

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Postoperative nausea and vomiting (PONV) is a major concern in patients undergoing general anesthesia, increasing patient discomfort even occasionally more than postoperative pain, delaying discharge and increasing costs. Because inhalation anesthetic agents are well-known to contribute to PONV (1), total intravenous anesthesia (TIVA) is preferred (2) with propofol/remifentanil most commonly used as hypnotic/analgesic combination for better hemodynamic and surgical status (3, 4, 5). While propofol is a well-known anti-emetic agent, the opioid remifentanil, despite rapid clearance, might cause PONV (6) although studies have shown inconsistent results (7, 8, 9, 10). Opioids act through the human µ-opioid receptor, and the A118G mutation is one of the most common single nucleotide polymorphism (SNP) in the µ-opioid receptor gene (OPRM1).
Based on the known value of genetic profiling (11), we hypothesized that genetic variation in opioid receptor might underlie inconsistency in PONV occurrence in patients undergoing general anesthesia with remifentanil. This study therefore investigated association between PONV and A118G SNP with type distribution of the latter in Korean female adults undergoing breast surgery under general anesthesia with remifentanil.
MATERIALS AND METHODS
Study population
All patients provided written informed consent, and the study was conducted in a prospective, blind and randomized fashion. Korean adult female patients with American Society of Anesthesiologists physical status classification I undergoing local breast excision under general anesthesia were enrolled. The patients were excluded if any of the following criteria were present: 1) age <20 yr, 2) re-do case, 3) other concurrent surgery, 4) allergy to egg or soybean oil, 5) history of drug abuse, 6) on medications, and 7) demand of patient-controlled analgesia (PCA). Using a randomized parallel study design, patients were allocated 1:1 before anesthesia induction to receive either TIVA (T group) or inhalation anesthesia (I group) using sealed envelopes. All data collection were done by trained observers who did not involve in patient care and were blinded to the study.
Anesthetic technique
The anesthetic technique used throughout the study was standardized and as follows. The patient had been on no pre-anesthetic medications. After routine non-invasive patient monitoring (pulse oximetry, electrocardiography, systemic blood pressure monitoring, and bispectral index [BIS]), anesthesia was induced. The anesthesiologists who were blinded to the study were requested to anesthetize the patients as described below. Lidocaine 0.5 mg/kg was administered for decreasing the pain induced by propofol. T group was anesthetized as follows. An initial target concentration of propofol 4 µg/mL (effect-site, modified Marsh model with a ke0 of 1.21/min) (12) and the fixed target concentration of remifentanil 10 ng/mL (plasma-site, Minto model) (13, 14) were administered using a target-controlled infusion device (TCI, Orchestra® Base Primea, Fresenius Vial, Brezins, France). The target concentration of remifentanil 10 ng/mL was achieved and maintained during anesthesia. An initial target concentration of propofol was titrated to maintain BIS values between 40 and 60. The I group was anesthetized as follows. Propofol 2 mg/kg was slowly injected for anesthesia induction and the fixed target concentration of remifentanil 10 ng/mL was administered using a TCI as for the T group. An initial end-expiratory concentration of sevoflurane 1.0 vol% was administered with a vaporizer and titrated up or down by 0.1 vol% to maintain BIS values between 40 and 60. Rocuronium 0.6 mg/kg was administered for muscle relaxation after loss of consciousness under the guidance of peripheral neuromuscular transmission (NMT) monitoring. Tracheal intubation was performed when remifentanil 10 ng/mL was achieved and train-of-four count was 0. TCIs of propofol and remifentanil in T group, and vaporizer of sevoflurane and TCI of remifentanil in I group were stopped after surgical procedure and skin dressing. Ketorolac 0.5 mg/kg was intravenously injected for postoperative pain control. Residual neuromuscular paralysis was antagonized with neostigmine 0.05 mg/kg and glycopyrrolate 0.01 mg/kg under the guidance of peripheral NMT monitoring. After tracheal extubation, patient was transferred to post-anesthetic care unit (PACU).
