

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute gout and septic arthritis are the major diseases that should be suspected in patients presenting as acute monoarthritis (1). The differential diagnosis of these two diseases is important because incorrect diagnosis and misled treatment can lead to undesirable outcomes such as joint destruction or unnecessary surgical debridement. However, differentiating acute gout from septic arthritis can be difficult on clinical examination since they are clinically similar. Both of these two diseases commonly involve a single joint and accompany severe joint inflammation. Septic arthritis often accompany systemic features such as fever and chilling (1), which can also be seen in patients with gout, though they are not as common in gout as in septic arthritis. Diagnosis of both gout and septic arthritis can be established by synovial fluid analysis: demonstrating monosodium urate crystal (MSU) for gout by a polarized microscope and bacteria by Gram staining or culture in the case of septic arthritis. However, synovial fluid analysis is often impractical in real practice and the differential diagnosis between gout and septic arthritis might be problematic without the help of synovial fluid analyanalysis. Recently, a novel diagnostic rule for acute gout without joint fluid analysis was introduced and showed a good performance in predicting the possibility of gout (2). However, the first study validating this rule included only 2 cases with septic arthritis. We applied this diagnostic rule to the patients with gout and those with septic arthritis and determined whether this rule properly diagnoses gout and excludes septic arthritis in the setting of acute monoarthritis.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the medical records of adult (age > 18 yr) patients who were diagnosed with acute gout or septic arthritis between January 2006 and December 2012 in Dongguk University Ilsan Hospital in Goyang, Korea. We searched in the electronic medical recording system for patients with an International Classification of Diseases (ICD)-10 code of gout (M10) or pyogenic arthritis (M00). After searching for such cases, in order to secure the certainty of diagnosis, we excluded patients who did not undergo synovial fluid analysis and only included those who were diagnosed by synovial fluid analysis (presence of monosodium urate [MSU] crystal in the case of gout and presence of bacteria in Gram stain or culture in the case of septic arthritis), which are the gold standards in the diagnosis of these two diseases.
Diagnostic rule
The diagnostic rule proposed by Janssens et al. (2) gives different scores to 7 clinical and laboratory variables: male sex=2, previous patient-reported arthritis attack=2, onset within a day=0.5, joint redness=1, 1st metatarsophalangeal (MTP) joint involvement=2.5, hypertension or at least one cardiovascular disease=1.5, serum uric acid level greater than 5.88 mg/dL=3.5. The probability of acute gout is high if the sum of the scores is 8 and over, intermediate if between 4 and 8 and low if below 4. We scored the patients in these two groups (acute gouty arthritis and septic arthritis) based on this diagnostic rule and classified them into 3 groups (high, intermediate and low probability of gout) according to their total scores.
Evaluation of the performance of the diagnostic rule
To evaluate the performance of this diagnostic rule, we compared the mean total scores and the proportion of the 3 gout probability groups of each group (gout and septic arthritis) and assessed the significance of the association between the 3 gout probabilities and the actual diagnosis (gout or septic arthritis) by eta statistics which is useful in evaluating the associations between binominal and polynominal variables. Positive predictive value (PPV) and negative predictive value (NPV) were calculated for high probability (≥8) and low probability (<4) score, respectively. The area under the receiver operating characteristic (ROC) curve for the diagnostic rule was calculated. Additionally, we conducted a sub-analysis excluding cases with podagra to determine whether this diagnostic rule performs well even in such a situation.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0. Student's t-test was used to compare continuous variables, Mann Whitney-U-test to compare nonparametric variables and chi-square test and eta (η) statistics to assess the association between ordinal (gout probability) and nominal (gout and septic arthritis) variables.
RESULTS
Patient characteristics
There were several significant clinical and laboratory differences between patients with gout and septic arthritis as shown in Table 1. Patients with acute gout were significantly younger, more likely to be male, and had higher levels of serum uric acid with the first MTP joints affected more frequently compared to those with septic arthritis. Patients with septic arthritis had significantly higher levels of inflammatory markers (erythrocyte sedimentation rate and C-reactive protein) and white blood cell count with knee joints most frequently affected compared to those with gout. The positive rates of the 7 variables of this diagnostic rule in each group are presented in Table 2.
Discrimination between acute gouty arthritis and septic arthritis
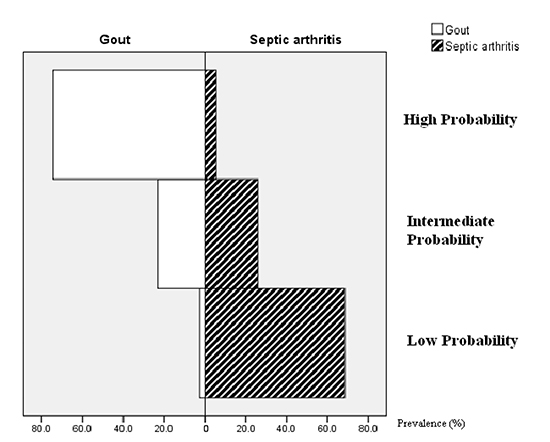
As shown in Table 3, the mean total score of the patients with acute gout was significantly higher than that of those with septic arthritis (8.6±0.2 vs. 3.6±0.32, P<0.001). In 82 patients with acute gout, the diagnostic rule classified 61 (74.4%) patients as high, 19 (23.2%) as intermediate and 2 (2.4%) as low probability, whereas in 54 patients with septic arthritis, it classified only 3 (5.6%) as high, 14 (25.9%) as intermediate and 37 (68.5%) as low probability. A histogram for this result is presented in Fig. 1. If these two groups are taken together, the prevalence of gout, as confirmed by the presence of MSU crystal, was 95.3% (61/64), 57.5% (19/33) and 5.1% (2/39) in high, intermediate and low gout probability group, respectively. PPV for high probability score (≥8) was 95.3% and NPV for low probability score (<4) was 94.8%. Patients with gout had more 'high' and less 'low' probabilities than those with septic arthritis and this association was statistically significant (eta=0.776). The area under the ROC curve for the diagnostic rule was 0.933 (95% confidence interval, 0.895-0.972).
