

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bifurcation lesions occur in about 15% of percutaneous coronary interventions (PCIs) (1, 2). Since first introduction of balloon angioplasty, bifurcation lesion has been problematic to interventional cardiologists (3, 4, 5, 6). Even in drug-eluting stent (DES) era, bifurcation PCI has been associated with higher procedural failure and worse outcomes compared with PCI of non-bifurcated lesions (7, 8). There might be several problems during bifurcation PCI due to the anatomical structure: plaque shift, carina shift, jail of side branch (SB), the protruded stent strut in the lumen, and so on (9, 10, 11). Therefore, many interventional techniques for bifurcation lesions have been developed and used (9). These techniques are mainly categorized, according to the strategy for SB, into one-stent versus two-stent strategy. To date, no study showed clear advantages on one strategy. Mainly simpler techniques are slightly favored in the randomized trials (12, 13, 14). Previous studies demonstrated that one-stent strategy could be recommended as the routine bifurcation stenting technique (12, 13, 14, 15). Based on these study results, the strategy of stenting main vessel with provisional SB stenting is currently favored by most interventional cardiologists. However, we occasionally use two-stent strategy with various reasons, expecting more favorable SB outcomes. For example, we could perform SB stenting in advance, if SB is so stenotic and large that we might be concerned with the jail of that vessel during main vessel stenting. The main objective of this retrospective cohort study was to investigate the angiographic outcome of SB ostium in two-stent group, compared with one-stent group.
MATERIALS AND METHODS
Patient selection
This was a single-center bifurcation cohort study to analyze the results of bifurcation PCI from June 2003 through January 2008. The study population consisted of patients with symptomatic coronary artery disease who underwent elective and emergency coronary artery stenting of bifurcation lesion with one-stent or two-stent. Patients whose quantitative coronary angiography (QCA) data for both index PCI and follow up coronary angiography (CAG) were not available were excluded. Furthermore, bifurcation lesion with diameter of main vessel by visual estimate <2.5 mm or diameter of SB by visual estimate <2.0 mm was excluded. The study population was divided into 2 groups: a one-stent bifurcation stenting versus a two-stent bifurcation stenting. The one-stent bifurcation stenting group underwent stent implantation only at main vessel regardless of whether Percutaneous transluminal coronary angioplasty (PTCA) of the SB was performed or not. In contrast, the two-stent bifurcation stenting group underwent stenting both at main vessel and SB, regardless of whether initial strategy was two-stent strategy or not. The patients were treated with aspirin and clopidogrel before procedure. Those took oral 300 mg to 600 mg loading dose of clopidogrel before the index PCI if the patient had not taken clopidogrel within 24 hr prior to procedure. Aspirin was prescribed indefinitely, and clopidogrel was continued for at least 6 months.
Quantitative coronary angiography
Coronary angiography, performed at baseline, at completion of the stenting, and at follow-up, was analyzed in our angiographic core laboratory (Seoul National University Hospital, Seoul, Korea). We obtained quantitative angiographic measurements of the bifurcation lesion in three segments: proximal main vessel, distal main vessel and the SB segment. We measured the minimal luminal diameter (MLD) and reference diameter (RD) for each segment. Percent diameter stenosis was calculated by the equation: 100×(RD-MLD)/RD. Furthermore, SB ostium was defined as the first 5 mm of the SB.
Clinical outcomes
Clinical data of baseline and follow-up were obtained from outpatient medical records or telephone interviews. The major adverse cardiac events (MACE) of this study were a composite of all cause death, myocardial infarction and target vessel revascularization (TVR) including target lesion revascularization (TLR). TVR was defined as any repeat PCI or surgical bypass of any segment of the target vessel. TLR was defined as any repeat PCI of the lesion within 5 mm of the stent or surgical bypass of the target vessel. Myocardial infarction was defined as new significant electrocardiographic Q waves or a creatinine kinase-MB isoenzyme (CK-MB) level >3 times the upper limit of normal.
Statistical analysis
All data are expressed as the mean values±SD or as numbers (percentages). The baseline characteristics of the groups and follow-up data were compared by t-test for continuous variables and by the chi-square statistic for categorical variables. All statistical analyses were performed using SPSS 12.0 (SPSS Inc., Chicago, IL, USA), and a P value of <0.05 was considered statistically significant.
RESULTS
Patient and lesion characteristics
From June 2003 to January 2008, 692 consecutive patients underwent coronary intervention for bifurcation lesion with drug eluting stent. Of these patients, we selected the patients whose follow-up coronary angiography and QCA data were available, after excluding the lesions of which main vessel or side branch were small (Fig. 1).
