

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Antimicrobials are one of the most commonly prescribed therapeutic agents in pediatric population worldwide (1, 2, 3). Antibiotic overuse increases health care costs substantially without providing much of therapeutic benefits in most patients. Recent studies have associated antibiotic exposure with a multitude of negative health-related consequences including long-term reduction in microbiota diversity, increased risk of atopic diseases, and even inflammatory bowel diseases (1, 4, 5, 6). More importantly, it has been a major public health problem and the most important factor in the emergence of antibiotic resistance (7, 8). Especially, even for conditions in which antibiotic use might be justified, concerns about overuse of broad-spectrum antibiotics such as amoxicillin/clavulanate, second- and third-generation cephalosporins, macrolides, quinolones have been expressed previously in many papers (9, 10, 11, 12).
To reduce overzealous prescribing habits and inappropriate use of antibiotics, public health campaigns and initiatives have been promoted. As awareness of the potential adverse events associated with overuse of antibiotics increased, general decline of antibiotic-prescribing rates have been observed recently in many countries (13, 14, 15). Nevertheless, a substantial number of antibiotic prescriptions are still written for clinical conditions that does not require the use of antibiotics. Such clinical conditions include common colds, acute upper respiratory tract infections, and bronchitis, and they account for a large proportion of the unnecessary antibiotic use. These conditions have a predominantly viral etiology and antibiotic treatment has not been shown to have a major clinical impact (16, 17). Particularly in pediatric patients, it has been estimated that 50% of all antimicrobial prescriptions are unnecessary (13, 18).
This study was conducted to assess national prevalence of pediatric antibiotic prescriptions for acute upper respiratory tract infections in ambulatory settings in Korea.
MATERIALS AND METHODS
Data source
We analyzed National Patients Sample (NPS) database by the Korea Health Insurance Review & Assessment Service (HIRA) from January 1, 2009 to December 31, 2011. The National Health Insurance (NHI) program, which was first introduced in Korea in 1977, is a publicly funded and managed program that has been expanded to cover the entire Korean population by 1989 (19). HIRA receives NHI claims from healthcare providers and collects information on patient demographics, symptoms, procedures, diagnoses, and prescribed medications for approximately entire 50 million Koreans. HIRA-NPS data, a nationally representative sample of whole beneficiaries, was constructed using a gender- and age-stratified random sampling from whole Korean population. No significant difference in the gender distribution, age distribution or average prevalence in specific drug use was found in a validation study (20). Also, a validation study compared the diagnosis derived from the HIRA database with the actual diagnosis in the patient medical records. The overall positive predictive value of the diagnoses was 83.4% (21). The resulting probability sample consisted of 3,416,578 individuals between 2009 and 2011.
HIRA-NPS data contains anonymized codes representing each individual together with information on patients (age, gender, diagnoses), medical institutions (type of institution, region), physician specialties, medical procedures, and prescribed drugs. All diagnoses are recorded using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). Information on prescribed drugs included generic name, prescription date, dosage, duration, and route of administration. All researchers who wish to use the HIRA-NPS and its data subsets are required to sign a written agreement declaring that they have no intention of attempting to obtain information that could potentially violate the privacy protection for patients or care providers.
Study population and diagnostic categories
The eligible study population included all children younger than 18 yr old who visited ambulatory care settings with diagnoses of acute upper respiratory tract infections (URI) during 2009-2011. The URI visits included those patients with diagnoses of acute nasopharyngitis (common cold), acute sinusitis, acute pharyngitis, acute tonsillitis, acute laryngitis/tracheitis, acute obstructive laryngitis/epiglottitis and acute upper respiratory infections of multiple and unspecified sites (ICD-10 codes J00, J01, J02, J03, J04, J05, and J06). These diagnoses are classified into two groups including URIs for which antibiotics are often indicated (acute sinusitis, acute pharyngitis, acute tonsillitis) and URIs for which antibiotics are rarely indicated (common cold, acute laryngitis/tracheitis, acute obstructive laryngitis/epiglottitis, and acute upper respiratory infections of multiple and unspecified sites). Infants and toddlers who were younger than 24 months old were excluded from the study population due to possible uncertainty in patient administrative data.
