

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute cholecystitis is an acute inflammatory disease of the gallbladder (1). Gallstones are etiologically involved in 90%-95% of cases, whereas acute acalculous cholecystitis accounts for 5%-10% of cases, in which severe systemic conditions, such as surgery, trauma, long-term intensive care unit stay, infection, burns, and parenteral nutrition, are commonly involved (1). The majority of patients with acute cholecystitis follow a mild clinical course, but about 6% of patients progress to accompanying organ dysfunction (grade III) according to the Tokyo guidelines 2007 (TG07) for severity assessment (2). Recently, it was reported that older patients with acute acalculous cholecystitis are more likely to have more severe complications and to succumb to the disease (3). With the exception of one study, which showed a decline in T cell numbers and functional activity in elderly patients (4), little is known of the status of the immune system before intervention in patients with acute cholecystitis.
Human mucosal-associated invariant T (MAIT) cells and natural killer T (NKT) cells are two distinct subsets of innate-like T cells that express an invariant TCR Vα7.2-Jα33 chain paired with a limited repertoire of Vβ chains or an invariant TCR pair of Vα24-Jα18/Vβ11 chains together with the Vβ chain, respectively (5, 6). Using these unique pairs of TCR chains, MAIT cells recognize bacteria-derived vitamin B2 metabolite antigens presented by major histocompatibility complex (MHC) class Ib-like related protein MR1 (7), whereas NKT cells react with endogenous and exogenous glycolipid antigens, such as isoglobotrihexosylceramide (iGb3) and α-galactosylceramide (α-GalCer), presented by MHC class I-like protein CD1d (8). Following antigen recognition, MAIT cells rapidly produce Th1/Th17 cytokines, such as interferon-γ (IFN-γ) and interleukin (IL)-17 (9), whereas NKT cells rapidly produce large amounts of Th1 and Th2 cytokines, such as IFN-γ and IL-4, in an innate-like manner (8). Accordingly, MAIT cells play important roles in mucosal immunity and gut homeostasis (9, 10), and NKT cells act as regulatory and/or effector cells and are implicated in the control of autoimmune diseases, cancer, and infectious diseases (11). Furthermore, these two invariant T cells are known to play protective roles in host immune responses against a variety of infectious pathogens, including certain enterobacterial and mycobacterial species, viruses, fungi, and parasites (12, 13). In humans, MAIT and NKT cells are more abundant in liver as compared with peripheral blood, suggesting that effector functions of MAIT and NKT cells might overlap and lead to protect the liver from infectious agents and intestinal floral products that reach the intrahepatic blood circulation (14, 15).
Recently, it was reported that patients with severe cholecystitis have high microorganism culture rates in bile and blood (2). Of the microorganisms cultured in bile or blood, Escherichia coli was most prevalent followed by other enterobacterial species. However, little is known about the relevances of MAIT and NKT cells in acute cholecystitis. Thus, the aims of the present study were to measure MAIT and NKT cell numbers in the peripheral blood of patients with acute cholecystitis and to investigate potential relationships between these cell numbers and clinical parameters.
MATERIALS AND METHODS
Study population
The study cohort was composed of 30 patients with a diagnosis of acute cholecystitis (7 women and 23 men; mean±SD age 66.7±10.8 yr) according to the revised Tokyo guidelines (TG13) regarding diagnostic criteria for acute cholecystitis (16), and 47 age- and sex-matched healthy controls (11 women and 36 men; mean±SD age 65.3±8.3 yr). None of the controls had a documented history of autoimmune disease, pregnancy, infectious disease, malignancy, chronic liver or renal disease, or diabetes mellitus, or had ever received immunosuppressive therapy or experienced fever during the 72 hr prior to enrollment.
