

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Staphylococcus aureus (S. aureus) is known to be a major cause of skin and soft tissue infections, pneumonia, bloodstream infections, and infective endocarditis via nosocomial transmission in hospitals (1). In otorhinolaryngology, S. aureus infection has become a great concern due to its ease of its propagation via medical appliances used to evaluate the nasal and oral cavities (2). In previous studies, the prevalence of S. aureus in ear discharge was reported to range from 9.9% to 54.1%, while that of methicillin-resistant S. aureus (MRSA) isolates ranged from 0.3% to 24.8% (3, 4). Recently, reports of MRSA infections, including hospital-acquired MRSA and community-acquired MRSA, in patients with continuous otorrhea have greatly increased in number. In the past, MRSA was mainly treated using antibiotics of the glycopeptide family such as vancomycin or teicoplanin; however, the MIC of MRSA has recently increased beyond what was observed in the past (5).
Arbekacin, a broad-spectrum antibiotic of the aminoglycoside family, has been shown to be effective against the various aminoglycoside-modifying enzymes found in MRSA (6, 7) and to exert a longer post-antibiotic effect than that observed with vancomycin. Aminoglycosides are able to pass through the biological membranes of renal tubular cells and inner ear cells and have been empirically used to treat otitis media, despite reports of adverse reactions such as ototoxicity and nephrotoxicity (8). Aminoglycoside ototoxicity was previously shown to occur due to the high concentrations and long retention of antibiotics in inner ear fluids (3, 8, 9).
Despite its pharmacokinetic advantages, the use of arbekacin to treat chronic suppurative otitis media (CSOM) caused by MRSA has not yet been sufficiently investigated in clinical trials. Accordingly, we attempted to evaluate the clinical usefulness of arbekacin in treating CSOM due to MRSA, comparing its clinical efficacy and safety with those of vancomycin.
MATERIALS AND METHODS
Study design
A case-control study was done at Chonbuk National University Hospital, in Jeonju, Korea. Adult patients with CSOM caused by MRSA who received arbekacin or vancomycin from January 2003 to December 2011 were enrolled. The aim of this study was to analyze the efficacy and safety of arbekacin compared to vancomycin. Clinical data were collected from electronic medical records, including sex, age, clinical diagnosis, underlying disease, bacteriologic isolates with antibiotic susceptibility, previous/concomitant antibiotic use, antibiotic duration, laboratory findings, operation, and adverse reactions. This study describes in detail both patient demographics and clinical characteristics according to the most recently published STROBE statement checklist (10).
General characteristics of the study population
Efficacy was classified according to bacterial elimination (BE) or bacteriologic failure (BF) and improved or failed clinical efficacy response (CER). BE was defined as no growth of MRSA or an absent culture due to being cured or having an improved health status, while BF was defined as persistent MRSA growth after appropriate antibiotic therapy. Improved CER was defined as the absence of signs and symptoms of otorrhea, otalgia, and hearing impairment related to ear infection with no worsening or appearance of new signs or symptoms of ear infection. CER failure was defined as persistent signs or symptoms of otorrhea, otalgia, and hearing impairment, as well as the appearance of new signs or symptoms associated with ear infection (11).
Underlying diseases in the patient cohort included cardiovascular disease, cancer, diabetes mellitus, and pulmonary disease. Gastric cancer, cervical cancer, and bladder cancer were also included. Chronic obstructive pulmonary disease, asthma, hypertension, and myocardial infarction were included in this study.
At least a 50% reduction in glomerular filtration rate (GFR) using the abbreviated modified diet in the renal disease equation was defined as nephrotoxicity (12). A white blood cell count of less than 4.8×103/µL during treatment was defined as leukopenia. Elevation in aspartate aminotransferase/alanine aminotransferase (AST/ALT) levels of more than two times the baseline values during treatment was defined as hepatotoxicity. Fever coinciding with the administration of a drug and disappearing after the discontinuation of the drug was defined as drug fever (13).
