

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hemoptysis is bleeding originating from the lower airways; it has a wide clinical spectrum that can reach life-threatening dimensions. The most important causes of hemoptysis are bronchiectasis, chronic bronchitis, tuberculosis, and malignancy (1). Etiological causes are usually investigated with chest radiography, computed tomography (CT), and bronchoscopy. Etiological causes cannot be identified in 7%-22% of cases, and the condition is defined as cryptogenic hemoptysis (2). Angiography and bronchial artery embolization (BAE) are important modalities allowing for rapid diagnosis and treatment in hemoptysis (3). Management of cryptogenic massive hemoptysis is difficult and surgery is not a reasonable option, as there is no underlying, identifiable pathology. The current study was performed to evaluate CT and angiographic findings and BAE outcomes in cryptogenic hemoptysis.
MATERIALS AND METHODS
In this retrospective study, we evaluated patients who had undergone BAE from January 2005 to January 2013 due to cryptogenic hemoptysis. Additionally, the angiography findings and the BAE results in patients with cryptogenic hemoptysis were compared with those in patients with non-cryptogenic hemoptysis in the same period. Diagnosis of cryptogenic hemoptysis was made in those without any specific disease history (e.g., bronchiectasis, tuberculosis, malignancy), when no endobronchial and parenchymal abnormalities (except for hemorrhagic findings) were observed after the patients were examined by bronchoscopy and CT, and when the laboratory findings were normal. In our hospital, hemoptysis is classifying as mild (< 30 mL/24 hr), moderate (30-100 mL/24 hr), and severe (> 100 mL/24 hr), and angiography and BAE is performing in severe hemoptysis. All patients were hospitalized, and standard treatment was administered to correct hypoxemia and hemodynamic instability with fluid replacement and blood products. All patients underwent chest radiography, thorax CT, and fiber-optic bronchoscopy to identify the cause of hemoptysis and localize the side with bleeding.
Angiography was performed on all patients using the right femoral approach with a Philips Allura XPER FD DSA machine. First, non-selective angiography was performed with a 5F pigtail catheter to visualize the aortic arch and thoracic aorta and to investigate the bronchial artery anatomy and the presence of systemic collateral vessels. Then, a 4F or a 5F Cobra or Simmons catheter were used to catheterize the bronchial artery on the bleeding side and visualize it with a nonionic contrast medium. Ipsilateral intercostals arteriograms and, when necessary, subclavian arteriograms were obtained by selective catheterizations. Bronchial arteriography criteria that can lead to a diagnosis of hemoptysis are bronchial artery enlargement, hypervascularization, bronchial-to-pulmonary shunting, and extravasation of the contrast material into the bronchial lumen. Following selective catheterization of the bleeding bronchial artery or other systemic artery, embolization was performed under fluoroscopic guidance by using 355-500 µm polyvinyl alcohol (PVA) particles (Contour; Boston Scientific, Natick, MA, USA).
Statistical analysis
To compare the angiographic findings and the outcomes of embolization in the cryptogenic and non-cryptogenic hemoptysis groups, Fisher's exact test was used. All analyses were performed using SPSS for Windows version 22.0. A two-sided P value less than 0.05 was considered statistically significant.
RESULTS
Cryptogenic hemoptysis
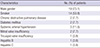
This study evaluated 26 patients (19 men, 7 women) with a mean age of 40.4 yr (range, 20-60 yr) who received endovascular treatment after being diagnosed with cryptogenic hemoptysis. Table 1 lists clinical characteristics of patients.
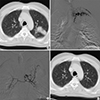
All patients had chest radiography. In 13 patients (50%), these were normal, and in the other 13 patients (50%), they were abnormal, showing alveolar infiltrates or consolidation. CT examination was performed on all patients. Upon CT imaging, 20 patients (76.9%) had ground-glass or scattered nodular infiltrates, while 6 patients (23.1%) had hazy consolidation. In addition to infiltrates, 1 patient (3.8%) also had liquefied material in segmental and lobar bronchi, and 1 patient (3.8%) had a mass image that disappeared on the fourth day after the BAE (Fig. 1). In all cases, bronchoscopy was performed before angiography to identify endobronchial lesions that could cause hemoptysis. Bronchoscopy identified active bleeding and the blood clot that showed the bleeding side. The side of bleeding identified at bronchoscopy was compatible with CT findings, in all patients. Nine patients (34.6%) had only left lung hemorrhage, while 16 patients (61.5%) had only right lung hemorrhage. One patient (3.8%) had hemorrhage in both lungs. Hemorrhage was located to upper lobe in 14 patients (53.8%), lower lobe in 7 patients (26.9%), and right middle lobe in 2 patients (7.7%). Three patients (11.5%) had hemorrhage in multiple lobes.
