

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is an obstructive lung disease diagnosed by variable airway obstruction. However, before diagnosis, other underlying causes should be excluded (1). One of them is diffuse panbronchiolitis (DPB) which incidence is high among Asians, especially Koreans and Japanese (2). Clinical manifestations of DPB are cough, dyspnea, and crackling sounds. A chest image shows bilateral centrilobular nodules. Although DPB is distinct from asthma, their clinical manifestations can overlap (3) and co-occurrence of DPB and asthma is possible in East Asian patients (4).
DPB can be treated successfully with long-term, low-dose macrolide administration. The effectiveness of macrolide has been confirmed in a double-blind, placebo-controlled study (5). Macrolide is an antimicrobial and anti-inflammatory agent (6). Macrolide can alter neutrophil functions, inhibit oxidant production, and influence the production of various cytokines and chemokines, such as interleukin (IL)-1, IL-6, IL-8, IL-10, and tumor necrosis factor (7). In this report, we describe 5 Korean patients with DPB who clinically presented with severe asthma but for whom computed tomography (CT) findings were suggestive of DPB; these patients showed a good response to long-term macrolide treatment.
CASE DESCRIPTION
Case 1
A 71-yr-old woman referred for a 10-yr history of cough, dyspnea, sputum, post-nasal drip on 4th June 2010. Her breathing sound was clear. A chest x-ray (CXR) showed increased bronchovascular markings in the both lower lungs and consolidation in the left lower lung field (LLLF) (Fig. 1A). Initial forced expiratory volume in 1 second (FEV1) was 1.21 L (64.9%) and forced vital capacity (FVC) was 1.70 L (75.5%) and FEV1/FVC was 71.1% without a bronchodilator (BD) response. The methacholine bronchial provocation test (MBPT) was positive as a result of provocative concentration (PC20) was 3.8 mg/mL. Induced sputum showed mild eosinophilia (3%). During one month of asthma treatment with inhaled budesonide combined with formoterol, theophylline, and montelukast, she complained of mild fever and yellowish sputum. Thus, we performed a chest CT and water's view x-ray. Bilateral maxillary sinusitis was observed (Fig. 1B). CT showed bronchial wall thickening with centrilobular nodules, which was suggestive of DPB (Fig. 1C, D). To differentiate from mycobacterial infection (8), acid fast bacilli (AFB) studies were done and showed negative. The patient took clarithromycin 250 mg twice a day for 9 months, after which her FEV1 improved from 64.9% to 84.2%, FVC and FEV1/FVC also improved. A follow-up examination, LLLF consolidation and sputum eosinophilia disappeared. In addition, she was able to reduce the daily amount of inhaled steroid and discontinue theophylline.
Case 2
A 52-yr old man visited for a 4-yr history of cough, dyspnea, sneezing, rhinorrhea, and wheezing on 25th June 2010. Initial FEV1 was 1.74 L (54.4%), FVC was 2.40 L (61.3%), and FEV1/FVC was 72.5%. BD response was positive (FEV1 increased 20.6%, 270 mL). CXR showed multiple nodules in both lungs. A sinus CT showed bilateral maxillary sinusitis. A chest CT showed a tree-in-bud appearance and air trapping in both lower lungs. Induced sputum showed neutrophilia. He showed a poor response to inhaled budesonide combined with formoterol and montelukast. As AFB studies were negative, we administered clarithromycin. The patient took clarithromycin 250 mg twice a day for 9 months, after which FEV1 improved from 54.4% to 95.3%, FVC improved from 61.3% to 92.8%, and FEV1/FVC also improved. Cough and sputum disappeared. He now takes montelukast and clarithromycin without respiratory symptoms.
Case 3
A 25-yr-old man had a 5-yr history of cough and dyspnea on 28th March 2007. Initial FEV1 was 2.51 L (62.6%), FVC was 3.65 L (77.8%), and FEV1/FVC was 68.8%. BD response was negative. The results of a MBPT were positive (PC20 4.36 mg/mL). A CXR showed miliary nodules in both lungs, but he didn't have sinusitis. A chest CT showed bronchiolectasis and centrilobular nodules on both lungs (Fig. 2A, B). Induced sputum showed severe eosinophilia (42%). The AFB studies were negative. He took inhaled fluticasone combined with salmeterol, montelukast, and theophylline, and he intermittently used 30 mg of prednisolone (PL) for asthma attacks. After the patient took clarithromycin 250 mg twice a day for 9 months, his FEV1 improved from 62.6% to 88.4%, and he could reduce the amount of PL. Before the patient had started taking clarithromycin, he had taken 720 mg of PL per year. After he treated with clarithromycin, he was able to reduce use of oral steroids by about 80%, such that he took 150 mg per year.