Discrimination between gout without the first MTP involvement and septic arthritis
Acute monoarthritis involving the first MTP joint can easily be diagnosed as gout and be distinguished from septic arthritis. To examine whether this diagnostic rule performs well even in patients without the first MTP involvement, we excluded patients with a podagra and performed the same analysis. Of the 46 patients with acute gout without the first MTP involvement, 28 patients had arthritis in the knee, 17 in the ankle and 1 in the tarsal joint. As shown in Table 2, the diagnostic rule showed similar performances. The PPV for high probability score was 90.3% and the NPV for low probability score was 94.8%.
DISCUSSION
In this study, the diagnostic rule properly predicted the possibility of acute gout among patients with gout and those with septic arthritis in the setting of acute monoarthritis. It also discriminated acute gout and septic arthritis fairly well since most of the patients with septic arthritis were, at least, not classified as high probability group. The sub-analysis excluding cases with a podagra, a situation which may confuse physicians, also demonstrated similar performances.
The performance of the extremes of this diagnostic rule (high and low probability) was powerful. The PPV for high probability score was 95.3%, which demonstrates its usefulness in diagnosing gout. However, it should be noted that the rule classified 3 cases with septic arthritis as high probability group. The NPV for low probability score was 94.8%. This suggests that the rule may be useful in excluding gout from septic arthritis.
The proportion of intermediate probability group was 24.2% and the prevalence of gout in the intermediate probability group was 57.5%. It is uncertain whether patients with scores within these ranges may have gout or not and a considerable number of patients with septic arthritis are included in this group. Therefore, within the framework of differential diagnosis between gout and septic arthritis, patients with intermediate scores should undergo further investigations such as synovial fluid analysis.
Differentiating gout and septic arthritis in the setting of acute monoarthritis on a clinical basis can be difficult because both gout and septic arthritis frequently involve a single joint and accompany severe joint inflammation. Several predisposing factors for septic arthritis such as age greater than 80 yr, diabetes mellitus, rheumatoid arthritis, prosthetic joint, and previous intra-articular corticosteroid injection were identified, but they have only a modest impact on the risk of septic arthritis (4, 5). There were also significant differences between patients with gout and those with septic arthritis in the baseline characteristics in this study. However, these differences are insufficient evidences to establish the diagnosis.
The diagnostic rule showed proper performances in the differential diagnosis between gout and septic arthritis especially in the case of high and low probability score. This rule may particularly be helpful in conditions where a physician encounters a patient with acute monoarthritis in whom gout is suspected, but septic arthritis cannot be ruled out, and vice versa. High probability scores would support the possibility of gout, whereas low probability scores would support non-gout diagnosis, which is septic arthritis in this study. Patients with intermediate probability scores may not benefit from this diagnostic rule because both diseases are possible. Of note, it should be noted that septic arthritis, a medical emergency which should never be missed, was present in all possibility groups. The diagnostic rule may aid the physician to reach the correct diagnosis, but cannot be diagnostic references.
Several classification criteria for gout have been developed since the 1960s. The early ones of Rome and New York criteria (6) deal with key features of gout, but were not based on prospective data and tested to a limited extent. In addition, confirmation of MSU was one of the items of the Rome criteria. The American College of Rheumatology (ACR) criteria (7), which were introduced in 1977, comprise several clinical and radiologic variables and do not require confirmation of MSU. However, 1977 ACR criteria chose the physician diagnosis of gout as the gold standard and showed limited performance in the external validation studies using MSU crystal confirmed cases (8, 9). Recently, the ACR criteria was modified by Pelaez-Ballestas et al. (10) based on the frequency of the items of ACR criteria and the modified criteria showed better performance compared to the ACR criteria. However, they had limitations such as that the non-gout controls did not undergo synovial fluid analysis and that the rate of tophi in the gout cases was relatively high (81%).
The diagnostic rule proposed by Janssens et al. does not require synovial fluid analysis, comprises simple clinical and laboratory variables, the information of which can easily be obtained in primary care settings. It showed good performances in predicting the possibility of gout in the setting of acute monoarthritis in primary care setting (2). The prevalence of gout, as confirmed by the presence of MSU crystal, was 82.5%, 31.2%, and 2.2% in high, intermediate and low probability group, respectively. It was recently evaluated in a secondary care setting and also showed proper performances. The PPV of high probability score was 87% and the NPV was 95%, which is similar to our results (11).
This study has several limitations. First, this study was retrospective in nature and it is not clear how patients were indicated to undergo synovial fluid analysis, which suggests that this study may have a risk of a selection bias. Second, the number of subjects included was relatively limited. Thirdly, the conclusions may be limited to the findings of this study. The setting was a tertiary referral medical center and the patient selection was very specific based on synovial fluid diagnosis. Further studies may be needed in the future dealing with other situations related with this issue: concurrent cases with both gout and septic arthritis or cases with synovial fluid analysis results negative for MSU or bacteria.
In this study, the diagnostic rule proposed by Janssens et al. showed a good performance in predicting the possibility of gout and discriminating it from septic arthritis. Though the rule is not an absolute standard, it might be a useful tool in distinguishing these two diseases in the absence of a polarized microscope.

 XML Download
XML Download