Genotyping assays
Blood specimens were collected after anesthesia induction and A118G SNP analyzed. Genomic DNA was extracted from the blood specimen using Qiagen DNeasy Blood & Tissue Kit (Cat. 69504, QIAGEN Inc., Alamaeda, CA, USA). A118G SNP genotypes were determined by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) analysis. PCR was performed using a set of primers (5'-GGTCAACTTGTCCCACTTAGATCGC-3' and 5'-AATCACATACATGACCAGGAAGTTT-3') to amplify A118G SNP (193 bp). Template DNA (50 ng) and 20 pM of each primer were added to a PCR mixture tube (AccuPower PCR PreMix, Bioneer, Korea), which contained 1 U of Taq DNA polymerase, 250 µM of each dNTP, 50 mM of Tris-HCl (pH 8.3), 40 mM of KCl, 1.5 mM of MgCl2, and gel loading dye. The volume was adjusted with distilled water to 20 µL. The reaction mixture was subjected to 30 cycles of amplification (30 sec at 94℃, 1 min at 60℃ and 1 min at 72℃) , followed by a 5 min extension at 72℃ (Veriti 96 well thermal cycler).
8 µL of PCR product was digested for 12 hr at 37℃ with 20 U Bsh126I enzyme (Cat. ER0922, Thermoc Scientific, Waltham, MA, USA) and electrophoresed on a 4% agarose gel (Roche). A118G SNP was analyzed by restriction patterns; the homozygous type (AA) was 193 bp, the heterozygous type (AG) was 193 bp, 169 bp, and 24 bp, and the homozygous type for the G allele (GG) was 169 bp and 24 bp. The results for each genotype were confirmed in randomly selected individuals by direct sequence analysis.
Measurements of nausea and vomiting
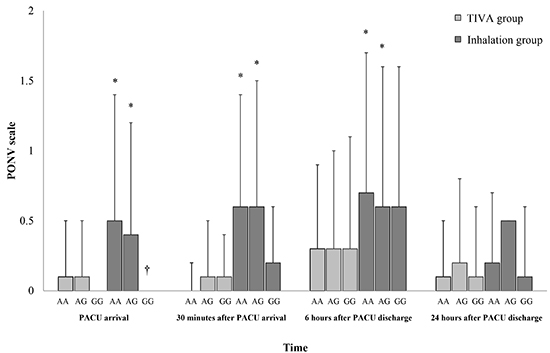
PONV was assessed using a three point ordinal scale (0=none, 1=nausea, 2=retching, 3=vomiting) (15) at PACU arrival (T1), 30 min after PACU arrival (T2), 6 hr after PACU discharge (T3) and 24 hr after PACU discharge (T4). Nausea was defined as a subjectively unpleasant sensation associated with awareness of the urge to vomit. Retching was defined as labored, spasmodic, rhythmic contraction of respiratory muscles without expulsion of gastric contents. Vomiting was defined as forceful expulsion of gastric contents from the mouth. Severity of PONV from T2 to T3 and from T3 to T4 was evaluated using a Rhodes index at T3 and T4 (16). Ondansetron 0.1 mg/kg was intravenously given for rescue anti-emetic treatment on demand. Cumulative numbers of intravenous ondansetron at T1, from T1 to T2, from T2 to T3 and from T3 to T4 were recorded.
Postoperative pain was also assessed using the visual analogue scale (VAS, ranged from 0 to 100, 0=no pain, 100=worst pain imaginable) concurrently with PONV. Ketorolac 0.5 mg/kg was given intravenously for postoperative rescue analgesia on demand. Cumulative numbers of intravenous ketorolac were recorded for the same time periods listed above for ondansetron.
Anesthesia time (from start of TCIs or injection of propofol to operation room discharge) and operation time (from surgical incision to end of surgery) were recorded.
Statistical analysis
The primary outcome was Rhodes index at T3 according to µ-opioid receptor polymorphism. Secondary outcomes were PONV scales at T1, T2, and T3 according to µ-opioid receptor polymorphism. In a pilot study of AA type patients undergoing local breast excision under general anesthesia (5 and 5 in T and I groups), Rhodes index at T3 was 2.6±4.1, and PONV scales at T1, T2, and T3 were 0.4±0.5 , 0.6±0.7 and 0.8±1.0, respectively. PONV scale of 0.8 at T3 represented nausea. To distinguish PONV scale among the types, 0 for none, 2 for retching, or 3 for vomiting of PONV scale were expected in other types. Therefore, a minimum detected difference of one score in PONV scale among the types was considered to be of clinical significance. According to PONV scale at T3, a minimum detected difference of 100% in Rhodes index at T3 was considered to be of clinical significance. Therefore, the sample sizes of 61 for Rhodes index, and 39, 35, and 39 for PONV scales at T1, T2, and T3 were calculated with a power 0.9 and an α value of 0.05. Analyses according to the µ-opioid receptor polymorphism were followed by those according to anesthetic techniques.