Study drugs
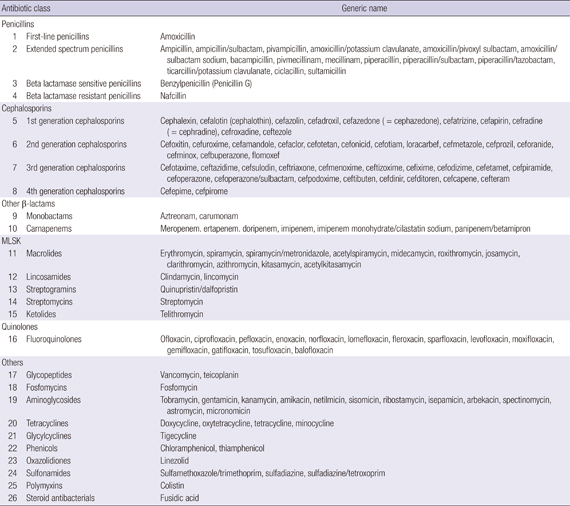
Using the World Health Organization (WHO) Anatomical Therapeutic Chemical (ATC) Classification, the study drugs are limited to medicines that follow the definition of ATC class J01, which are antibiotics for systemic use. Antivirals, antifungals, and topical antibiotics (e.g., ophthalmic solutions, topical ointments) were excluded from the study drug list. After these exclusions, 128 antibiotic drugs were included in the study. Antibiotics were grouped into 26 classes including first-line penicillins, extended spectrum penicillins, beta lactamase sensitive penicillins, beta lactamase resistant penicillins, first- to fourth-generation cephalosporins, macrolides, lincosamides, streptogramins, streptomycins, ketolides, monobactams, carbapenems, fluoroquinolones, aminoglycosides, sulfonamides, tetracyclines, glycopeptides, fosfomycins, glycylcyclines, phenicols, oxazolidiones, polymyxins, and steroid antibacterials (22) (Appendix).
Analysis
In this study, the analyses of frequencies and proportions of antibiotic prescriptions were spell-based using every outpatient visit as the unit. We first analyzed the frequency of antibiotic prescriptions in pediatrics with URI by calculating the proportions of antibiotic prescriptions for each year. The denominator used in this calculation was total prescriptions in pediatric patients with URI and the numerator was prescriptions containing one or more antibiotic drugs. In order to see the antibiotic prescribing pattern according to diagnosis, proportions of antibiotic prescriptions were calculated by dividing the number of antibiotic prescriptions by all prescriptions written for each diagnosis: acute nasopharyngitis (common cold), acute sinusitis, acute pharyngitis, acute tonsillitis, acute laryngitis/tracheitis, acute obstructive laryngitis/epiglottitis, acute upper respiratory infections of multiple and unspecified sites. Percentage of antibiotic prescriptions within each diagnostic category was also estimated. Prescriptions with both diagnosis codes which antibiotics were often indicated and rarely indicated were classified as those written for diagnoses which antibiotics were often indicated.
We also calculated the frequencies and proportions of antibiotic prescriptions by antibiotic groups. The proportions of each drug group comprising antibiotic prescriptions were presented according to the year. The difference between proportions in 2009 and 2011 for each drug group was calculated. Absolute difference and relative difference were estimated in proportions of antibiotic groups, and the 95% confidence intervals (CI) were calculated.
To investigate the status of antibiotic use in pediatric patients with URI in detail, we performed a comprehensive analysis according to the type of medical care institution, physician specialty and geographic region.
