

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neisseria meningitides (NM) causes life-threatening infections, such as meningitis and septicemia (1). The meningococci are transmitted exclusively from human-to-human by direct contact through respiratory droplets and have the capacity to spread rapidly in crowded settings (2). Secondary cases and outbreaks are predicted to follow index cases, especially among high-risk groups. Young adults living in communal settings, such as military bases, are at a high risk for meningococcal diseases (1). Therefore, all Korean young adult males who are in obligatory military training would be exposed to an increased risk for meningococcal infections (3). Herein, we report three consecutive cases of meningococcal disease, at a military training base in April 2011 that were caused by NM serogroup W-135, which is novel sequence type ST-8912. These cases demonstrate the need for systemic epidemiologic investigations of meningococcal diseases among military populations.
CASE DESCRIPTION
Case 1
In late April 2011, a 19-yr-old male military recruit at his 4th week in the Korea Army Training Center in Nonsan, Chungcheongnamdo, Korea, arrived at the emergency room (ER) presenting with fever, headache, and mental deterioration. He had experienced a cough, myalgia, and fever for one day at the military base, at which point he visited the military district hospital. His vital signs were unstable and he was referred to our hospital that same day. At the ER, he had a temperature of 36℃, blood pressure of 130/80 mmHg, pulse rate of 84/min, and respiratory rate of 22/min. Multiple purpuric spots were present on his trunk and lower extremities. Laboratory analytical results on admission were as follows: 20,400 leukocytes/µL with 90% neutrophils, hemoglobin 11.1 g/dL, platelets 75,000/µL, and C-reactive protein (CRP) 12.8 mg/dL. In the cerebrospinal fluid (CSF), leukocytes were 21,708/µL with 90% neutrophils and the glucose level was < 1.0 mg/dL. With a presumptive diagnosis of meningococcal meningitis after blood and CSF culture, intravenous ceftriaxone was initiated. Five hours post-presentation, the patient was transferred to another hospital on parental request. Gram staining and antigen detection of CSF were negative and no microorganisms were cultured from his CSF and blood. Later on, we were notified that he was discharged without any complications.
Case 2
Two days after the first case, a 21-yr-old male recruit in a different regiment from the same military training base was admitted to our hospital, presenting with high fever, purpura fulminans, and a confused mentality. He had shown symptoms of an upper respiratory tract infection for more than 10 days. He joined the military march training one day prior to admission, despite progressive myalgia. At admission, he had a blood pressure of 100/70 mmHg, temperature of 38.8℃, heart rate of 134/min, and respiratory rate of 24/min. Laboratory tests showed 2,500 leukocytes/µL (67% segmented, 14% band neutrophils), platelets of 78,000/µL, and a CRP of 6.6 mg/dL. CSF analysis showed 42 leukocytes/µL (95% neutrophils), protein 18 g/dL, and glucose 66 mg/dL. Physical examination revealed nuchal rigidity. Soon after blood and CSF sampling for bacterial culture, a ceftriaxone injection was initiated based on a suspicion of meningococcal meningitis. Eight hours after the admission, he suddenly had asystole and cardiopulmonary resuscitations were unsuccessfully performed four times. He expired within 16 hr of hospitalization. Two days after his death, Gram-negative diplococci were observed in his blood and CSF.
Case 3
Six days after the index case, a 20-yr-old male military recruit was admitted to the ER presenting with fever and headache, which he had experienced for more than 24 hr. He was from the same military training base, but in a different regiment from the previous two patients. He had been in training for one month. The patient was alert and had no acute distress. Presenting symptoms included a generalized maculopapular rash with some hemorrhagic transformation on his entire body. The doctor at Nonsan Army Hospital made a presumptive diagnosis of meningococcal disease and injected ceftriaxone before the patient was transferred to our hospital. The patient's vital signs on admission to our hospital were as follows: body temperature 36.7℃, blood pressure 80/50 mmHg, heart rate 60/min, and respiratory rate 20/min. Initial laboratory test results were as follows: 22,900 leukocytes/µL with 90.6% neutrophils, hemoglobin 12.8 g/dL, and platelets 213,000/µL. There was no evidence of meningitis. Antibiotic treatment was continued as it had been in the two previous patients. He was hospitalized for 15 days and discharged without any residual complications. No microorganisms were cultured from his CSF and blood.
The samples of serum and CSF from all three patients, and the two isolates from the second patient's blood and CSF were forwarded to the Korea Centers for Disease Control and Prevention (CDC) for further analysis. Identification of the organism and serogrouping were performed by polymerase chain reaction (PCR). NM serogroup W-135 was identified from the sera and CSF, by real-time PCR for sodC and serogroup-specific PCR targeting synG (4, 5). We confirmed NM serogroup W-135 as the etiological organism in the three cases.
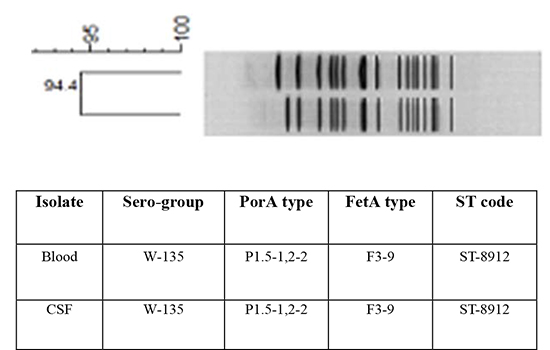
The two isolates from the second patient were analyzed for antimicrobial susceptibility and molecular typing characterization. Multilocus sequence typing (MLST), sequencing of the outer membrane proteins PorA and FetA, and pulsed-field gel electrophoresis (PFGE), were performed to define the clonal complex and the subtype, according to described methods (6, 7). These strains showed full susceptibility to ceftriaxone, levofloxacin, azithromycin, and rifampicin, and intermediate susceptibility to penicillin. The MLST analysis showed a novel sequence type, ST-8912, with an undetermined clonal complex. The PFGE patterns of these isolates showed ≥94% homology (Fig. 1). By the molecular characterization, these two strains were designated as W-135:P1.5-1,2-2:F3-9:ST-8912.