Data were analyzed using Statistical Package for the Social Sciences 18® (IBM SPSS Inc., Chicago, IL, USA). Differences among the µ-opioid receptor polymorphism were analyzed using an one-way analysis of variance as parametric test, and chi-square test, Fisher exact test or Kruskal-Wallis test as non-parametric test. If results were statistically significant, Bonferroni's test was performed for multiple comparisons among groups. All data are expressed as number of patients or mean ± standard deviation. A value of P<0.05 was considered statistically significant.
Ethics statement
The study protocol was approved by the institutional review board of Konkuk University Medical Center, Seoul, Korea (IRB No. KUH1160043). Informed consent was confirmed by the IRB. The study was registered at Clinical Research Information Service; Korea Centers for Disease Control and Prevention, Ministry of Health and Welfare (Registration number: KCT0000461; http://cris.nih.go.kr).
RESULTS
Four hundred and thirty-three patients were eligible for the study from June 2012 to July 2014. Seventeen of these patients were excluded: five patients for re-do case, four for other concurrent surgery, one for allergy to egg or soybean oil and 7 for receiving current medications. Thus, 416 patients overall were included in the final analysis (Fig. 1).
One hundred fifty eight patients (38%) were homozygous type (AA), 195 patients (46.9%) were heterozygous type (AG), and 63 patients (15.1%) were homozygous type for the G allele (GG) (Table 1). Demographic variables had similar distributions among A118G genotype (Table 1). Analyses of inter-group differences showed only lower PONV scale value at T1 in patients with GG type as compared with AA and AG types (P=0.002) (Fig. 2A). Rhodes index and VAS did not show significant intergroup differences (Fig. 2B, C).
Similar distribution of anesthetic technique in each A118G genotype was observed with P=0.671 (Table 2). Demographic data were also similarly distributed according to anesthetic technique within µ-opioid receptor groups (Table 2). As expected, propofol use was higher in T vs. I group for each µ-opioid receptor gene group (Table 2). In patients with AA and AG types, T group showed significant lower values of PONV scale at T1, T2, and T3, compared with I group (Fig. 3A). However, in patients with GG type, T group showed no differences for all parameters, compared with I group (Fig. 3A). In patients with GG type in I group had significantly lower PONV scale value at T1 than AA and AG types (0.0±0.0 in GG type; 0.5±0.9 in AA type and 0.4±0.8 in AG type, P=0.003) (Fig. 3A). Rhodes index and postoperative pain did not show significant intergroup differences according to the µ-opioid receptor gene polymorphism or anesthetic technique (Fig. 3B, C). Total cumulative numbers of rescue anti-emetics and analgesics did not show significant intergroup differences in all time.
DISCUSSION
This study showed different patterns of PONV timing and intensity according to µ-opioid receptor gene polymorphism in patients undergoing general anesthesia with remifentanil. Patients with GG type A118G SNP showed lower PONV scale value on arrival at PACU than the other types. Analyses according to anesthetic technique for each µ-opioid receptor gene polymorphism showed better outcomes of PONV in TIVA, compared with inhalation anesthesia, except for no difference in patients with GG type.
Research in anesthesia on opioid receptor gene polymorphism has focused on postoperative pain (17, 18, 19), mainly evaluating association of postoperative pain and postoperative opioid use for each opioid receptor polymorphism. Increased opioid use would be absolutely associated with PONV because postoperative use of opioid is a well-known risk factor of PONV (1). Therefore, these studies were not suited to evaluate the relationship between PONV and opioid receptor gene polymorphism. Moreover, anesthetic protocol was not standardized (17), intraoperative infusion of remifentanil was inconsistent (18), and one study was done in the setting of spinal anesthesia (19).