Antibiotic prescribing proportions for pediatric outpatients in each prescribed circumstances were calculated. Along with prescription proportions, daily amount of prescribed antibiotics was estimated using Defined Daily Dose (DDD) and expressed in DDDs per 1,000 pediatric outpatients per day. In this analysis, every beneficiary was the unit. Referring to the index from WHO ATC/DDD classification, DDD was assigned to each antibiotic drug. DDD values of some drugs which are not listed by WHO were determined on the basis of literature articles and drug labels (23). DDDs are the sum of total amount of drug prescribed (single dose×frequency×days prescribed) divided by the specific DDD for that drug. DDDs/1,000 persons/day was calculated using the following equation: DDDs×(1,000 persons/the number of outpatients for each type of medical care institution, physician specialty, and geographic region)×(1/365 days). To adjust variations in age distributions across regions, the direct method of age-standardization was applied to the estimation of antibiotic prescribing proportions and daily amount of antibiotic consumption.
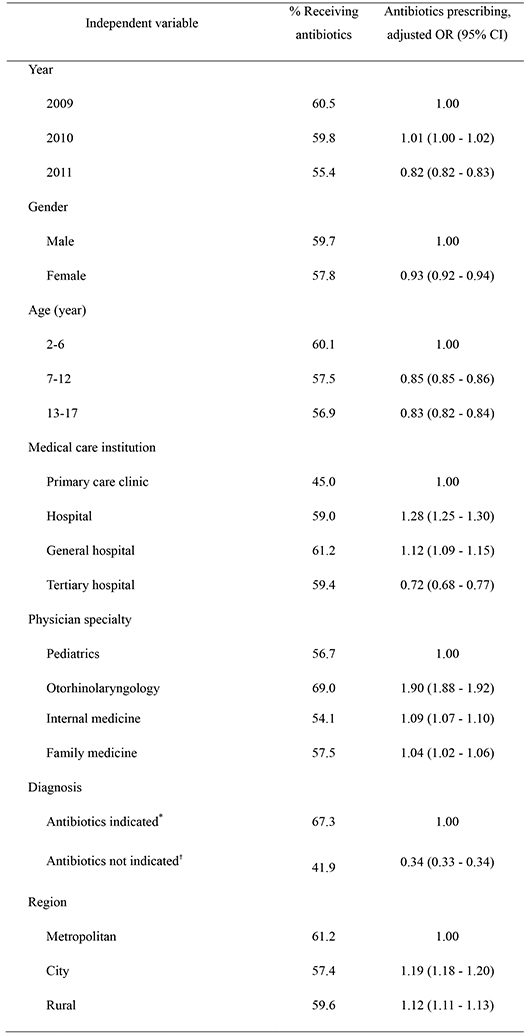
Also, we performed multiple logistic regression to identify demographic and clinical factors associated with antibiotic prescribing. The factors considered were year (2009, 2010, and 2011), gender (male and female), patient age (2-6, 7-12, and 13-17 yr), region (metropolitan, city, and rural), type of medical care institution (tertiary hospital, general hospital, hospital, and primary care clinic), physician specialty (pediatrics, otorhinolaryngology, internal medicine and family medicine), and diagnosis (antibiotics indicated and not indicated). All statistical analyses were performed using the SAS statistical application program (Release 9.3, SAS Institute Inc., Cary, NC, USA).
RESULTS
During the study period, total 1,267,999 prescriptions were identified in 194,570 pediatric outpatients with diagnoses URI (Table 1). The overall antibiotic prescribing proportion was 58.7% during the study period. The annual proportion of antibiotic prescribing slightly decreased (55.4% in 2011 vs. 60.5% in 2009; adjusted odds ratio, 0.82; 95% CI, 0.82-0.83) (Tables 2, 3). The most commonly prescribed antibiotic class was extended spectrum penicillins which accounted for 49.0% of antibiotic prescriptions. Second generation cephalosporins, macrolides and first-line penicillins were also frequently prescribed (20.3%, 15.6%, and 9.4%, respectively). The proportion of extended spectrum penicillin prescriptions remained stable during study period, whereas second generation cephalosporin, first generation cephalosporin, lincosamide, aminoglycoside, and fluoroquinolone decreased (Table 2). The proportions of prescription in which first-line penicilins, macrolide, third generation cephalosporin, and sulfonamides were used increased by 10.5%, 16.0%, 40.7%, and 13.1%, respectively.
