

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Japanese encephalitis (JE) virus is the leading cause of viral encephalitis in Asia. The recent emergence of JE virus in new territories that has been attributable to the climate change and international travel has raised the concern of global public health (1, 2). Because there are still limitations in vector control and specific antiviral treatment of JE, vaccination is the most effective strategy for prevention.
Although the inactivated Vero-cell culture JE vaccine has recently introduced, two JE vaccines have been widely used in Korea: the mouse brain-derived, killed-inactivated JE vaccine (MBDV) and the live attenuated SA 14-14-2 JE vaccine (LAJEV). MBDV was first developed in Japan (BIKEN, distributed by Sanofi Pasteur as JE-VAX) and the only commercially used vaccine worldwide for past decades (3, 4). Local productions of similar vaccine have been used effectively to immunize travelers and residents in enzootic areas, and this has reduced JE incidence in some countries. However, the MBDV had the uncertainty as to the duration of protection and required multiple doses to maintain immunity (5, 6). In addition, an unacceptable occurrence of neurologic and hypersensitivity reactions has prompted a major manufacturer to cease production in Japan (6, 7, 8). In 1994, two cases of death temporally associated with MBDV led to a serious social issue, and to establish the Vaccine Injury Compensation Program in Korea. As such, there has been an apparent need for a vaccine with an enhanced safety profile and smaller dose schedule to protect against JE, which led to the introduction of LAJEV.
Since its licensure in 1988, more than 300 million doses of LAJEV have been administered in China where it has shown an excellent efficacy and safety profile (9, 10). This vaccine manufactured in China has been used in countries of western pacific region and Asia (Nepal, Sri Lanka, India, and Korea), and constituted more than 50% of the global production of all JE vaccines in 2005 (11). However, the lack of precedence for using a primary hamster kidney cell line as the substrate and the safety profile remain special issues of concern (12). Nevertheless, some physicians prefer to use the LAJEV because of simple schedule compared with MBDV. The primary series in Korea is scheduled with two doses administered 12 months apart in infants aged 1-2 yr. This preferred interval was established based only on data from studies conducted in China (13), and no published data for the primary series using a 12-month interval exists for countries other than China. Therefore, this study was undertaken to assess the immunogenicity and safety of LAJEV according to the local schedule in Korea.
MATERIALS AND METHODS
Study design
The study was designed as an open-label, prospective cohort, multicenter trial in Korea. The study was performed at five centers between July 2, 2007 and October 26, 2009. At enrollment, eligible participants from 1 to 3 yr of age were given a brief health examination, blood samples were taken, and the first vaccine dose was administered. A follow-up visit occurred at 4-6 weeks after vaccination, at which point blood samples were collected from all children. One year after the first vaccination, a blood sample was collected and the second vaccine dose was administered. As with the first dose, a follow-up visit was done at 4-6 weeks after second vaccination and blood samples for immunogenicity analysis were collected.
Study subjects
Healthy children without significant medical history or clinically significant physical examination or laboratory findings at screening were eligible. Exclusion criteria included: congenital or acquired immunodeficiency or immunosuppressive conditions; hypersensitivity to any of the vaccine components; use of systemic corticosteroids, immunosuppressive medications, or biological agents in the previous 3 months or anticipated administration of such medications during the course of the study; a known history of clinically, serologically or microbiologically confirmed flavivirus infection; or febrile or acute illness on the day of injection. The protocol allowed children to receive additional vaccines as recommended, including hepatitis A vaccine at 12 to 24 months of age, Haemophilus influenzae type b conjugate vaccine and pneumococcal conjugate vaccine at 12 to15 months of age, and diphtheria, tetanus, acellular pertussis (DTaP) vaccine at 15 to 18 months of age, as long as doses were given at least 8 days after and at least 4 weeks before a dose of the study vaccine. Measles, mumps, rubella (MMR) and varicella vaccines were allowed if administered at least 4 weeks before or after administration of the study vaccine.
Study vaccine
LAJEV (CD-JEVAX™, Chengdu Institute of Biological Products, Chengdu, China) was used in this study. The main component of this vaccine is SA14-14-2 strain of JE virus. The others are lactose, sucrose, gelatin, human blood albumin and urea. Each subject was administered 0.5 mL of freshly reconstituted vaccine subcutaneously to the upper arm as instructed by the manufacturer.
