

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common clinically significant arrhythmia in clinical practice. AF is associated with increased morbidity and mortality that primarily occur as a result of complications, such as thromboembolic events and heart failure (1, 2).
In clinical practice, one should distinguish between the AF clinical types: paroxysmal AF (PAF): episodes of the arrhythmia that terminate spontaneously; persistent AF (PeAF): episodes that are sustained 7 days or more and are not self-terminating; permanent AF: ongoing long-term episodes (3), which will affect the individual treatment strategy for each patient (4).
AF usually starts as PAF and transforms into PeAF (5). The mechanism of PAF consists of initiating factors. The role of the maintenance factors is less important, but becomes more important in association with progression of AF to PeAF or permanent AF (6, 7). This seems particularly to be a concern in patients with PeAF or permanent AF, whose higher incidence of events from cardiac and non-cardiac origins can affect long-term outcomes (8).
In previous studies, Canadian Registry of Atrial Fibrillation (CARAF) investigators found that underlying heart disease and age were independently associated with progression of AF.
The Euro Heart Survey (EHS) on AF presents a unique overview of AF management in a large group of patients in several European countries (4, 9, 10). Significant interest also has been directed to factors predicting the progression of PAF to PeAF or permanent AF. Recently, the HATCH score, which is an acronym for hypertension, age ≥ 75 yr, transient ischemic attack (TIA) or stroke (2 points), chronic obstructive pulmonary disease (COPD) and heart failure (2 points), was proposed as a simple clinical tool to identify patients who are likely to progress PeAF or permanent AF (4, 11). However, available data on the progression rate of PAF to PeAF or permanent AF and predictors for progression are relatively limited in Korean populations.
The aim of this study was to evaluate the prognosis of patients with AF progression and validate a risk stratification to assess the probability of AF progression in Korean populations.
MATERIALS AND METHODS
Study populations
In our study, total 2,413 patients with AF were reviewed for 18 yr. The patients were excluded if they had one of the following conditions; including a recent history of acute infection or inflammatory disease, age >80 yr old, a history of cardiomyopathy, or valvular (defined as ≥moderate mitral regurgitation, aortic regurgitation, aortic stenosis or a presence of prosthetic heart valve or history of repair) or congenital heart disease, hepatic or renal disease, an acute cardiovascular or cerebrovascular event within the preceding 3 months, any major trauma or surgery within the preceding 3 months, hyperthyroidism, uncontrolled hypertension, malignancy, connective tissue disease, or any acute or chronic inflammatory disease.
Finally, a total 434 patients with PAF were enrolled and we retrospectively analyzed those 434 non-valvular PAF patients (mean age: 71.7±10.7 yr, 60.6% male) consecutively. Patients with a history of PAF documented by a standard electrocardiogram (ECG) or Holter-ECG were enrolled. The flow chart is shown in Fig. 1. The baseline characteristics of the patients are presented in Table 1.
Data collection
After ECG and chest radiograph, cardiovascular status was evaluated for each patient using echocardiography, an exercise test, 24-hr Holter recordings, and blood laboratory data from the initial visit, as determined by the attending physicians. From the database, the following information was collected: 1) patient data, including sex, age, height, and weight; 2) cardiovascular risk factors, including hypertension (use of antihypertensive agents, systolic blood pressure ≥140 mmHg, or diastolic blood pressure 90 mmHg on admission) and diabetes mellitus (use of oral hypoglycemic agents or insulin, or glycosylated hemoglobin ≥6.5%); 3) cardiovascular disease status, including structural heart disease, congestive heart failure, or a history of a disabling cerebral infarction or TIA; and 4) use of medication. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters.