The associations between demographic and clinical variables and antibiotic prescribing are shown in Table 3. The use of antibiotics was relatively low in patients aged 7 yr or older when compared to younger patients. Also, less antibiotic prescribing proportion was shown in diagnoses without indications for antibiotics (41.9% vs. 67.3%; adjusted odds ratio, 0.34; 95% CI, 0.33-0.34).
Also, antibiotic prescribing proportions for each diagnosis were much higher in diagnosis with indications (67.3%) compared to those without indications (41.9%) (Table 3). In terms of the change in prescribing proportion for each diagnosis, antibiotic prescribing decreased more in diagnoses without indications for antibiotics (8.5% vs. 6.8%) (Table 2). Antibiotic prescribing was decreased by 8.7% and 7.4% for acute upper respiratory infections of multiple and unspecified sites (J06) and acute nasopharyngitis (J00) respectively. Such reduced use of antibiotics in conditions without indications may be inferred as an evidence of improved prescribing practice.
The antibiotic prescribing was related to the types of medical care institutions. Tertiary hospitals were less likely to prescribe antibiotics than primary and secondary hospitals (adjusted odds ratio, 0.72; 95% CI, 0.68-0.77) (Table 3). Extended spectrum penicillin was the most commonly prescribed antibiotic regardless of type of medical care institutions. However, the proportions of second and third generation cephalosporin showed substantial differences depending on the type of medical care institutions. Also, greater consumption of antibiotics was observed in smaller and lower-level medical care institutions (Fig. 1).
Among physician specialties, the highest proportion of antibiotic prescribing was shown in otorhinolaryngology (69.0%, adjusted odds ratio, 1.90; 95% CI, 1.88-1.92). However, the proportions of each antibiotic class prescribed were similar regardless of physician specialties (Fig. 2). Geographic variations were found across regions in Korea (Fig. 3). Metropolitan regions tend to have a relatively lower proportion of antibiotic prescribing, ranging from 53.4% in Seoul to 57.2% in Incheon, compared to the overall average proportion of 58.7%. For city and rural regions, adjusted odds ratios were 1.19 and 1.12, respectively (Table 3).
DISCUSSION
This is a descriptive study to provide current prevalence of antibiotic-prescribing for pediatric outpatients with URI in Korea. In this study, frequent prescribing of antibiotics for URI during ambulatory pediatric visits was observed, which occurred in more than half of the prescriptions written. However, the annual proportion of antibiotic prescribing in pediatric outpatients with URI decreased during three years of study period (55.4% in 2011 vs. 60.5% in 2009; adjusted OR, 0.82). Its reduction is consistent with the global trends of decreasing antibiotic use in ambulatory settings, as previous studies had reported (13, 14, 15). Such decline might have resulted from increased attention to antimicrobial resistance in the media and continuous efforts by many organizations to promote appropriate use of antimicrobials, including public disclosure of antibiotic prescribing rates in medical care institution that was initiated by the Ministry of Health and Welfare. Another favorable finding was that antibiotics were less prescribed (adjusted OR, 0.34) and more decreased in diagnoses without indications for antibiotics (8.5% vs. 6.8%) than in those with indications for antibiotics. Such reduced use of antibiotics may be inferred as an evidence of improved prescribing practice.
Several studies identifying trends of antimicrobial prescribing have shown that antibiotic use for URI in children has substantially decreased and its prescribing rate was stabilized down to approximately 10% in the United States (13, 24). The majority of the antibiotic studies analyzed the antibiotic use in adults or in general pediatric patients not specific to URI. According to Finkelstein et al. (25) overall antibiotic rates for children under 18 yr old decreased continually from 1996 to 2000 with greater % reduction in children younger than 6 yr old. In our study, the annual percentage of antibiotic prescriptions has also slightly decreased. However, it is still considered higher than that of Western countries.