Case 4
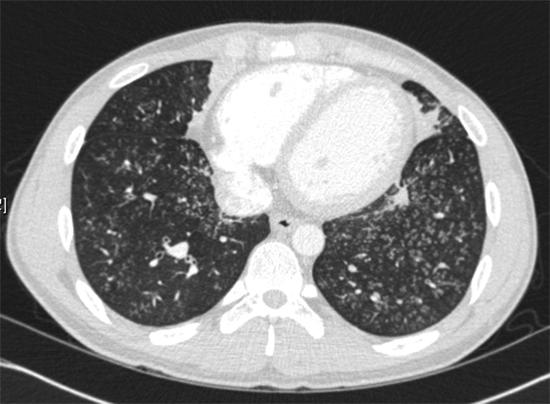
A 60-yr-old woman referred for a 5-yr history of severe asthma on 18th August 2010. Cough and dyspnea were her main symptoms. Her initial FEV1 was 0.88 L (42.9%), FVC was 1.10 L (44.9%), and FEV1/FVC was 73.4% without a BD response. A crackling sound was heard in both lungs. A chest CT showed diffuse bronchial wall thickening and centrilobular nodules with a tree-in-bud appearance in both lower lungs (Fig. 3A, B). Induced sputum showed 2% eosinophils. A MBPT could not be performed. Water's view showed bilateral maxillary sinusitis. She had been using inhaled budesonide combined with formoterol, a tiotropium inhaler, montelukast, and theophylline for a month. After a month, she complained of continuous cough and sputum. The crackling sound was consistently heard. The AFB studies were negative, and clarithromycin was introduced. The patient took clarithromycin 250 mg twice a day for 5.5 months with asthma medication, after which her FEV1 improved from 0.88 L (42.9%) to 1.96 L (97.1%), and FVC improved from 44.9% to 98.8%. Follow-up chest CT after a year showed improved centrilobular nodules in both lungs. She was able to discontinue budesonide and formoterol.
Case 5
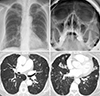
A 69-yr-old man came with a 3-yr history of cough, sputum, and dyspnea on 11th July 2012. His initial FEV1 was 1.88 L (79.2%), FVC was 2.34 L (76.8%), and FEV1/FVC ratio was 80.3%. FEV1 increased 13.2% (250 mL) after bronchodilator inhalation. Induced sputum showed neutrophilia without eosinophils. CXR showed tiny nodules and bronchial wall thickening in both lower lungs (Fig. 4A). Water's view showed left maxillary sinusitis (Fig. 4B). A chest CT showed severe and diffuse centrilobular nodules and branching linear opacities in both lungs (Fig. 4C). The AFB studies were negative. He was prescribed fluticasone combined with salmeterol, pranlukast, myrtol, and clarithromycin. After the patient took clarithromycin 250 mg twice a day for 40 days, his cough and sputum decreased. A follow-up CT showed a slight decrease in bronchial wall thickening and multiple nodules throughout both lungs (Fig. 4D). After 8 months of clarithromycin, he was able to use only fluticasone and salmeterol inhaler with clarithromycin. His FEV1 increased from 79.2% to 127.0%, and FVC increased from 76.8% to 118.9%.
The study occurred in the allergy clinic of a tertiary teaching hospital in Korea. We collected 5 patients who visited as severe asthma but treated well with DPB treatment. Institutional review board reviewed and approved this study (4-2014-0362).
DISCUSSION
All patients in this study were referred to our clinic with treatment resistant severe asthma, but our report shows that DPB should be excluded before diagnosing asthma in East Asian patients. As DPB is a progressive inflammatory airway disease and can be treated by long-term administration of macrolide (9), accurate diagnosis is especially important. Both asthma and DPB patients complain of chronic cough, sputum, and dyspnea, and it is not easy to discriminate between the two diseases. All 5 patients had CT findings that were consistent with DPB, and all showed marked improvement in lung function and clinical symptoms with long-term macrolide treatment.
In this study, all patients were treated with clarithromycin, which consists of 14-membered ring macrolides. The mechanism by which macrolides manage DPB may be related to their immune modifying effects. Only 14-membered ring macrolides (erythromycin, clarithromycin, and roxithromycin) and 15-membered ring macrolides (azithromycin) are effective; 16-membered ring macrolides are not effective. The structure of macrolides determines their immune modifying activity (10), and it has been reported that macrolides could reduce airway mucus secretion and decrease airway neutrophil accumulation through reduced expression of adhesion molecules or cytokine expression from macrophages, lymphocytes, monocytes, fibroblasts, and eosinophils (10). The treatment effects of macrolides in DPB have been reported independent of the presence or absence of Pseudomonas infection, and the treatment effect can be observed below the minimum inhibitory concentration of macrolides, (10, 11) suggesting that immune modifying effects of macrolides are crucial for management of DPB.
Previously, the lower airway has been regarded as a bacteria-free area, but recent data show that bacterial colonization can occur in asthma (12, 13) and chronic obstructive pulmonary disease (COPD) (14). These bacteria may exacerbate chronic airway diseases (14). In addition to their immune-modifying effects, macrolides have anti-microbial properties that may play a role in the management of other chronic airway diseases, such as asthma, COPD (15), cystic fibrosis, and chronic rhinosinusitis (16). For cystic fibrosis patients on long-term macrolide treatment, the prevalence of sputum culture positivity for Haemophilus influenzae and Streptococcus pneumoniae are markedly decreased, although positive rates of these bacteria with macrolide resistance are much higher (17, 18). Decreased bacterial burden may contribute to the effect of long-term treatment of macrolides. Emergence of macrolide-resistant bacteria is an important concern related to the long-term administration of macrolides, but no cases have been reported in which macrolide-resistant bacterial infection led to a life threatening episode (2). In conclusion, it is essential to consider DPB for treatment resistant asthmatics in East Asian patients. DPB can be treated well by long term use of clarithromycin.



 XML Download
XML Download