Definitions of atrial fibrillation, atrial arrhythmia, and clinical events
In the present study, paroxysmal AF at the initial visit was defined as sinus rhythm on ECG and previous diagnosis of paroxysmal AF by referring physicians. Patients whose AF was estimated to continue for ≥7 days after the initial visit were considered to have persistent AF originally and were excluded from the analysis. Permanent AF was defined as an ongoing long-term episode. Asymptomatic AF was defined as AF documented on 12-lead ECG during a visit, in the absence of any new symptoms such as palpitations, tachycardia, fatigue, malaise, shortness of breath on exertion, dyspnea, chest pain, syncope, or pre-syncope related to AF or other illnesses. During the follow-up period, the onset of persistent AF was defined as the first time in which all ECGs indicated AF after ≥3 consecutive ECGs at intervals of ≥1 week after the initial examination, and permanent AF was defined as AF that was present for at least 6 months without intervening spontaneous episodes of sinus rhythm for which cardioversion was unsuccessful and subsequently not attempted (12). When an ECG could not be obtained thrice during the period, the physicians made a clinical judgment regarding the onset time of AF progression. When electrical cardioversion was performed after >7 days from AF onset, it was also considered as AF progression. We calculated the CHADS2score (congestive heart failure, hypertension, age [≥75 yr], diabetes mellitus, and history of stroke or TIA; 2 points). The CHA2DS2-VASc score was also determined, which also includes vascular disease (previous myocardial infarction, complex aortic plaque, and peripheral artery disease [PAD]), age 65-74 (13, 14). Atrial arrhythmia during follow-up was assumed based on recurrence of any symptoms ECG showing atrial premature complex, atrial tachycardia, or atrial flutter.
Re-admission was defined as any hospitalization of cardiac causes including AF symptoms related admission, embolic events, anticoagulation, others (percutaneous coronary intervention, coronary angiogram, permanent pacemaker insertion, etc.).
Definition of HATCH score
The HATCH score has been proposed as predictive of AF progression in pharmacologically treated AF patients (4). The HATCH acronym stands for hypertension (1 point), age ≥75 yr (1 point), transient ischemic attack or stroke (2 points), chronic obstructive pulmonary disease (1 point), and heart failure (2 points).
Transthoracic echocardiography
All enrolled subjects underwent 2-dimensional transthoracic echocardiography (TTE). All examinations were performed using a commercially available Vivid 7™ (GE Medical System, Vingmed, Horten, Norway) ultrasound system. All recorded echocardiograms were measured and interpreted with clinical information blinded using a computerized off-line analysis station (Echopac™ 6.3.4; GE Medical System).
All measurements were derived from 3 consecutive cardiac cycles and averaged. The left ventricular (LV) dimensions, wall thicknesses and left atrial dimensions (LAD) were determined in the parasternal long-axis view with the M-mode cursor positioned just beyond the mitral leaflet tips perpendicular to the long axis of the ventricle according to the recommendations of the American Society of Echocardiography (15). The LV ejection fraction (LVEF) was obtained via the modified biplane Simpson method from the apical 4- and 2-chamber views.
Statistical analysis
All continuous variables are expressed as either mean±standard deviation (SD) or median (25th, 75th interquartile range), depending on the distribution. For continuous data, statistical differences were evaluated using Student's t-test or the Mann-Whitney U test, depending on the data distribution. Categorical variables are presented as frequencies (percent) and were analyzed using the chi-square test. To determine whether any of the variables were independently related to early recurrence of AF, a multivariate analysis of variables with a P value<0.05 in the univariate analysis was performed using linear logistic regression analysis. All correlations were calculated using Spearman's rank correlation test. All statistical analyses were conducted using SPSS statistical software, version 19.0 (SPSS Inc., Chicago, IL, USA), and statistical significance was set at P<0.05 (two-sided).
RESULTS
The baseline demographics for both groups are listed in Table 1. This study consisted of 168 subjects with progression to PeAF or permanent AF and 253 subjects without AF progression. Baseline characteristics were not statistically different between the AF progression subjects and the non-AF progression subjects, except for age at diagnosis (P=0.019), BMI (P=0.042), and amiodarone medications (P=0.010). In our study, there was no difference in HATCH scores between the groups (P=0.537), which is known as a modest predictor of progression to sustained AF (4).