The present study used a fixed target concentration for plasma-site of remifentanil 10 ng/mL to equalize the effect of opioid on PONV among opioid types. The slow achievement at anesthesia induction and maintenance during anesthesia for target concentration of remifentanil in the present study was able to establish the pseudo-steady state and to prevent the overshooting of the plasma-site concentration with side effects, such as hypotension, bradycardia and chest tightness. Remifentanil with its characteristic of rapid clearance is expected to be associated with less PONV. Kim et al. (20) proved that PONV occurrence was similar between remifentanil 10 ng/mL and 5 ng/mL, although remifentanil 10 ng/mL showed the better hemodynamic stability without increasing the side effects. Therefore, inconsistent results on PONV among studies of patients undergoing general anesthesia with remifentanil appeared associated not with remifentanil itself but with genetic variation.
The lower PONV scale value in patients with GG type at T1 was remarkable in the present study. Several studies have reported no significant differences in PONV incidence and scale during 24 hr post surgery (18, 19). In the present study, no significant differences in Rhodes indices were observed at T3 and T4. However, in patients of Han descent with GG type undergoing total abdominal hysterectomy or myomectomy required more intravenous fentanyl to achieve adequate pain relief but had similar PONV rates than other types (18). Chinese Singaporean women with GG type, receiving intrathecal morphine during Cesarean section also required more intravenous morphine but had lower or similar PONV compared with other types (19). The latter observations suggest that patients with GG type are resistant to the effect of opioid and show lesser PONV despite higher opioid use for postoperative pain. Lower PONV scale value in patients with GG type at T1 in the present study could be explained by a diminished effect of remifentanil during emergence and recovery after anesthesia, and because of rapid clearance the effect would be short and not influence time points other than T1.
Interestingly, PONV outcomes in patients with GG type were similar for both anesthetic techniques while for other SNP types they were better at T1, T2, and T3 for TIVA vs. inhalation anesthesia. GG type SNP therefore might have a protective role for inhalation anesthesia-induced PONV.
Because patients usually wake up at propofol concentrations of 1.0-2.0 µg/mL during TIVA, the anti-emetic effect of propofol lasts for up to 30 min after operation (21). And better outcomes of PONV until T3 in patients with AA and AG types in T group were not unexpected.
In the present study, postoperative pain did not differ according to µ-opioid receptor gene polymorphism or anesthetic technique. However, several studies have demonstrated that patients with GG type require more analgesic for postoperative pain (17, 22, 23), and generally, TIVA is preferred to inhalation anesthesia based on postoperative pain (24, 25). In this study, postoperative pain after local excision of breast was not severe and was limited; and Kim et al. had reported that the postoperative pain after local excision of breast might be controlled with ketorolac (17). Injection of ketorolac at the end of the surgery appears to have almost completely covered postoperative pain with or without remifentanil-induced hyperalgesia although some patients needed rescue ketorolac.
Frequency of AG, AA, and GG type groups was 46.9%, 38.0%, 15.1%, respectively, which differs from other reports (18, 19). However, the 118G allele frequency of 38.6% in the present study was closer to that reported for Han ethnicity (32.4%) and Chinese Singaporean (33.7%), and differs more noticeably from that in Caucasians (11.5%) and African Americans (1.6%) (18, 19, 26). Because of the higher frequency of GG type, Koreans might experience lower PONV scale immediately after general anesthesia as compared to the other populations, a possibility that warrants research.
In the present study, we focused PONV until postoperative 6 hr, although the evaluation was performed until postoperative 24 hr. The female patients undergoing local breast excision under general anesthesia were enrolled for the study. Because local breast excision is performed in ambulatory surgery center, the prediction and prevention of PONV before discharge is important. Therefore, primary and secondary outcomes were PONV until postoperative 6 hr.
In conclusion, µ-opioid receptor polymorphism influences PONV occurrence, thereby influencing anesthetic technique choice to improve patient experience. The patients with GG type showed lower PONV at PACU arrival regardless of anesthetic technique, compared with AA and AG types, showing the better outcomes of PONV in TIVA. Korean women with larger distribution of GG type, compared with other population, might have advantage in PONV.



 XML Download
XML Download