Monoclonal antibodies (mAbs) and flow cytometry
The following mAbs and reagents were used in this study: fluorescein isothiocyanate (FITC)-conjugated anti-CD3, phycoerythrin (PE)-Cy5-conjugated anti-CD161, FITC-conjugated anti-TCR γδ and PE-conjugated 6B11 (all from Becton Dickinson, San Diego, CA, USA), allophycocyanin (APC)-conjugated anti-TCR Vα7.2 (BioLegend, San Diego, CA, USA) and APC-Alexa Fluor 750-conjugated anti-CD3 (Beckman Coulter, Marseille, France). Cells were stained with combinations of appropriate mAbs for 20 min at 4℃. Stained cells were analyzed on a Navios flow cytometer using Kaluza software (Beckman Coulter, Brea, CA, USA).
Isolation of peripheral blood mononuclear cells (PBMCs) and the identification of MAIT and NKT cells
Peripheral venous blood samples were collected in heparin-containing tubes, and PBMCs were isolated by density-gradient centrifugation using Ficoll-Paque Plus solution (Amersham Biosciences, Uppsala, Sweden). MAIT and NKT cells were identified phenotypically as CD3+TCRγδ-Vα7.2+CD161high and CD3+6B11+ cells, respectively, by flow cytometry, as previously described (17, 18, 19, 20, 21).
Statistical analysis
Percentages and absolute numbers of MAIT and NKT cells were compared using the Mann-Whitney U test. Linear regression analysis was used to examine potential relationships between MAIT/NKT cell numbers and clinical or laboratory parameters. P values of less than 0.05 were considered statistically significant. The statistical analysis was performed using SPSS version 18.0 (SPSS, Chicago, IL, USA).
RESULTS
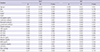
The clinical and laboratory characteristics of the acute cholecystitis patients are summarized in Table 1. Thirty patients with acute cholecystitis treated during a 6-month period were included in this study. Of these patients, 24 (80%) and 6 (20%) patients had moderate and severe acute cholecystitis, respectively, according to the Tokyo guidelines (TG13) (16).
The percentages and absolute numbers of MAIT cells in the peripheral blood samples of the 30 patients and the 47 age- and sex-matched healthy controls (HCs) were determined by flow cytometry. MAIT cells were defined as CD3+TCRγδ- cells expressing TCR Vα7.2 and CD161high (Fig. 1A). Percentages of circulating MAIT cells were significantly lower in patients than in HCs (median 0.34% vs. 1.37% [P<0.05]) (Fig. 1B). Absolute numbers of MAIT cells were calculated by multiplying MAIT cell fractions by CD3+γδ- T cell fractions and total lymphocyte numbers (per microliter of peripheral blood). Acute cholecystitis patients had significantly lower absolute numbers of MAIT cells than HCs (median 0.75 cells/µL vs. 8.51 cells/µL [P<0.001]) (Fig. 1C).
The percentages and absolute numbers of NKT cells in the peripheral blood samples of the 30 patients and the 47 age- and sex-matched HCs were determined by flow cytometry. NKT cells were defined as CD3+6B11+ cells (Fig. 2A). No significant difference was observed between the NKT cell percentages of patients and HCs (Fig. 2B). Absolute NKT cell numbers were calculated by multiplying NKT cell fractions by total lymphocyte numbers (per microliter of peripheral blood). Acute cholecystitis patients had significantly lower absolute NKT cell numbers than HCs (median 0.47 cells/µL vs. 0.78 cells/µL [P<0.05]) (Fig. 2C).
To investigate the clinical relevances of MAIT and NKT cell levels in patients, we explored relationships between the absolute numbers of MAIT cells and NKT cells in peripheral blood with clinical and laboratory parameters using regression analysis (Table 2). Because distributions were skewed, the absolute numbers of MAIT cells and NKT cells were log-transformed for the analysis. Linear regression analysis showed that log-transformed MAIT cell numbers were significantly correlated with age and lymphocyte count (P=0.039 and P=0.025, respectively). Log-transformed NKT cell numbers were found to be significantly correlated with age, TG13 grade, death, lymphocyte count, and BUN level (P=0.011, P=0.024, P=0.002, P=0.007, and P=0.044, respectively) (Table 2).
