and interquartile range (IQR). The sensitivity, specificity, and accuracy of pathologically insignificant PCa predictions between each AS criteria were compared. Sensitivities, specificities, and diagnostic accuracy were calculated using standard formulas: sensitivity= TP/TP+FN; specificity=TN/TN+FP; and accuracy=TP+TN/TP+TN+FP+FN, where TP is the number of true positives, TN is the number of true negatives, FP is the number of false positives, and FN is the number of false negatives. Analysis was performed using SPSS 20.0 software (SPSS Inc., Chicago, IL, USA).
Ethics statement
The study was carried out in agreement with applicable laws and regulations, good clinical practices, and ethical principles as described in the Declaration of Helsinki. The institutional review board of Severance Hospital approved the present study protocol (Approval number: 4-2014-0619).
RESULTS
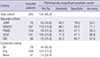
Table 1 summarizes the baseline characteristics of the 205 low-risk PCa patients included in the analysis. The median prebiopsy PSA and prostate-specific antigen density were 5.4 ng/mL (IQR 4.3-6.9 ng/mL) and 0.16 ng/mL/g (IQR 0.11-0.23 ng/mL/g), respectively. The majority of men had a biopsy Gleason score of 6 and clinical T1c or T2a disease at the time of diagnosis.
After radical prostatectomy, 61 (29.8%) patients had their disease upgraded in the prostatectomy specimen (5 were upgraded to a Gleason score of 6, 50 were upgraded to a Gleason score of 3+4, 4 were upgraded to a Gleason score of 4+3, and 2 were upgraded to a Gleason score of 8) and 26 (12.7%) had non-organ-confined disease (Table 2). The rates of adverse pathology in patients who qualified for each AS protocol are listed in Table 3. A total of 82% of the patients fulfilled the inclusion criteria of at least one protocol, whereas 18% did not meet any criteria of contemporary five AS protocols. The JHMI protocol was the most stringent, with only 34.1% of the patients fulfilling the JHMI criteria, whereas the MSKCC protocol was the most lenient, with 78.5% of the patients fulfilling the MSKCC criteria. For the PRIAS, UCSF, and UM criteria, 53.2%, 68.8%, and 46.8% of patients fulfilled these criteria, respectively. Non-organ-confined disease was found in 8.6% to 10.6% of patients, and a Gleason score of 7 or greater disease was found in 18.6% to 23.9% of patients according to the five AS protocols.
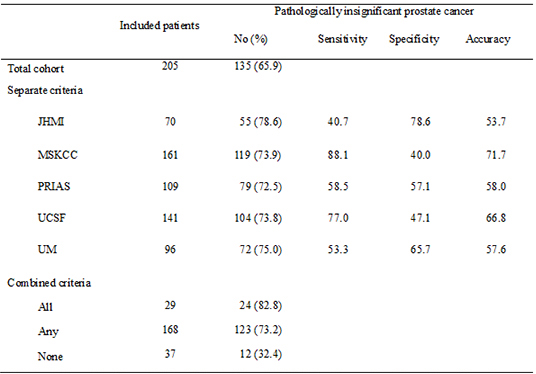
Overall, 135 patients (65.9%) had pathologically insignificant PCa. The abilities of each AS protocols to predict pathologically insignificant PCa are described in Table 4. The JHMI protocol showed the highest specificity but lowest sensitivity, whereas the MSKCC protocol showed the highest sensitivity but lowest specificity. Among patients who did not meet any criteria of contemporary five AS protocols, 12 (32.4%) patients had pathologically insignificant cancer (Table 5). There were no significant clinical and biopsy characteristics, which can discriminate pathologically significant from insignificant tumors in a cohort of 12 patients who are not eligible for any criteria of contemporary five AS protocols (data not shown). During the median follow up of 47 (IQR: 25-72) months, only six patients (2.9%) had a biochemical recurrence. There was no case of cancer-specific death.
DISCUSSION
The present study investigated the pathologic outcomes in men with low-risk PCa who were potential candidates for contemporary AS protocols. Significant adverse pathology was identified in patients deemed eligible for contemporary AS protocols, but also some patients in whom expectant management would be appropriate are not eligible for any criteria of contemporary five AS protocols. Our results suggest the limited value of currently obtained histological criteria to appropriately select candidates for AS.
Currently, many different criteria of AS protocols are in use, ranging from stringent exclusive criteria to less stringent inclusive criteria (6). Given the current status of numerous AS guidelines with no uniformly accepted standard, no current criteria sufficiently discriminate clinically significant from indolent tumors. Several retrospective studies have emphasized the risk of under-diagnosis (17, 18, 19, 20). Even with the most stringent selection criteria, it may be difficult to perfectly differentiate between clinically insignificant and life-threatening PCa (10, 21). Several authors have analyzed the pathologic features of surgical specimens in patients who qualified for different criteria of AS protocols. The discriminative ability of contemporary AS protocols showed significant variation across different institutions (8, 11, 22, 23, 24). In a recent study by Iremashvili al., five AS protocols were compared with regard to discriminative ability to predict three pathologic end points in a 391 radical prostatectomy cases. In this study, PRIAS and UM have demonstrated the highest ability to identify patients with insignificant prostate cancer (8). Lee et al. also compared the discriminative ability of five AS protocols and concluded that the PRIAS had the best balance between sensitivity, specificity and the diagnostic accuracy (11). Our results were similar to those described in previous studies in which significant variations exist in the ability of contemporary AS protocols to predict pathologically insignificant PCa. While numerous investigators described the ability of contemporary AS protocols to predict pathologically insignificant PCa, little is known about the possible exclusion of actual insignificant PCa. Interestingly, 32.4% of patients who did not meet any AS criteria contemporary AS protocols had a pathologically insignificant cancer. These results suggested that none of the currently used clinical or histological criteria have a sufficient sensitivity or specificity for the appropriate selection of candidates for AS (25). Consequently, there is a great needs for novel tools such as repeat biopsy, multi-parametric magnetic resonance imaging and various blood markers (PSA isoform/kinetics), or others to blend into selection criteria on active surveillance for low-risk prostate cancer.
Our study has both limitations and strengths. It had a retrospective design, which may have introduced some sampling bias. In addition, our study cohorts were consisted of low-risk PCa according to the D'Amico classification, which could be a confounding factor affecting discriminative performance. Therefore, our results should be viewed as a comprehensive consideration of contemporary AS criteria. On the other hand, our data originated from a single institution and a single surgeon, which minimizing performance variability and bias.
In conclusion, significant adverse pathology was identified in patients deemed eligible for contemporary AS criteria. On the other hand, some patients in whom expectant management would be appropriate did not meet any AS criteria. These findings suggest that none of the clinical or histological criteria reported to date is able to sufficiently discriminate aggressive tumors from indolent ones.
 XML Download
XML Download