Bacterial study and therapeutic regimens
We identified the bacterial strains and evaluated their antimicrobial susceptibility based on minimum inhibitory concentration (MIC) from the culture using standard methods with the Vitek 2 (bioMeriux Vitek Inc., Hazelwood, MO, USA) automated system. Antimicrobial susceptibility was determined according to the criteria defined by the Clinical and Laboratory Standards Institute (CLSI).
S. aureus was cultured, and the minimum inhibitory concentration was determined according to results from the Vitek 2 automated system. The therapeutic regimens were as follows: arbekacin, 100 mg two times intravenously (iv) (200 mg/day, 19/20, 95%) or 100 mg three times by iv (300 mg/day, 1/20, 5%); vancomycin, 1,000 mg twice by iv (2,000 mg/day, 35/36, 97.2%) or 1,000 mg once by iv (1,000 mg/day, 1/36, 2.8%).
Statistical analysis
The chi-squared test or Fisher's exact test was used to compare categorical variables, and the Mann-Whitney U test was used for continuous variables. The laboratory results obtained before and after treatment among the two groups were compared using the repeated measure analysis of variance (ANOVA). To conduct all analyses, we used SPSS software (20.0 version), and P values of less than 0.05 were considered statistically significant.
RESULTS
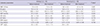
During the study period, a total of 1,760 adults over 18 yr old were diagnosed with otitis media. Among them, 95 subjects (5.4%) were diagnosed with MRSA-infected CSOM. Twenty of these subjects were treated with arbekacin, and 36 received treatment with vancomycin (Table 1). Therefore, a total of 56 subjects with otitis media were included.
The mean age of the arbekacin group was 59 (36-76) yr, and that of the vancomycin group was 53 (24-73) yr (P=0.082). The presence of one or more underlying diseases was more common in the arbekacin group (70%, 14/20) than in the vancomycin group (38.9%, 14/36, P=0.026).
Clinical status was classified as CSOM either with cholesteatoma or without cholesteatoma (P=0.686). The previous antibiotics used included aminoglycosides, quinolones, cephalosporins, and penicillin, and did not differ between the two groups (P=0.357).
Concomitant antibiotic treatment was undertaken in 4/20 cases (20.0%) in the arbekacin group and in 13/36 cases (36.1%) in the vancomycin group (P=0.209). Polymicrobial infections occurred in 3/20 cases (15.0%) in the arbekacin group and in 4/36 (11.1%) in the vancomycin group (P=0.691). For median medication duration, subjects in the arbekacin group received medication for 9 (4-42) days and those in the vancomycin group did so for 10 (4-27) days (P=0.324). The success rate of TM graft was not statistically different between the two groups (arbekacin vs. vancomycin; 85% (17/20) vs. 75% (27/36), P=0.999).
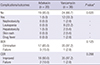
Laboratory findings from both before and after treatment are summarized in Table 2. No statistically significant difference was found between the two groups. MIC results are shown in Table 3. The operations in the patients who received surgery were tympanoplasty [arbekacin vs. vancomycin group, 16/20 (80%) vs. 33/36 (91.7%)], tympanomastoidectomy [3/20 (15.0%) vs. 6/36 (16.7%)], and tympanoplasty with ossiculoplasty [vancomycin only, 2/36 (5.6%)].
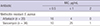
Complications during the medication period were more common in the vancomycin group (33.3%, 12/36) than in the arbekacin group (5.0%, 1/20) (P=0.020). In addition, a total of 12 adverse reactions were found, including two instances of hepatotoxicity, one of nephrotoxicity, eight leukopenia, two skin rashes, and one case of drug fever in the vancomycin group (Table 4). Only one patient was treated with alternative antibiotics because of an adverse reaction in the vancomycin group.
The BE of the arbekacin and vancomycin groups were 85.0% and 97.2%, respectively (Table 4). The BE of the arbekacin group was 12.2% lower than that of the vancomycin group, but this was not statistically significant (P=0.125). In addition, the CER of the arbekacin group (90.0%) was slightly lower than that of the vancomycin group (97.2%), but, again, this was not significant (P=0.288).
