

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Post-operative remnant thyroid ablation using radioiodine followed by total or near total thyroidectomy is a mainstay in the management of patients with differentiated thyroid carcinoma (DTC). Remnant ablation eliminating residual thyroid tissues has been credited for improving sensitivity of serum thyroglobulin (Tg) monitoring and reducing the likelihood of recurrence (1, 2). These clinical benefits of remnant ablation mainly stem from facilitating complete initial staging to detect previously unrecognized metastases via a post-therapy whole body scan (RxWBS); enabling early detection of recurrence via serum Tg monitoring with/without a diagnostic (DxWBS) or RxWBS; serving as an adjuvant therapy by destroying suspected but unproven metastatic disease (3, 4, 5).
The appropriate amount of radioactivity for remnant ablation has been recommended by major guidelines for managing patients with thyroid cancer (3, 4). However, these guidelines provide only broad guidance with a wide range of administered radioactivity (1.1-3.7 GBq) because radioiodine ablation using 1.1 GBq and 3.7 GBq shows similar rates of successful remnant ablation and recurrence rates (6). Although higher radioiodine activities are likely to achieve higher ablation rates, more frequent side effects such as thyroiditis, sialoadenitis, and nasolacrimal duct obstruction are unavoidable (7, 8, 9, 10, 11). Moreover, recent randomized and prospective studies have reported that low radioiodine activity (1.1 GBq) is as effective as high radioiodine activity (3.7 GBq) to decrease serum Tg levels and destroy remnant thyroid tissue (12, 13). In particular, in patients with low-risk thyroid cancer, the use of minimum radioactivity should be required to achieve beneficial effects of remnant thyroid ablation as well as avoid unnecessary exposure to radiation.
Controversies exist on determining the total amount of administered radioactivity and number of radioiodine therapy sessions to complete remnant ablation. Successful remnant ablation is defined as an absence of visible radioiodine uptake on a subsequent scan or undetectable serum Tg (3). It is not easy to predict the outcome of radioiodine therapy in consideration of differences in the amount of residual thyroid tissues left in situ after surgery, preparation status including thyroid stimulating hormone level (TSH) and low iodine diet, and the effective biological half-life of radioiodine. Fixed radioactivity of 1.1 GBq is preferred in most countries based on feasibility of safety regulations about the release of patients after radioiodine administration and similar results with that of a high activity radioiodine ablation. However, a considerable number of patients need more than two sessions of radioiodine to complete remnant ablation. It would be of great importance to utilize prognostic factors of radioiodine ablation for the management of thyroid cancer. In this regard, we analyzed clinical outcomes of remnant ablation with 1.1 GBq of radioiodine in patients with low to intermediate-risk DTC, to suggest an optimized remnant thyroid ablation protocol.
MATERIALS AND METHODS
Patients
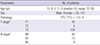
Among 780 patients with DTC who underwent total thyroidectomy from June 2006 to June 2012, 225 were treated with 1.1 GBq of radioiodine for remnant thyroid ablation at our institute. Patients with low to intermediate risk were included based on the guidelines (3, 4). Consequently, patients who presented with distant metastases (n=2), locoregional tissue invasion or macroscopic extrathyroidal extension (n=18), or recurred before completion of remnant ablation (n=2) were excluded from the study. In addition, patients who were not followed 6-12 months later with TSH stimulated Tg (off-Tg) measurements (n=16) and follow-up DxWBS (n=12), were not included. Finally, 176 patients (25 males and 151 females) were retrospectively analyzed for this study. Detailed demographic data are summarized in Table 1.
Preparation for remnant thyroid ablation
All patients were requested to follow a strict thyroid hormone withdrawal regimen in conjunction with a strict low iodine diet. For thyroid hormone withdrawal, levothyroxine supplementation was discontinued at 4 weeks before radioiodine administration and switched to triiodothyronine supplementation for 2 weeks. At 2 weeks before radioiodine administration, all forms of thyroid hormone supplementation were completely prohibited, and a strict low-iodine diet was started at the same time. The low-iodine diet was continued until 3 days after radioiodine administration.