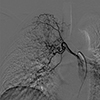
Diagnostic angiography revealed abnormalities in all patients. While all patients had bronchial artery abnormalities, 4 patients (15.4%) also had systemic artery abnormalities, including 3 patients (11.5%) who had intercostal artery abnormalities and 1 patient (3.8%) who had abnormalities of 1 lateral thoracic artery and 2 intercostal arteries (Fig. 2). The most commonly detected abnormalities of bronchial artery were dilatation in 18 patients (69.2%) and hypervascularity in 25 patients (96.2%) (Fig. 3). Four patients (15.4%) had bronchial-to-pulmonary shunting while 4 patients (15.4%) had extravasation into the bronchial lumen. In addition to bleeding bronchial artery branches, 18 patients (69.2%) exhibited hypervascularities in contralateral bronchial arteries and/or ipsilateral bronchial artery branches other than bleeding lobar branches (Fig. 3, 4). Intercostal and lateral thoracic arteries abnormalities were also dilatation and hypervascularity.
Bronchial arteries were investigated bilaterally in 10 patients. Of those, 7 patients had bronchial artery abnormalities on both sides (Fig. 4). In 3 of 10 patients, the bronchial artery on the bleeding side was thinner than the bronchial artery on the opposite side (Fig. 4). Interestingly, 71.4% of the patients (5 patients) with bilateral bronchial artery abnormalities were smokers.
Hemoptysis ceased in all patients after embolization. Embolization was repeated in 3 patients (11.5%) after 1, 6, and 7 months, respectively, as there was mild recurrence of hemoptysis. In the remaining 23 patients (88.5%), hemoptysis was not observed during long-term follow up. After the last embolization, no hemoptysis was reported during a mean follow-up period of 29.2 ± 15.6 months (6-61 months). There were no major complications related to the procedure.
Non-cryptogenic hemoptysis
A total of 152 patients (97 men, 55 women) with a mean age of 47.5 yr (range, 25-85 yr) who received endovascular treatment after being diagnosed with non-cryptogenic hemoptysis were evaluated. Of those, 22 patients (14.5%) were smokers.
CT examination revealed bronchiectasis in 95 patients (62.5%), cavitary lesion in 26 patients (17.1%), pleuroparenchymal fibrotic changes due to tuberculosis in 16 patients (10.5%), lung cancer in 11 patients (7.2%), and metastasis in 4 patients (2.6%). All of the patients also had infiltrates and/or consolidation in the CT images. Of the patients with non-cryptogenic hemoptysis, 87 (57.2%) had unilateral lung abnormality, while 65 (42.8%) had abnormality in both lungs; moreover, 134 patients (88.2%) had abnormality in more than one lobe.
Diagnostic angiography revealed abnormalities in all of the patients. While all of the patients had bronchial artery abnormalities, 54 (35.5%) also had nonbronchial systemic artery abnormalities, including abnormalities in the intercostal artery, thyrocervical trunk, internal mammary artery, and lateral thoracic artery. The most commonly detected abnormalities of the bronchial artery were dilatation in 80 patients (52.6%) and hypervascularity in all patients (100%). Thirty-nine patients (25.7%) had bronchial-to-pulmonary shunting while 2 (1.3%) had extravasation into the bronchial lumen. A comparison of the bronchial artery abnormalities between the cryptogenic and noncryptogenic hemoptysis groups showed that only extravasation was statistically significant in the cryptogenic hemoptysis group than the non-cryptogenic hemoptysis group (P = 0.004), while the other bronchial artery abnormalities had no significant difference between groups (for all, P > 0.05). Conversely, the involvement of the nonbronchial systemic artery was significantly greater in the non-cryptogenic hemoptysis group than the cryptogenic hemoptysis group (P = 0.044).