DISCUSSION
MRSA is a major cause of ear infections, and treatment with an appropriate antibiotic is highly important. In this study, we demonstrated a better therapeutic value for arbekacin in comparison to vancomycin for treating CSOM. Although the BER and CER were not statistically different between the two groups (arbekacin vs. vancomycin), we observed fewer adverse reactions in the arbekacin group. These results suggest that arbekacin may be a good alternative drug to vancomycin for the treatment of MRSA-infected CSOM. In clinical settings, less frequent use of vancomycin may facilitate decreases in the appearance of vancomycin-resistant strains such as vancomycin-intermediate S. aureus (VISA) and vancomycin-resistant Enterococcus (VRE).
MRSA isolation rates among S. aureus ear infections have consistently increased from 47.5% (1997), 63.4% (2004), to 60.9% (2008) (14, 15, 16). These MRSA strains are resistant to many antibiotics such as β-lactam antibiotics, aminoglycosides, macrolides, tetracycline, and chloramphenicol. In addition to vancomycin-resistant S. aureus, VRE is common in clinical settings in all over the world (17, 18). Nevertheless, vancomycin is routinely used as an antimicrobial agent for treating MRSA, the usage for which has greatly increased (19).
Vancomycin, which is characterized by its narrow therapeutic index, has been shown to cause severe adverse reactions such as local thrombophlebitis, nephrotoxicity, red-man syndrome, ear toxicity, and severe allergy, necessitating therapeutic drug monitoring to reduce its potential toxicity (20). In addition, muscle injection of vancomycin is not feasible due to tissue reaction (21). For these reasons, treatment of CSOM due to MRSA is quite difficult (14, 15, 16), which has heightened the need for new antibiotics choices.
As an alternative treatment, arbekacin has been used to control MRSA. Arbekacin is used to treat MRSA infections in combination with vancomycin or as single therapy because the majority of MRSA isolates in Europe and Japan are susceptible to arbekacin (17, 22, 23, 24). MRSA was reported 100% sensitive to arbekacin in a university hospital in Korea, similar to findings from other reports (25, 26, 27, 28). The bactericidal activity of arbekacin depends more on the drug concentration to quell infections, compared to the time-dependent antibiotic effect of vancomycin. Although these studies demonstrated the usefulness of using arbekacin at a high concentration to treat MRSA infections, further clinical studies on efficacy and safety are required. Accordingly, in a previous retrospective study, the improved efficacy and safety of arbekacin in comparison to vancomycin were documented in the treatment of MRSA infections. In addition, significantly fewer adverse reactions were recorded in the arbekacin group (15.1%) than in the vancomycin group (32.9%) (P=0.019) (29).
We also previously observed statistical differences in the indications for treatment with arbekacin and vancomycin in age- and sex-matched groups. Investigating further, we conducted a study of skin and soft tissue infections due to MRSA. The results of that study with regard to the clinical and bacteriological efficacy were not different between the two groups; however, adverse reactions were less commonly reported in the arbekacin group (30).
Based on our previous studies, we conducted the present retrospective cohort study to evaluate the efficacy and safety of arbekacin in the treatment of CSOM due to MRSA. Arbekacin exerted similar effects to that of vancomycin in regards to its clinical efficacy; moreover, it led to fewer adverse reactions than vancomycin. Underlying diseases, polymicrobial infections, concomitant antibiotic use, duration of treatment, laboratory findings, and operation methods did not differ between the two groups. In this study, only one case from the vancomycin group had treatment discontinued due to an adverse reaction. The patient had acute kidney injury and was changed to treatment with teicoplanin. There were no specific adverse reactions recorded in the arbekacin group.
In conclusion, arbekacin, which has an efficacy similar to vancomycin, is safer than vancomycin in treating patients with CSOM caused by MRSA. Arbekacin is a promising antibiotic in treatment of the CSOM caused by MRSA.

 XML Download
XML Download