Post-therapy WBS
An RxWBS was performed 3 days after radioiodine administration. Using a gamma camera equipped with a high-energy parallel hole collimator (Infinia Hawkeye 4, GE Healthcare, Parsippany, NJ, USA), whole body images were obtained at a 20% symmetrical window that was centered at 364 keV. RxWBS images were visually interpreted based on a consensus between two nuclear medicine physicians with extensive experience in thyroid imaging; as definite versus no uptake.
Serum Tg and anti-Tg antibody measurements
Serum levels of TSH, Tg, and Tg-Ab were measured on the day of radioiodine administration in all patients. Serum Tg and Tg-Ab titers were considered valid only when serum TSH level was >30 µIU/mL. Serum Tg levels were determined in duplicate using an immunoradiometric assay (Cisbio Bioassays, Codolet, France). Serum Tg-Ab levels were determined in duplicate using a radioimmunoassay (Brahms, Mannheim, Germany). In addition, ratio of urine iodide of creatinine levels (µI/Cr) was measured using an ion-selective electrode method (NeoMet, ISTEK, Seoul, Korea) to evaluate low iodine diet status, which was performed in 66 patients.
Clinical outcome assessment
The completion of remnant thyroid ablation was determined only when no visible radioiodine uptake was observed in the thyroid bed on a WBS and serum off-Tg level became undetectable (<1.0 ng/mL). Subsequent radioiodine therapy or follow-up DxRBS and serum off-Tg measurement were repeated with a 6-12 months interval until complete remnant ablation was achieved.
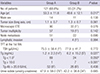
Patients who were confirmed to have complete thyroid ablation on the first post-therapy evaluation or the follow-up evaluation were classified into Group A. Patients who required radioiodine therapy more than twice to complete thyroid ablation were classified into Group B. Demographic data and prognostic factors including age, sex, TNM staging, serum levels of TSH, serum Tg and Tg-Ab, and µI/Cr were compared between the two groups (Table 2).
Statistical analysis
All statistical analyses were performed using SPSS ver. 18.0, software (SPSS Inc., Chicago, IL, USA). All the continuous data were expressed as mean±standard deviation. Comparisons of continuous values were performed with the independent t-test, and independence tests of non-continuous values were carried out by Pearson's chi-square test. Binary multivariate logistic regression analysis was used to identify independently related factors to the first radioiodine therapy results. Linear-by-linear association analysis was adopted for subgroup analysis to identify the trend of ablation success rates. P values<0.05 were considered significant.
RESULTS
The remnant ablation results of low radioiodine activity were quite excellent in patients with low-risk thyroid cancer. Among 188 patients who were enrolled in this study, outcomes of the first radioiodine administration were assessable in 176 patients. With the first radioiodine administration, 68.8% (n=121/176) of the patients achieved successful remnant ablation; they were classified into Group A. In particular, 9 patients already had no remnant thyroid tissue, as proven by no visible uptake on an RxWBS and undetectable off-Tg. On the other hand, 55 patients who had more than two times of radioiodine administration were classified into Group B. However, remnant ablation results were disappointing in Group B, compared to Group A. Only 28.8% (n=15/52) of Group B patients completed remnant ablation, and received a significantly large amount of radioiodine (3.4±0.6 times, 3.7±0.7 GBq) than that of Group A patients.