DISCUSSION
To the best of our knowledge, this is the first study to measure levels of circulating MAIT cells and NKT cells in acute cholecystitis and to examine the clinical relevances of these two distinct invariant T cell levels. The present study showed that percentages and numbers of circulating MAIT cells were lower in patients than in healthy controls. Recently, MAIT cells were reported to express high levels of CCR6 and CXCR6 and intermediate levels of CCR9 (12, 14), and these chemokine receptors are known to be involved in cell trafficking to intestines and liver (22, 23, 24). Thus, a loss of circulating MAIT cells in acute cholecystitis might be due to the transmigration of these cells from blood to sites of inflammation. This notion is supported by several lines of evidence that MAIT cells number are diminished in blood but obviously elevated in the intestines of patients with inflammatory bowel disease and in the ascetic fluids of patients with ovarian cancer or active tuberculosis (12, 25, 26). In the present study, no significant differences were observed between NKT cell percentages in the peripheral blood of patients and HCs. However, circulating NKT cell numbers were found to be significantly reduced in patients. This decline in NKT cell numbers might be due to lower lymphocyte counts in patients (data not shown), as a similar finding was reported in patients with head and neck squamous cell carcinoma. In this previous study, circulating NKT cell numbers and total lymphocyte counts were significantly reduced in patients, but NKT cells per million T cells in patients and HCs were not significantly different (27).
In addition, our data also revealed that numbers of MAIT and NKT cells were negatively correlated with age in acute cholecystitis patients, which is reminiscent of a previous report that demonstrated an age-dependent decrease in circulating NKT cell numbers in cancer patients and HCs (28). Similarly, we previously reported circulating MAIT and NKT cell numbers are affected negatively by age in healthy subjects (21, 29). These findings show that an age-related decline in these invariant T cell numbers can be expected regardless of patients or healthy subjects.
We also found that reductions in NKT cell numbers are associated with TG13 grade and death (i.e., disease severity and outcome). However, correlations between NKT cell numbers and grade or death might be obtained because all of these parameters are age-dependent. Thus, in the present study, age was included as a control variable in a partial correlation analysis and correlations were reanalyzed. It was found that death (r=-0.485, P=0.008), but not TG13 grade (r=-0.265, P=0.165), retained its association with NKT cell deficiency after this adjustment, which suggests that screening for NKT cell levels in blood samples could be used to predict prognosis in acute cholecystitis. Interestingly, this prognostic value of circulating NKT cell levels was also addressed in a previous study on head and neck cancer (27).
The present study has some limitations that require consideration. The study was performed on small populations with unbalanced sex ratios and narrow age ranges (41-83 yr). Furthermore, selection bias may have been caused by the inclusion of patients with pathologically proven acute cholecystitis in a tertiary-care regional referral center. Thus, patients with mild cholecystitis were not included in this study. Moreover, male (76.7%) and elderly (mean age, 66.7 yr) patients accounted for the majority of the patients, and several studies have reported patients with more severe cholecystitis tend to be male and that elderly patients have more severe grades (i.e., grade III) (2, 3). In addition, levels and functions of circulating immune cells are known to be affected by several factors, such as drugs and invasive procedures (30, 31). To exclude the possibility that MAIT and NKT cell levels were affected by these factors, blood samples were obtained before surgery and study subjects with a history of drug exposure (e.g., steroid or immunosuppressant use) were excluded. Nonetheless, follow-up analyses of MAIT and NKT cell levels before and after treatment are required to evaluate changes in these cell levels according to disease activity. Further investigations for large populations with balanced sex ratios and broad age ranges are needed and in particular functional studies are required to assess MAIT and NKT cell functions and to elucidate the roles these invariant cells play in immune responses to acute cholecystitis.
Summarizing, the present study describes numerical deficiencies of circulating MAIT cells and NKT cells in acute cholecystitis and age-related declines in these invariant T cells. In addition, NKT cell deficiency was found to be associated with disease severity or outcome. These findings provide important information regarding the monitoring of changes in circulating MAIT and NKT cell levels during disease course and predicting the prognosis of acute cholecystitis.



 XML Download
XML Download