Table 2 shows the laboratory and echocardiographic findings in patients with PAF at baseline. LVEF was lower in the AF pro gression subjects compared with the non-AF progression subjects (P=0.001). Left atrial chamber size (LAD, P<0.001; LAD ≥50 mm, P<0.001; left atrial volume index [LAVI], P=0.004), concentric left ventricular hypertrophy (LVH, P=0.008), and mitral regurgitation (MR) grade (P<0.001) were higher in AF progression subjects compared with non-AF progression subjects as determined by TTE.
The clinical outcomes in patients with PAF at the 6-yr follow-up are shown in Table 3. The incidences of any event (P<0.001), re-admission rate (P=0.001), arrhythmic events (P=0.021) and DC cardioversion rate for rhythm control (P<0.001) were higher in AF progression subjects compared with non-AF progression subjects.
In univariate analysis, age at diagnosis, BMI, atrial arrhythmia during follow-up, LVEF, concentric LVH, LAD, and MR grade were significantly associated with AF progression. In multivariate analysis, age at diagnosis (P=0.009), atrial arrhythmia during follow-up (P=0.015), LAD (P=0.002) and MR grade (P=0.026) were independent risk factors for AF progression from PAF to PeAF or permanent AF (Table 4) at the long-term follow-up.
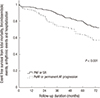
Kaplan-Meier curves show that the event free survivals of total mortality, thromboembolic events, arrhythmic events and hospitalizations (P<0.001; Fig. 2) and event free survivals of arrhythmic events (P=0.002; Fig. 3) are lower in AF progression subjects compared with non-AF progression subjects at the 6-yr follow-up. Fig. 4 shows that mean annual AF progression rate from PAF to PeAF or permanent AF in Korean populations was 10.7% at the 6-yr follow-up.
DISCUSSION
In this study, we show that the mean annual AF progression rate from PAF to PeAF or permanent AF in Korean populations was 10.7% at 6-yr follow-up and the patients with larger left atrial chamber size and severe MR grade were more likely to experience such progression, suggesting that underlying diseases might cause chronic stretching and atrial dilation, which seem to be important stimuli for chronic atrial structural remodeling. This is consistent with a previous study (16) that found chronic structural changes with cellular hypertrophy, fibroblast proliferation, and tissue fibrosis enables maintenance of AF. Younger patients at diagnosis and the patients with atrial arrhythmia during follow-up were also more likely to have experience progression of PAF to PeAF or permanent AF in our study. Considering the longer duration from the first diagnosis of PAF and in view of the fact that younger patients are associated with higher chances to make more substrates that might be arrhythmogenic foci, the age at diagnosis of PAF might be a good correlate to predict AF progression. And atrial arrhythmia during follow-up might be a clue for the progression of chronic atrial remodeling as arrhythmogenic substrates. Therefore, in these patients, intensive medical therapy with close clinical follow up is required.
This is the first study to evaluate the prognosis of patients with AF progression and validate a risk stratification to assess the probability of AF progression in Korean populations. Various factors were associated with AF progression, including valvular disease, alcohol consumption, age, left atrial dimension and enlargement over time, stroke, and heart failure. In our study, age at diagnosis, atrial arrhythmia during follow-up, LAD and MR grade were associated with AF progression.
Aging is associated with an increase in the prevalence of AF. The fibrosis in promoting the perpetuation of AF in aging hearts and age related development of collagenous septa have been described in human histological studies (4, 10, 17). In our study, patients with AF progression also were older than those without AF progression. This relationship between aging and atrial fibrosis is probably the major explanation of progression to permanent AF.
It is of interest that the patients with AF progression were younger at diagnosis, suggesting that AF duration was longer in the AF progression group. This finding is consistent with previous reports that as PAF lasted longer, progression to PeAF became more likely, which led to the adoption of the now oft-quoted adage "AF begets AF" (18, 19, 20).