To identify factors related with the ablation success rate at the first radioiodine administration, various factors were compared; age, sex, size (long axis), microscopic extrathyroidal extension (mETE), tumor multiplicity, lymphatic invasion, N stage, serum levels of TSH, Tg, Tg-Ab, µI/Cr at the first radioiodine administration (Table 2). A univariate analysis revealed that age, and Tg level at the first radioiodine administration (pre-ablative Tg) were significantly different between Group A and Group B. Group A patients were significantly older than Group B patients (53.3±11.8 yr vs. 48.6±12.1 yr, P=0.017) and presented with significantly lower pre-ablative Tg levels than those of Group B patients (1.2±2.3 ng/mL vs. 6.2±15.2 ng/mL, P=0.027). Binary multivariate logistic regression analysis was performed for age and pre-ablative Tg. Consequently, it turned out that only pre-ablative Tg was an independent factor (odds ratio, 1.138, P=0.021) related with the first radioiodine ablation results (Table 3).
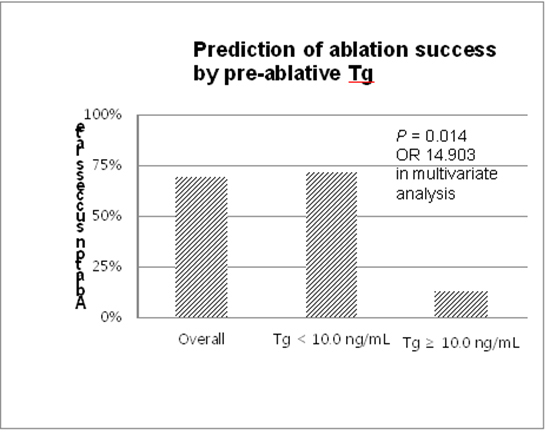
Pre-ablative Tg was further evaluated as a potential factor for predicting successful remnant ablation at the first radioiodine administration. Patients with lower pre-ablative Tg were more likely to achieve remnant ablation at the first radioiodine administration (P=0.004, Fig. 1). The diagnostic performance of pre-ablative Tg was analyzed with two cutoff values of 1.0 ng/mL and 10.0 ng/mL, respectively. Patients presenting with pre-ablative Tg<1.0 ng/mL were more frequent in Group A with a borderline significance (P=0.050). Diagnostic performances of pre-ablative Tg<1.0 ng/mL were sensitivity of 64.5%, specificity of 52.0%, positive predictive value (PPV) 74.2%, and negative predictive value (NPV) of 40.6%. When the cutoff raised to 10.0 ng/mL, patients presenting with pre-ablative Tg<10.0 ng/mL were more likely to be found in Group A, with a stronger statistical significance (P<0.001). Diagnostic performances of pre-ablative Tg<10.0 ng/mL were sensitivity of 99.1%, specificity of 14.0%, PPV of 71.1%, and NPV of 87.5% (Table 4). In addition, repeated multivariate logistic regression analyses showed that patients presenting with pre-ablative Tg≥10.0 ng/mL had a 14.9 times higher risk of failure at the first radioiodine administration than those not.
DISCUSSION
The total amount and number of radioiodine therapy required for complete remnant ablation are of great concern to many clinicians and patients, so as to avoid unnecessary exposure to radiation and minimize adverse effects of radioiodine. However, the minimum radioactivity recommended for remnant ablation has quite a broad range from 1.1 to 3.7 GBq. Recently, randomized trials reported that a low activity of radioiodine (1.1 GBq) is as effective as a high activity of radioiodine (3.7 GBq) to ablate small normal thyroid remnants after total thyroidectomy (12, 13). We found that the first radioiodine administration of 1.1 GBq was enough to achieve remnant ablation in 68.8% of patients with low to intermediate risk thyroid cancer, and pre-ablative Tg less than 10.0 ng/mL could be a useful factor predicting success remnant ablation of the first radioiodine administration.
The ablation success rate of the present study was lower than those of the randomized trials, ranging from 90-94% (12, 13), mainly because of the differences in the criteria for complete remnant ablation. Schlumberger et al. assessed thyroid ablation with neck ultrasonography and serum off-Tg level or a DxWBS in patients with detectable Tg-Ab (13). Serum Tg measurement is more sensitive than a DxWBS for detecting recurrence and metastasis, and thus a diagnostic radioiodine scan at 6-12 months later is no longer routinely performed in low-risk thyroid cancer patients with no visible uptake outside the thyroid bed (14, 15). However, complete remnant ablation was given only when there was no visible uptake on RxWBS and undetectable off-Tg at 6 months follow-up in the present study.