Immunogenicity evaluation
Blood samples for immunogenicity assays were taken prior to and 4-6 weeks after each vaccination. The samples were kept frozen at -70℃ and were sent to the central laboratory of the Korean National Institute of Health. Sera were tested for neutralizing antibodies using the plaque reduction neutralization test (PRNT) as followings. Test sera were heat-inactivated at 56℃ for 30 min and diluted 1:5 and in serial two fold dilutions (up to 1:2,560). The Nakayama strain (heterologous SA-14-14 strain) was diluted in phosphate buffer saline containing 5% fetal calf serum and 5% guinea pig complement to provide 200 pfu/0.1 mL, and added in equal volume to each serum dilution. Serum-virus mixtures were incubated over-night at 48℃ and added to drained baby hamster kidney 21 cell culture monolayers grown in six well plates. After adsorption for one hour at 37℃, the monolayers were overlaid with semisolid medium. Approximately 5 days later, when plaques could be seen microscopically, the medium was removed. The complete titration of each serum was carried out in a single test (14). The end point for neutralization was the highest dilution of serum reducing plaques by 50% of the JE challenge virus, compared with a negative serum control. JE neutralizing antibody titer ≥10 was considered seropositive and seroprotective (15).
Safety evaluation
After vaccination, a physician monitored subjects for any immediate sign or symptom of local and/or systemic reactions for at least 30 min. We asked the parents or legal guardians to record any adverse reactions occurred from days 0-42 after vaccination. Significant local reaction was defined as redness >2.5 cm, swelling >2.5 cm, or tenderness, or crying and protesting when the injection site was touched. Systemic reactions included vomiting, diarrhea, irritability, drowsiness, loss of appetite, shivering, or fever. Fever was defined as a temperature ≥38℃ (100.4°F) (16). Symptoms were defined as being related if there was a reasonable possibility that the vaccine contributed to the adverse event. Unsolicited local or systemic reactions (with onset date, intensity and resolution) were recorded throughout the 42-day period after each vaccination. Serious adverse events were reported for the duration of the study. Blood pressure, pulse, and body temperature of all subjects were recorded at every visit, and physical examinations were performed.
Statistical analysis
Based on the premise of a 98% production rate of seroprotective antibody, a 10% allowable error for the trial and 10% level of significance, the minimum necessary number of subjects was found to be 65 in this study. Immunogenic response was assessed by the percentage of subjects with seroprotective neutralizing antibody titer and by calculation of the geometric mean titer (GMT) values. For the GMT, 95% confidence intervals (CI) were calculated using a percentile-based bootstrap method stratified by baseline serostatus. The percentages of subjects who experienced solicited and unsolicited adverse reactions were expressed. Missing data were excluded.
RESULTS
Subjects
Ninety subjects were enrolled to receive the first dose vaccine at five study centers. The male to female ratio was 1.0, and the median age at enrollment was 12±4 months (87 children age 12-23 months, two 24-35 months, and one 36-47 months). There were no withdrawals due to adverse events after the first vaccination. Among all subjects enrolled at the first vaccination, 19 subjects were lost to follow up at the second vaccination and 2 voluntarily withdrew participation. Overall, a total of 69 subjects completed the following study, thus receiving the second dose. Three samples after the second dose were not included in the immunogenicity analysis for reasons expected to impact immunogenicity such as erroneous sampling or inappropriate sampling time, but these cases were not excluded from the safety analysis. The male to female ratio of the follow-up group was 1.25, and the median age was 24±4 months (67 children age 24-35 months, one 36-47 months, and one 48-59 months).
Immunogenicity results
The immunogenicity results are summarized in Table 1. Seroprotection to the first dose was observed in 91.1% (82/90) of subjects. The GMT showed an increase of 3-fold (40.90, 95% CI, 30.09-50.58), from 12.86 (95% CI, 10.67-15.51) at baseline.
At the 1-yr follow-up, 4 out of 66 subjects had no detectable neutralizing antibody. Overall, the seroprotection rate following the second dose rose to 97% (64/66), compared to 93.9% (62/66) prior to vaccination. The GMT was measured from 33.05 (95% CI, 24.42-44.60) to 213.84 (95% CI, 151.54-301.59), representing a 6.47-fold rise.
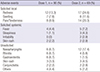
Safety
The results of adverse reactions after each dose are summarized in Table 2. Adverse events reported by all subjects after the first dose were mild to moderate in severity and self-limited in duration, with 18.9% of subjects reporting one or more adverse events. The most frequently reported local reactions after the first dose were redness (13.3%) and tenderness (8.9%) at the injection site. Systemic reactions were infrequent with the exception of fever (4.4%), but no subject experienced a fever ≥40℃. During the 42 days following vaccination, unsolicited adverse events were experienced by 30% of children. Most unsolicited adverse events were not related to vaccination, and included nasopharyngitis (6.7%), rhinitis (6.7%), gastroenteritis (6.7%), skin rash (3.3%), and conjunctivitis (2.2%).
The incidence of solicited local reactions was slightly higher after the second dose (30.3%) than the first dose. The most frequently reported local reaction was redness and tenderness, which occurred in 24.6% and 20.3% of subjects, respectively. Fever was developed in 7.2% subjects after the second dose. There were no serious adverse events, deaths, or withdrawals from the study due to any type of adverse event.