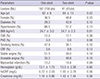
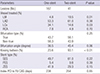
The study population consisted of 199 patients who underwent elective or emergency intracoronary stent implantation at bifurcation lesion (208 lesions). Of these patients, 158 patients (167 lesions) were treated with one-stent stenting for bifurcation lesions and 41 patients (41 lesions) underwent two-stent stenting. The baseline clinical characteristics are presented in Table 1 and the angiographic data are shown in Table 2. Left main bifurcation lesions were more frequently treated by two-stent technique whereas bifurcation lesions of left circumflex artery were more frequently treated by one-stent technique. Kissing ballooning was more commonly performed in two-stent group as expected (23.5% in one-stent vs. 93.1% in two-stent, respectively) (P<0.01). But both groups are similar in terms of bifurcation angle, stent type, and mean duration of follow-up coronary angiography which was about 8 months after PCI.
Quantitative coronary angiography analysis
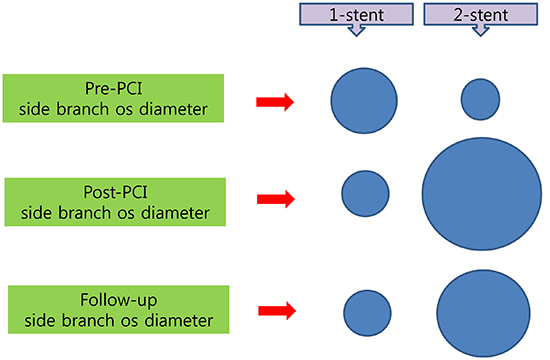
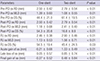
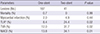
The angiographic results are presented in Table 3. Prior to coronary intervention, the ostium diameter tended to be larger in the one-stent group (1.39±0.60 mm vs. 1.08±0.55 mm, P=0.01). However, the reference diameter was larger in the two-stent group, reflecting the fact that there was hemodynamically more important SB in this group (2.50±0.42 mm vs. 2.79±0.54 mm, P<0.01). After treatment, wider ostium of SB was attained in the two-stent group (1.18±0.68 mm vs. 2.41±0.10 mm, P<0.01). Also, in terms of diameter stenosis, more favorable result was obtained in the two-stent group. Acute gain was -0.21±0.68 mm in the one-stent group and 1.33±0.49 mm in the two-stent group (P<0.01). In the follow-up coronary angiography, the late loss of SB ostium was significantly larger in the two-stent group, which is consistent with the previous studies. In spite of greater late loss of SB ostium MLD in two-stent group, the final gain of SB ostium diameter was still greater than one-stent group (difference of MLD between follow-up and before PCI; -0.27±0.52 mm in the one-stent group and 0.48±0.84 mm in the two-stent) (P<0.01).
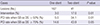
The rates of SB intervention during follow-up are given in Table 4. Actually, SB interventions were more frequently performed in the two-stent group during follow-up period. In the cases of SB diameter stenosis more than 50% at follow-up angiogram, the rate of SB intervention was 5.0% and 34.1% in one-stent and two-stent group, respectively (P<0.01). In the cases of SB diameter stenosis more than 70%, the rate increased to 14.6% and 43.9%, respectively, demonstrating the tendency of more common re-intervention of SB at follow up in the two-stent group (P=0.05). The rate of re-intervention of main vessel at follow up, however, was similar between two groups; 7.1% and 7.3%, respectively (P >0.99).
Clinical outcome
The clinical outcomes are shown in Table 5. Mortality rates were less than 1% in both groups with no significant difference between them (0.7% vs. 0%; one- vs. two-stent group; P >0.99). Moreover, the rate of myocardial infarction was not statistically different between two groups with less than 5% (2.0% vs. 4.9%; one- vs. two-stent group; P=0.44). Accordingly, the incidence of hard end points was not different. However, the incidence of TLR and TVR considered to be soft endpoints was 24.4% and 31.7% in two-stent group, which was higher than in one-stent group by 16.0% and 19.7% (P=0.02 respectively). TLR included main vessel and side branch revascularization. However, only main vessel revascularization was included if no intervention was done at index procedure at side branch in the case of one-stent group. The rate of MACE (mortality, myocardial infarction, TLR and TVR) during 1 yr follow-up was higher in two-stent group, which was mainly driven by the difference of TLR and TVR.
DISCUSSION
The main finding of this study is that, due to the remarkable acute gain after stenting, we could attain wider final SB ostium at follow up after two-stent technique for bifurcation lesion in spite of greater late loss, compared with one-stent technique. This is in favor of two-stent technique in terms of final SB ostium, considering that there were relatively worse baseline characteristics in two-stent group although statistically insignificant. Interesting paradox is that the greater late loss at the stented SB results in more frequent re-intervention of SB in spite of wider SB ostium.