Several factors were additionally considered to determine complete remnant ablation in the present study. Most patient population comprised intermediate-risk DTC. There are also false negative Tg and true positive radioiodine scan cases, although they are infrequent. It could be helpful to combine radioiodine scan and serum Tg measurement in a complementary way for detecting recurrence and metastasis (16). In this regard, the present study adopted more strict criteria for complete remnant ablation and reported lower ablation success rate with 68.8% than the randomized trials.
The current study performed in a high-iodine intake area. Epidemiology of thyroid cancer including incidence and histology differs by iodine intake amounts. It is well known that excess iodide suppresses thyroid function via down-regulation of Na/I symporter (NIS) mRNA. In addition, patients have difficulties to accomplish a strict low-iodine diet for radioiodine therapy. These environmental conditions could lead a decrease in the delivered radioactivity to remnant thyroid tissues. Despite these unfavorable conditions, a single administration of low-activity radioiodine was enough to achieve complete remnant ablation in patients with low to intermediate-risk DTC.
A total of 136 patients completed remnant thyroid ablation with 2.1 times and 2.3 GBq of radioiodine, on average. Among them, 68.8% of patients achieved remnant ablation with the first radioiodine administration. This ablation results are remarkable in terms of both total amount and number of radioiodine administrations when compared with a previous study that was performed in Korean patients with thyroid cancer almost two decades ago. Kim et al. reported that successful remnant ablation was confirmed in 51% of patients who were treated with a low radioiodine activity of 1.1 GBq, which was achieved in only 24% of patients at the first radioiodine administration (17). The differences in remnant thyroid ablation results between the two studies might be due to heterogeneous patient populations related to the extent of thyroid surgery. Most patients with thyroid cancer are currently treated with total or near total thyroidectomy, and have a small amount of normal-remnant thyroid. Therefore, a single administration of low radioiodine activity could be sufficient to ablate remnant thyroid tissues in patients with low-risk thyroid cancer who performed total or near total extent of thyroidectomy.
We found that a considerable number of patients (Group A patients, n=121) could have completed remnant thyroid ablation at the first radioiodine administration. Particularly, a few patients (n=9) in Group A already had no remnant thyroid tissue, as there was no visible uptake on a scan and undetectable pre-ablative Tg at the first radioiodine administration. Except these 9 patients, remaining patients (n=112) were in danger of unnecessary radiation exposure since they received the second radioiodine administration. Group B patients (n=55) and vice versa could have put up with risks incurred by incompletion of remnant thyroid ablation, if they decided to stop radioiodine therapy without a follow-up DxWBS and/or subsequent radioiodine administration or serum off-Tg measurement. It is a complicated matter to weigh the importance between the two clinical situations; potential hazards from unnecessary radiation exposure versus recurrence risks from incomplete remnant ablation.