We also found that more antibiotic prescriptions were given in primary care clinics and secondary hospitals than in tertiary hospitals. A patient first seen in primary care clinic may be referred to a higher level of care facility when special expertise and equipment are required for the condition. Considering that primary care clinics are initially visited for most generalized health issues, huge antibiotic prescribing in primary care suggests excessive prescribing without mandatory indications. Also, proportions of each antibiotic class showed differences depending on the type of medical care institutions. Third generation cephalosporin was more frequently prescribed in tertiary care hospitals when compared to secondary and primary care clinics. Third generation cephalosporins have further increased activity against Gram-negative organisms, but it is not generally recommended as a first-line treatment due to decreasing susceptibility. When a patient first seen in primary care clinic was referred to a higher level of care facility, physicians may review patients' medication history and consider another antibiotic class. Therefore, such different antimicrobial properties may influence the pattern of antibiotics use according to the type of medical care institutions.
Significant increases in the proportions of third generation cephalosporins and macrolides raise concerns about overuse of particular antibiotics. Several studies have reported that frequent utilization of third generation cephalosporin is a risk factor for occurrence and spread of extended spectrum beta-lactamase (ESBL)-producing bacterial pathogens, and extensive use is considered to be an independent risk factor (9, 26). Macrolide spectrum is slightly wider than that of penicillin and it is used to treat infections caused by atypical pathogens such as Mycoplasma pneumoniae. The epidemic of Mycoplasma pneumoniae in 2007 that occurs periodically every three or four years may be responsible for the macrolide increase (27). However, macrolides are not generally recommended for URI caused by M. pneumoniae, and the efficacy of macrolides for Mycoplasma is still controversial (28). Also, studies have documented that countries with a high consumption of macrolides have experienced a rapid increase in macrolide resistance in the common pathogens of respiratory tract infections such as Streptococcus pneumoniae, and currently its resistance is becoming a globally growing concern (12, 29). Therefore, continuous monitoring of its prescribing patterns and a further research on its resistance seem to be necessary.
No antibiotic in Korea is approved as an over-the-counter (OTC) medication and all antibiotics are covered by the HIRA. Additionally, Korean patients pay a fee-for-service for all services including drugs; therefore, misclassification of antibiotics in general does not occur. Our study included a sample claims data which was abstracted from the whole Korean population. The data was constructed using a gender and age-stratified random sampling, which guarantees the representativeness, and it was validated that there was no significant differences in gender distribution, age distribution, or average prevalence in specific drug use.
Despite our findings, the study has certain limitations. First, even though HIRA-NPS data has large sample and high generalizability, the suitability of administrative claims data to identify certain disease in research is not well established. Due to limitations in the level of clinical details encoded by coding system and the required codes in reporting insurance claims, the accuracy of diagnostic codes for URI needs to be investigated. Second, the outpatients with diagnoses URI included in our study might have more than one diagnosis besides URI at the same time. In those cases, antibiotics could be prescribed not only for URI but also for other purposes. Therefore, the relation between antimicrobial use and a specific disease should be interpreted carefully. Another limitation of this study is that the study period of three years may be too short to make our conclusion definitive. Further analyses with long-term databases are needed to explore trends of antibiotic use over time and to identify the factors which drive inappropriate antimicrobial use decisions.
There is a consensus that antimicrobial use can lead to drug resistance. The decline in antimicrobial prescribing proportions for pediatric outpatients with URI was observed from 2009 to 2011. Despite the decrease in antimicrobial prescribing for children, proportions of third generation cephalosporins and macrolides were increasing. Currently, these antibiotic classes have been issued warnings on increasing resistant bacteria. Therefore, it is important to promote appropriate antibiotic selection, so that can reduce the antimicrobial prescribing. As well as a restrictive antibiotic policy, developing practical guidelines and educational resources seem necessary to help physicians with choosing appropriate antimicrobial therapy.



 XML Download
XML Download