In our study, LAD and MR grade were independent risk factors for predicting AF progression at long-term follow-up. The Framingham Heart Study demonstrated a 42% increased risk for development of AF with every 5 mm increment in left atrial size and the CARAF study demonstrates an increased risk of progressing to permanent AF with LADs in the upper range of normal or minimally enlarged (40-45 mm), a risk that increases further with larger diameters (9, 21). In our study, LAD (P<0.001) and larger LAD ≥50 mm (P<0.001) also were associated with AF progression in univariate analysis and LAD in logistic analysis (OR 1.071 [1.002-1.145], P=0.044) was an independent risk factor for prediction of AF progression in multivariate analysis.
Mitral regurgitation grade was associated with an increased probability of AF progression in our study. This finding is consistent with previous studies (9, 22) that have found that valvular lesions, such as moderate to severe mitral regurgitation and aortic stenosis, increase left atrial pressure and stretching and increase the propensity of AF.
There are higher incidences of total any events, including re-admission, arrhythmic events and DC cardioversion rate for rhythm control in patients with AF progression to PeAF or permanent AF at 6-yr follow-up, which supports the need to predict AF progression.
Previous studies have shown that a considerable number of patients with AF also develop clinically relevant sinus node dysfunction and AV block requiring permanent pacemakers (23, 24). In our study, there was a higher incidence of AV block in patients with AF progression (Table 3), which likely reflects an underlying atrial remodeling progression that may be involved as a substrate of AF both functionally and anatomically.
Arrhythmic events including atrial premature complex, atrial tachycardia (AT) and atrial flutter were also higher in patients with AF progression. This finding is consistent with a previous study (25) that found that patients destined to convert to PeAF were more likely to have AT/AF on any particular day and had a higher mean and median AT/AF burden that also increased progressively with time.
In our study, BMI was higher in patients with AF progression. This finding is consistent with the previous studies that showed the relationship among electromechanical remodeling and metabolic syndrome and that obesity and overweight are risk factors for incident AF (26, 27).
The rate of AF progression described in past studies varied between 8% and 22% after 1 yr of follow-up, depending on the rhythm monitoring methods used and definitions (9, 28). In our study, the mean annual AF progression rate was 10.6% (Fig. 4).
Based on the predictors of AF progression, a risk stratification rule to estimate the probability of AF progression in patients with PAF, the HATCH score, was developed (4, 29, 30). The premise of the HATCH score is early selection of patients for rhythm control therapy in an effort to prevent disease progression (4). However, in our study, there was no difference in HATCH score between groups.
Our study is the first to demonstrate a younger age at diagnosis-consistent with longer duration of AF, atrial arrhythmia during follow-up, left atrial chamber size, severe MR grade-important factors of electrical and structural remodeling. Those factors are associated with AF progression from PAF to PeAF or permanent AF in Korean populations.
There are some limitations to our study. First, this study was a single-center, retrospective study derived from a real world practice with inherent limitations. Hence the results of our study should be considered as hypothesis generating, and future prospective studies are warranted to confirm our results. Second, the definition of AF progression that we selected is arbitrary. In clinical practice, it is extremely difficult to determine the progression from PeAF to permanent AF because of the lack of a firm end point. Therefore, we defined AF progression to be from PAF to PeAF or permanent AF. Third, using the CARAF definitions, non-differential misclassification of PeAF and permanent AF is possible. To adjust for this, we required 2 consecutive annual visits with ECG evidence of permanent AF before the patient was designated as permanent for the analysis, making it likely that most patients with permanent AF would fit the newer definition (9, 31, 32). Fourth, patients with potentially reversible causes were excluded from the study. Therefore, the results of this study cannot be transferred to other patient populations with first detected PAF. Finally, according to current guidelines, catheter ablation was performed only in the few patients who had drug-refractory AF or who were intolerant to antiarrhythmic drug therapy.
In conclusion, the patients with younger age at diagnosis, atrial arrhythmia during follow-up, larger left atrial chamber size and severe MR grade are more likely to progress to PeAF or permanent AF, suggesting more intensive medical therapy with close clinical follow up would be required in those patients.







 XML Download
XML Download