DxWBS can be a useful tool to decide the subsequent radioiodine therapy, but it is not commonly used in Korea. DxWBS requires a thyroid hormone withdrawal and a strict low iodine diet. It is extremely stressful for patients to keep a low iodine diet for 2 weeks in a region taking dietary iodine almost 20 times more than that of the recommended amount for a low iodine diet. Moreover, there is another concern for "thyroid stunning". Thyroid stunning is a phenomenon that a small amount of radioiodine for DxWBS might decrease iodine uptake on the followed radioiodine therapy (18, 19). Thus, it would be of great importance in the management of thyroid cancer patients, to predict successful remnant ablation and select patients who are in need of the subsequent radioiodine therapy. We revealed that only pre-ablative Tg was an independent factor for predicting successful remnant ablation at the first radioiodine administration. The importance of pre-ablative Tg is well consistent with previous clinical studies (20, 21, 22, 23). A meta-analysis including 14 articles and nearly 4,000 patients with thyroid cancer clearly showed that serum Tg levels<10 ng/mL just before radioiodine remnant ablation has a high NPV of 94.2% and a low PPV of 47.0% (24). Although the number of the patients was smaller than the meta-analysis, we could derive confident and reliable analyses since the study population was homogeneous and treated with one fixed radioiodine activity under a unified protocol. In the present study, a cutoff value of 10.0 ng/mL resulted in a higher PPV (71.1% vs. 47.0%), but a slightly lower NPV (85.7% vs. 94.2%). A higher PPV is a more important property than a higher NPV since it would be helpful to avoid unnecessary radioiodine administration. In this regard, pre-ablative Tg is a promising factor to assist remnant thyroid ablation in the management of patients with low-risk thyroid cancer. It is less likely that patients presenting with pre-ablative Tg greater than 10.0 ng/mL achieve complete remnant ablation at the first radioiodine therapy. In such cases, the subsequent radioiodine therapy might be needed to follow 6-12 months later based on Tg level and DxWBS.
Serum Tg level is related to the mass of thyroid tissue left in situ after near-total thyroidectomy. However, there is currently no universally accepted serum Tg cutoff value to decide disease-free status, although serum Tg measured just before remnant thyroid ablation has been suggested in the selection of patients for the remnant thyroid ablation (25, 26). Post-operative serum Tg levels should be cautiously interpreted considering various compounding factors, such as surgical techniques affecting the amount of remnant thyroid tissue, differences in Tg secretion ability, and sensitivity to TSH from remnant thyroid tissues and tumors. It has also been reported that the effectiveness of radioiodine remnant ablation varies and depends on the amount of radioactivity as well as remnant thyroid tissue. In the present study, no significant differences were found in remnant ablation results by operating surgeons, and all patients were treated with a single low radioiodine activity. Thus, potential influences caused by technical factors and differences in radioactivity could be excluded from the results interpretation.
The clinical usefulness of the off-Tg measurement is deliberately considered in the determination of remnant thyroid ablation. Currently, an absence of visible radioiodine uptake on a subsequent DxWBS or undetectable serum Tg is regarded as the successful remnant ablation (3). However, there are significant discordances between the absence of visible uptake on a scan and serum off-Tg levels. It is well known that thyroid remnant tissues are present in the vast majority of patients undergoing near-total thyroidectomy (26, 27). In the present study, remnant thyroid uptake was definitely visualized in 94.8% (n= 167/176), and pre-ablative Tg levels were already below 10.0 ng/mL in 96.5% (n=170/176) of the patients. Surprisingly, pre-ablative Tg levels were less than 1.0 ng/mL in 52.8% (n=93/176) of patients, and most of them (n=84/93, 90.3%) showed remnant thyroid uptake on the RxWBS. However, remnant thyroid uptake was persistently seen in 28% of patients showing pre-ablative Tg less than 1.0 ng/mL on the subsequent RxWBS or DxWBS. Therefore, undetectable Tg level (<1.0 ng/mL) does not always guarantee the disappearance of the remnant thyroid tissues, and it is too hasty to discard the complementary use of a radioiodine scan in the management of DTC.
Successful remnant ablation was achieved in a considerably high number of patients with a single administration of low radioiodine activity in patients with low to intermediate-risk thyroid cancer. A pre-ablative Tg is a promising factor to predict the success rate of the first radioiodine administration. To confirm remnant thyroid ablation, a follow-up DxWBS would be recommended for patients with a pre-ablative Tg less than 10.0 ng/mL, and a subsequent radioiodine administration would be saved for those with a pre-ablative Tg greater than 10.0 ng/mL.



 XML Download
XML Download