The QCA analysis of follow-up coronary angiography for one-stent and two-stent techniques for bifurcation lesion revealed several findings. First, the reference diameter of SB ostium in two-stent group was wider than in one-stent group. This means that larger SB is more likely to be treated with stent than smaller SB. There is no established guideline for SB stenting which was made by any authoritative organization. However, the general consensus is to try to keep the bifurcation intervention safe and simple. Nevertheless, two-stent strategy is appropriate when SB is significantly stenotic and SB is relatively big vessel (i.e.>2.5 mm) (16). In our study, SB in two-stent group was bigger and more stenotic than in one-stent group, which is in accordance with general consensus. Moreover, this might be the reason why operators performed one-stent stenting in one-stent group. Second, the ostium of SB in two-stent group after intervention was wider than in one-stent group. This means that we could get favorable immediate result by two-stent technique, although there might be possibility of restenosis or stent thrombosis. Third, the late loss of SB ostium was larger in two-stent group. Consequently, the initial remarkable acute gain after SB stenting was partly offset by the late loss. Nevertheless, wider SB ostium at the time of follow-up coronary angiography was demonstrated in the two-stent group, even thought the late loss was larger than previous studies (17, 18). In addition, more favorable diameter stenosis was proven, too. In the future study, we might be able to prove the functional benefit of such a wider SB ostium using fractional flow reserve (FFR) that is known to be a useful tool to investigate the functional significance for the stenotic coronary lesion (10).
The incidence of death and myocardial infarction in the follow-up period was low and similar in both groups. However, TLR and TVR rates were higher in two-stent group than one-stent group. Interesting paradox was observed in QCA result. The two-stent technique provided greater acute gain and wider final SB ostium at follow up angiography despite greater late loss, in comparison with the one-stent technique. We could consider that the greater late loss at the stented SB may induce oculostenotic reflex and TLR in two-stent group. Obviously, a follow up angiography may detect asymptomatic moderate restenosis and induce TLR that may not be performed if follow up angiography was not done. In our study, we included only the subjects who underwent follow-up coronary angiography. This might be responsible for higher rate of revascularization compared with other previous studies (12, 13).
The analysis of SB intervention during follow-up period in the respective stenting groups made new information. The SB intervention rate was higher in two-stent group, although SB ostium width and diameter stenosis were more favorable in this group. This contradictory result might be explained by so-called oculostenotic reflex (19). Oculostenotic reflex refers to the phenomenon that if an amenable lesion is found in the coronary angiography, all patients (even asymptomatic) would receive a stent. This reflex is thought to be more likely to happen in the stenotic lesion previously intervened with stent, because interventionist might be willing to compensate for the late loss. Actually, in our study, examining the SB intervention during follow-up, the PCI rate of SB ostium was higher in two-stent group than in one-stent group, even when the diameter stenosis was comparable between two groups. However, main vessel revascularization rate was not significantly different between two groups. Therefore, we could understand that the greater late loss might induce oculostenotic reflex resulting in more frequent re-intervention for the stented SB. Recently, Gao et al. demonstrated that the overall risks of TLR and TVR were comparable between a simple strategy and a complex strategy in a meta-analysis of nine randomized trials (20). However, the simple strategy was associated with a reduced risk of myocardial infarction. Considering the nature of randomized trial, there might be more objective judgement than our retrospective study reflecting real world practice, possibly excluding oculostenotic reflex.
Most interventionists prefer the simple stenting for the bifurcation lesion to the complex one. Actually, randomized clinical trials support the simple strategy (15, 16, 17, 18). In addition, final kissing balloon dilatation in general shows better side branch results (21). However, the merit of complex stenting might be underestimated, although it provides wider long-term SB ostium after PCI as well as immediate result. In fact, general consensus admits the appropriateness of SB stenting, when SB is significantly stenotic and big enough. Given the complexity of bifurcation lesions or importance of SB, the complex stenting would be performed adequately. However, we should keep in mind that we have to try not to be influenced by the temptation named as oculostenotic reflex during follow-up. Faced with restenosis at the SB, we had better perform FFR, intravascular ultrasound, noninvasive stress test and so on. With these additional data, we could escape from unnecessary revascularization for SB and oculostenotic reflex. A larger prospective study including functional study would show the realistic value of two-stent technique in terms of ischemic burden of myocardium.
Our study has several limitations. First, this study was a nonrandomized retrospective analysis of bifurcation cohort from one center; therefore the results and conclusions are subject to the limitations inherent in this type of studies. This study did not compare two techniques by an intention-to-treat analysis which is usual in randomized trials. Second, we analyzed only the subjects whose follow-up coronary angiography and QCA data were available, which may have introduced a selection bias in the analysis. Mandatory follow up angiography may increase the TVR rate, which may not reflect the real-world practice where follow up angiography is not usually done. Third, this study focused on quantitative coronary angiographic data and did not include functional studies.
In conclusion, two-stent technique for bifurcation lesion provides a remarkable acute gain and wider long-term SB ostium at follow up angiography despite greater late loss, in comparison with one-stent technique. Considering wider long-term SB ostium, we might expect, at least, more favorable angiographic outcome with two-stent strategy. The greater late loss of the stented SB increased TVR rate in two-stent technique probably due to oculostenotic reflex. Thus, if we could avoid oculostenotic reflex, prevent thrombotic events, and further reduce late loss using new DES, two-stent technique would be more positively considered.

 XML Download
XML Download