Of the 65 patients with bilateral lung abnormalities in CT examinations, 55 had bilateral bronchial artery abnormalities in angiography. Of the 87 patients with unilateral lung abnormalities, 38 were investigated for bilateral bronchial arteries, and no abnormality was identified in the contralateral bronchial artery. Only 5 patients with unilateral lung abnormality who were investigated for bronchial artery bilaterally (as both bronchial arteries originated from a trunk) were smokers.
Because most of the patients had diffuse parenchymal disorders in the lung(s), they also had diffuse bronchial artery abnormalities. Only 18 patients (11.8%) had abnormality in one lobe of the lung in the CT images, and abnormalities in the ipsilateral bronchial artery branches, other than bleeding lobar branches, were not identified in any of the patients. Of those patients, only 3 were smokers.
Hemoptysis ceased in all patients after embolization. Recurrence of hemoptysis appeared 14 days to 21 months after the embolization in 38 patients (25%). Of those, 20 (13.2%) were reembolized 1 to 6 times, as the hemoptysis was severe. Other patients were treated medically. Recurrence of hemoptysis had no statistically significant difference between the cryptogenic and non-cryptogenic hemoptysis groups (P = 0.205).
DISCUSSION
Diagnostic radiological examinations used for hemoptysis are chest radiography and thorax CT. The role of CT is identification of the cause of bleeding and pulmonary lobe with bleeding. In cryptogenic hemoptysis, the cause of bleeding cannot be identified; CT findings show infiltration and/or consolidation on the bleeding side parenchyma and liquefied material in the bronchial system. In addition to these findings, the current study found a mass image that resolved after BAE in one patient. The mass image arose as a result of hemoptysis; it was not the cause of hemoptysis. This state shows that diagnosis of a tumor cannot be done until a control CT examination reveals an unresolved mass image after the BAE. To the best of our knowledge, this resolving CT finding in cryptogenic hemoptysis has not been reported previously in the literature.
The efficacy and safety of BAE in treating hemoptysis caused by various etiologies has been analyzed in both the short term and long term. In 90% of cases, embolization stops the bleeding immediately, and 70% of patients do not have hemoptysis recurrences during one year of follow up (4, 5). In the current study, hemoptysis was ceased immediately after the embolization in all patients with non-cryptogenic hemoptysis, while 75% of those patients had no recurrence of hemoptysis in the long follow-up period. In contrast to hemoptysis with known etiologies, in cryptogenic hemoptysis, information about the role of BAE is limited. A limited number of studies evaluating the role of BAE in cryptogenic hemoptysis have reported that bleeding stopped immediately after embolization in 85%-95% of cases (2, 6, 7). In one of these studies, 15% of the cases had recurrences in three months (7). For cryptogenic hemoptysis cases that have undergone BAE, long-term follow-up results are insufficient. In the current study, BAE was efficient at immediately controlling hemoptysis in all cases. Mild recurrence of hemoptysis occurred in three cases (11.5%), and re-embolization was performed. While the rate of recurrence of hemoptysis was lower in the cryptogenic hemoptysis group than the non-cryptogenic hemoptysis group, there was no statistically significant difference between the groups. Otherwise, the recurrence of hemoptysis was mild in the cryptogenic hemoptysis group; in contrast, the most severe hemoptysis recurrence occurred in the non-cryptogenic hemoptysis group. Furthermore, only one re-embolization was sufficient in the recurrence of cryptogenic hemoptysis, while multiple re-embolizations were needed in the recurrence of non-cryptogenic hemoptysis. In all cases with cryptogenic hemoptysis, after the last embolization, no hemoptysis occurred during a mean follow-up period of 29.2 ± 15.6 months.
The angiography findings in cryptogenic hemoptysis cases cited in the literature are bronchial artery enlargement, hypervascularization, retrograde bronchial-to-pulmonary shunting, and contrast extravasation into the bronchial lumen (2, 3, 6, 7). The current study found that dilatation of the bronchial artery and hypervascularity were the most commonly detected abnormalities, consistent with previous reports. In contrast, in this study, extravasation into the bronchial lumen occurred slightly more often than in previous reports. Comparison of the angiographic findings for the cryptogenic hemoptysis patients and the non-cryptogenic hemoptysis patients showed no significant difference in bronchial artery enlargement, hypervascularization, and bronchial-to-pulmonary shunting, while extravasation into the bronchial lumen was significantly greater in the cryptogenic hemoptysis patients than in the non-cryptogenic hemoptysis patients.