DISCUSSION
We have described 3 cases of meningococcal disease caused by the NM serogroup W-135, which occurred within a one-month span at a military training camp. The first patient had meningitis, the second had septicemia and meningitis, and the third had no definite septicemia or meningitis. NM W-135 was detected from the blood and CSF in all three cases by PCR. The presenting symptoms of the three patients were nonspecific, including headache and fever. The time from the initial presentation to the first dose of antibiotics ranged from 1-10 days. One of the three patients died within the first day of hospitalization. This patient had the longest time delay between the onset of symptoms and antibiotic administration. We supposed that he could have mistakenly regarded his symptoms as fatigue from military training.
Meningococcal disease is legally mandated to be reported in Korea. However, the data on incidence rate and serogroup distribution of the disease in Korea are very limited. The rate of the disease reporting is very low and most of the reports lack information on the causative organism. This is a cumulative result of the difficulty in diagnosis and in obtaining adequate samples for culture, along with the common use of antibiotics prior to sample collection. It is likely that the true burden of disease is underestimated in Korea. During the decade from 1991 to 2001, 2 to 13 probable cases of meningococcal disease were reported annually (8). The number of cases dramatically increased in 2002 and 2003, to 27 and 38 cases, respectively. During this period, 9 organisms were isolated from clinical samples, of which 7 were serogroup Y, while one was serogroup B and one was serogroup 29E (6). The calculated incidence rate was 0.06-0.08 per 100,000 population (9). After the peak occurrence in 2003, the number of cases decreased to about 10 cases per year. Between 2004 and 2012, the incidence rate was 0.00-0.02 per 100,000 population (8).
In the Korean Army, epidemiologic data on meningococcal disease are incomplete. There have been several studies about the meningococcal pharyngeal carrier rate in military bases, including meningococcal disease cases. During April 1988 to January 1990, there were 13 cases (seven probable and six confirmed) in Armed Forces Capital Hospital or Nonsan Military Hospital (10). Of them, 7 cases resulted in death, leading to a case fatality rate of 53.8%. NM was grown from the blood of two cases but serogroup was not determined. From 1988 to 1992, there were 18 cases (eight probable and ten confirmed) in the Korean Army with a 50.0% mortality rate (nine patients died) (11). The annual incidence rate was 0.5-1.3 per 100,000 soldiers, and 56% of these cases occurred in the Nonsan Army Training Center, where the annual incidence rate was 0.8-3.3 per 100,000 recruits (11). Also in this study, causative serogroup was not determined. Lee et al. (3) reported 12 cases of meningococcal disease in the Korean Army from August 2000 to July 2001; one case had serogroup A, three cases had serogroup C, and the others were not identified. In this study, there was an annual incidence of 2.2 per 100,000 among 550,000 soldiers.
NM W-135 has been known to be rare and to be associated with sporadic cases. Two Hajj-associated outbreaks of NM W-135 occurred in 2000 and 2001, for which NM W-135 of ST-11 was responsible (12). In 2002, the first large-scale outbreak of W-135 meningococcal disease occurred in Burkina Faso, with more than 12,000 reported cases, resulting in 1,400 deaths (13). In Asian areas, there has been scarce data about NM W-135. In Singapore, W-135 meningococcal disease was first imported via Hajj pilgrims in 2000 (14). In Taiwan, NM W-135 was the second most common serogroup after serogroup B, was of ST-11 (15). However they were introduced before the Hajj pilgrimage outbreak and was found to be genetically distinct from the Hajj-related strain in 2000 (15). To date in Korea, only three publications have studied the serogroup data in meningococcal disease, of which there were no reported W-135 cases (3, 6, 16). During 2000-2001, the Korean Army reportedly had one of 12 cases was identified as serogroup A and three cases of serogroup C (3). During 2002-2003, of nine clinical isolates by Korean CDC, seven were serogroup Y, with one each of serogroups B and 29E (6). In a prospective surveillance among children <5 yr between 1999 and 2001, 92 cases of NM meningitis were confirmed by PCR. Among them, 16 cases could be serogrouped and one of them was serogroup C, nine of them were serogroup X, and six of them were serogroup Y (16). Although several NM carrier studies have been done on NM serogroups including NM W-135, as far as we know, this is the first report about invasive meningococcal disease by W-135 in this country. The ST-8912 identified in our report has never been identified before, and its clonal complex has not yet been determined. More data about serogroup and molecular characterization of the meningococcal disease is needed to know the implications of W-135 and the new sequence type ST-8912 in Korea.
In Korea, where military service is mandatory for all men, these consecutive cases in 2011 raised public awareness of the elevated risk for disease at the military training bases. Consequently, the Korean government issued that quadrivalent (A/C/Y/W-135, Menveo®) meningococcal vaccination to all recruits in basic military training starting in November 2012 (17). However, meningococcal epidemics in military bases are an ongoing problem in Korea. The intensive physical training and various environmental conditions may lead to delays in diagnosis and treatment, leading to a negative impact on survival. Also, the currently available quadrivalent vaccine does not protect against serogroups other than A, C, Y, and W-135. Organism isolation and strain typing are essential to assess the epidemiologic link among the isolates. This report demonstrated that improved case diagnosis and serologic and epidemiologic surveillance of the disease are required to monitor the disease trends as well as to evaluate the efficacy of newly adapted vaccines in the Korean Army.

 XML Download
XML Download