DISCUSSION
Over the past decades, there has been the geographical expansion of JE to new territories, and recurrent outbreaks in Vietnam, Nepal, and India (17). Because there is no other effective public health option for the prevention of JE, vaccination is the best tool for JE control. A number of organizations including PATH, WHO, UNICEF, and the United States CDC are together developing a strategic plan that could broadly control JE by 2015 (18). In the countries where high vaccination coverage has been achieved, such as in Japan, Taiwan, Thailand, and Korea, the incidence of JE has decreased, primarily as a result of widespread use of vaccines (17). The choice of vaccine will need to take into account long-term protection, ease of administration, cost, and above all, safety.
The primary outcome of this study was the remarkable immunogenicity of LAJEV given to Korean children aged 1 to 3 yr with local schedule. After the first dose, seroprotection was obtained in about 90% of subjects and the GMT increased 3-fold. Protective levels of antibodies were maintained in 93.9% of the subjects until the time of administration of the second dose, which was given 1 yr later. This finding is similar to previously published studies with relatively high immunogenicity (19, 20, 21, 22, 23). However, the seroprotection rate in a few studies was higher compared to our results. In a case-control study in Nepal, one dose of the vaccine given to children and adolescents aged 1 to 15 yr was shown to be 98.5% protective 1 yr following vaccination (24) and the vaccine remained protective at an estimated 96% 5 yr after vaccination in JE-endemic areas (25). A clinical study conducted by Sohn et al. revealed that LAJEV given as a single dose to Korean children aged 1 to 3 yr (mean age 27 months) produced seroprotection with antibody response as high as 96% (20), which possibly reflects the methodological differences in titer calculations, as noted by the authors (9, 19). In addition, age differences in the study groups may also affect antibody response.
The children enrolled in our study responded strongly to the second dose (96%), and the GMT increased by approximately 6.5-fold from the first dose level. A schedule was introduced in Korea based on results of a field trial of more than 250,000 Chinese children which found that high efficacy was achieved with two vaccine doses given 1 yr apart (13). Although the immunogenicity of two doses given 1 and 2.5 months apart has been reported in children ranging from 12 to 15 yr old (19), studies of the principal target group for primary immunization have not previously been conducted. Our study highlights antibody responses in young children, who are the target group for primary immunization in Korea. The 2-dose schedule of LAJEV could help to immunize children who did not have an adequate response to a first dose, and decrease the number of secondary vaccine failures. However, observational studies on children in China, Nepal and Thailand have suggested that even single dose of this vaccine can produce significant long-term protection (25, 26). Based on consideration of cost-benefit effect, there is a need for carefully planned studies to establish more optimal immunization schedule.
In this study, LAJEV was safe and well-tolerated. Reactogenicity was satisfactory, although local reactions tended to be more frequent after the second dose. The systemic reactions were mainly fever, which was seen in less than 10% of subjects during the study, and which resolved spontaneously in all cases. Most adverse events were relatively mild and self-limiting. There were no reports of encephalitis or aseptic meningitis following vaccination. In a prospective, randomized study where patients were actively monitored for 30 days, no cases of encephalitis or meningitis were observed, and no differences in hospitalization or prolonged fever were found (10). However, recent encephalitis cases have been reported in Chinese patients who received a first dose of LAJEV, although it is difficult to identify the causal link between the disease and JE vaccination (27). Therefore, concerns about safety still remain, and continued surveillance and careful investigation of any events that occur after LAJEV is required.
Some limitations of our study must be considered. First, the number of study subjects were relatively small. However, the study design was prospective, and the serial assessment of immunogenicity and safety of LAJEV over 1 yr was firstly done in Korean children with local schedule. Second, it is necessary to observe the long-term safety of this vaccine. Although severe neurologic or hypersensitivity reactions did not occur during this study, the prolonged observation of adverse events is required. Third, we did not assess the interchangeability of other available JE vaccines. Because the national immunization program (NIP) in Korea includes inactivated JE vaccine and LAJEV (approved as NIP vaccine in 2014), clinicians can face this situation considering interchangeable vaccination when a patient is lacking a vaccination record or there is a limited vaccine supply from a particular manufacturer. These limitations need to be addressed in future studies.
In conclusion, our findings provide evidence of high protection rate elicited by a 2-dose schedule of LAJEV given 1 yr apart. With respect to vaccine safety, there was no severe vaccine-related adverse events. Although the data is insufficient to conclude whether LAJEV can prevent JE outbreaks, we expect that this immunization strategy will decrease the susceptibility level and increase herd immunity in affected regions, and thereby substantially reduce the burden of JE.

 XML Download
XML Download