Bronchial artery dilatation is reported as the most common angiographic finding. In our study, in 30% of the cryptogenic hemoptysis patients who had bilateral bronchial arteriography, the bronchial artery on the bleeding side was thinner than the contralateral bronchial artery. This finding made us conclude that other angiography findings, such as hypervascularization, bronchial-to-pulmonary shunting, and contrast extravasation into the bronchial lumen, were more valuable and significant as diagnostic findings.
An important finding of the current study was that 69.2% of patients with cryptogenic hemoptysis had, in addition to bleeding bronchial artery branches, hypervascularities in contralateral bronchial arteries and/or ipsilateral bronchial artery branches other than bleeding lobar branches. Menchini et al. (7) reported bilateral bronchial artery abnormality in 76% of the patients who underwent bronchial arteriography bilaterally. Although the current study found similar results; Hypervascularity in ipsilateral bronchial artery branches other than bleeding lobar branches was also found. To the best of our knowledge, this angiography finding has not been reported previously in the literature. In contrast to the cryptogenic hemoptysis cases, in the non-cryptogenic hemoptysis cases the contralateral bronchial artery and the ipsilateral bronchial artery branches, other than the bleeding lobar branches, had no abnormalities.
Another important finding of the current study was the abnormality of nonbronchial systemic arteries in 4 patients (15.4%). In hemoptysis, nonbronchial systemic artery abnormalities are observed during inflammatory conditions with the involvement of pleura (8). Our cases were regarded as cryptogenic hemoptysis, as they did not have any parenchymal or pleural abnormalities. To the best of our knowledge, abnormality of the nonbronchial systemic artery in cryptogenic hemoptysis has not been reported previously in the literature. In the current study, as expected, abnormalities of the nonbronchial systemic arteries were significantly greater in the non-cryptogenic hemoptysis group than in the cryptogenic hemoptysis group.
Angiographic findings show us that there are conditions affecting one or both lungs widely in the pathophysiology of cryptogenic hemoptysis. The fact that 53.8% of our patients smoked supports this hypothesis, because smoking has chronic inflammatory effect. In recent years, the literature has mentioned the relationship between smoking and cryptogenic hemoptysis (2, 7). Smoking induced inflammatory changes are seen mostly on the upper zones of the lungs (7, 9, 10). Supporting this, a study reported bleeding in the upper lobes in 71% of the cryptogenic hemoptysis cases in smokers (7). Similarly, the most effected side of lung is the upper lobe in our study.
The goal of BAE is to stop systemic arterial inflow in fragile vessels in the pathological region of the lungs, thereby decreasing perfusion pressure and preventing bleeding (11). The objective in endovascular treatment of hemoptysis is occlusion of the bleeding distal bed, and the embolic material used should be particles. Absorbable gelatin sponge can be used in embolization; however, as it resorbs over time and recanalizes, it is not a preferred embolic material for hemoptysis. The most commonly used embolization material in BAE is PVA particles. PVA is biocompatible and nonbiodegradable, providing for permanent embolization (12). We used PVA when performing BAE on our patients and did not encounter any significant complications, either during or after the procedure. Trisacrylgelatin microspheres also are being used now as embolization material in BAE (3).
The complications of BAE are quite limited and can be related to the femoral arterial approach, selective catheterization or embolization. The main complications are arterial occlusion, perforation, dissection, pseudoaneurysm, arteriovenous fistula, hemorrhage, non-target embolization and postembolization syndrome. The major risk of the BAE is the paraplegia caused by occlusion of the spinal artery. In the present study, no treatment complications occurred.
A limitation of the current study is that it focused only on patients with cryptogenic hemoptysis who underwent transarterial embolization and excluded patients who received other medical or surgical treatments. The study sought to evaluate arterial abnormalities and embolization results in cryptogenic hemoptysis.
In conclusion, bronchial artery dilatation is one of the most commonly observed angiographic findings, yet hypervascularization, bronchial-to-pulmonary shunting, and contrast extravasation are considered more valuable and significant in cryptogenic hemoptysis. Angiographic findings show that whatever the underlying cause for cryptogenic hemoptysis, it involves the lung(s) in a diffuse manner. Nonbronchial systemic arteries can also be affected in cryptogenic hemoptysis. BAE is an effective and reliable treatment option for cryptogenic hemoptysis, with excellent short-term and long-term results.


 XML Download
XML Download