

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Fibroblast growth factors (FGFs) have diverse biologic functions, such as cell differentiation, cell growth, angiogenesis and wound healing (1). FGF-family consists of 22 members and most are demonstrated to play an important role as paracrine factors (2).
Recently, a subfamily which include FGF-19, FGF-21 and FGF-23 are considered to be endocrine factors (3). FGF-21 is an important metabolic regulator with beneficial effects on glucose and lipid metabolism (4). In animal model, FGF-21 is expressed mainly in the liver and stimulates glucose uptake in adipocyte by induction of GLUT1 (5). According to a recent study, skeletal muscle is other important source of FGF-21 production (6). FGF-21 is expressed and secreted from human skeletal muscle in response to hyperinsulinemia, suggesting FGF-21 is an insulinregulated myokine. Based on positive metabolic effects, FGF-21 is considered as a potential therapeutic agent to treat impaired glucose homeostasis in metabolic diseases (5).
In human study, increased level of FGF-21 are found in obese individuals (7) and are closely associated metabolic syndrome, type 2 diabetes mellitus and coronary artery disease (CAD) (8, 9). However, the role of FGF-21 in development of atherosclerosis related to glucose and lipid metabolism remains unclear. The aim of this study was to evaluate the association of plasma FGF-21 with angiographically significant CAD in patients with type 2 diabetes mellitus and non-diabetic patients.
MATERIALS AND METHODS
Subjects
A total of 120 pateints were recruited from patients who underwent coronary angiography due to chest pain between June 2009 and May 2011. Age of patients ranged from 18 to 80 yr old. Subjects with following criteria were excluded: 1) severe liver and renal dysfunction (AST and ALT of three times above the normal limit, creatinine > 2 mg/dL), 2) heart failure (left ventricular ejection fraction < 40%), 3) a history of acute myocardial infarction, 4) a history of coronary artery disease underwent coronary angiography, 5) a recent history of hematologic disease, 6) connective tissue disease, 7) valvular heart disease, and 8) pregnancy.
CAD was diagnosed angiographically and defined as a stenosis of >50% of the luminal diameter in at least one of the coronary arteries or their major branches. Patients were divided into 4 groups based on the presence/absence of type 2 diabetes mellitus and of significant CAD.
Measurement of FGF-21
Specimens for this study were provided by Pusan National University Hospital, a member of the National Biobank of Korea, which is supported by the Ministry of Health and Welfare. Serum samples were centrifuged for 20 min at 3,000 rpm and removed serum and stored at ≤-70℃. Serum concentrations of FGF-21 were analyzed by a commercial ELISA kit. Human FGF-21 immunoassay kits were purchased from BioVendor Laboratory Medicine, Modrice, Czech Republic. The assays were conducted according to the manufacturer's protocol. The samples were diluted with dilution buffer before the assay (1:1 dilution). The samples generated values higher than the highest standard were further diluted with dilution buffer and repeated the assay. All samples were run as duplicates and were within the range of the standard curve. The standard curve range for the assays was 30-1,920 pg/mL, and limit of dectection was 7 pg/mL.
Coronary angiography and quantitative scoring
All patients were catheterized percutaneously via the radial artery or via the femoral artery. The atherosclerotic burden was obtained by two independent angiographic scores: Gensini Score and Extent Score.
The Gensini score defined by narrowing of the lumen of the coronary arteries (10). With diameter reductions of 25%, 50%, 75%, 90%, 99%, and 100%, the Gensini scores were given 1, 2, 4, 8, 16, and 32, respectively. The score was mulitiplied based on the relative amount of myocardium supplied by the segment: the left main coronary artery, 5; the proximal segment of the left anterior descending (LAD) coronary artery or left circumflex (LCX) artery, 2.5; the mid segment of the LAD or LCX coronary artery, 1.5; the distal segment of LAD and LCX, first diagonal branch, first obtuse marginal branch, right coronary artery, posterior descending artery, 1; and intermediate artery, and the second diagonal and second obtuse marginal branches, 0.5. This score represents both severity and extent of coronary atherosclerosis.
The extent score was used to measure the percentage (0% to 100%) of the coronary surface involved by atheroma (11). This scoring system defined that the proportion of each vessel involved by angiographically detectable atheroma, as identified by lumen irregularity. The score was multiplied by a factor for each vessel: left main, 5; left anterior descending, 20; main diagonal branch 10; first septal perforator, 5; left circumflex, obtuse marginal, and posterolateral vessels, 10; right coronary, 20; and main posterior descending branch, 10. When the major lateral wall branch was a large obtuse marginal or intermediate vessel, the factor was given 20, and the left circumflex artery, the factor was given 10. Occluded vessels which were not filled with contrast medium and the distal vessel was not visualized, the proportion of the vessel not visualized was given the mean score of the remaining vessels.
Statistical analyses
Statistical analyses were performed using SPSS version 15.0 (SPSS, Chicago, IL, USA). Data were presented as mean±SD for normally distributed values and median (interquartile range) for nonparametric values. Differences between the groups were analyzed by ANOVA. Categorical variables were reported as frequencies and proportions. Pearson's chi-square test was performed to analyze categorical data as appropriate. We performed multiple regression analysis with the coronary artery disease severity and extent (Gensini score and extent score) as dependent variables and serum FGF-21 as independent variables, respectively. Several models were gradually built to adjust multiple confounding factors. A P value of <0.05 was considered statistically significant.
RESULTS
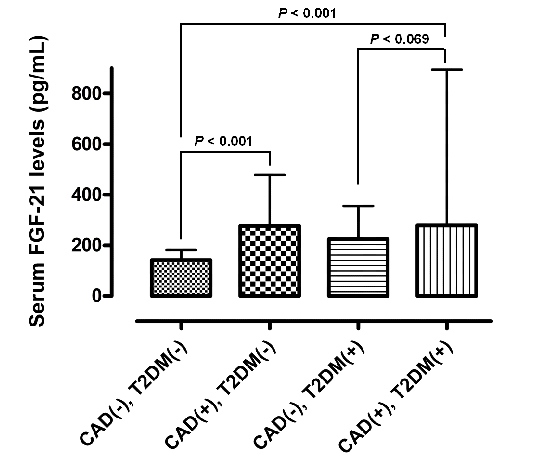
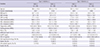
The baseline characteristics of the subjects are shown in Table 1. Metabolic and laboratory parameters were compared according to the presence/absence of type 2 diabetes mellitus and coronary artery disease. Serum FGF-21 levels were significantly higher in diabetic patients than in non-diabetic patients (P=0.014). A significant difference existed among non-diabetic patients, according to the presence or absence of significant CAD (P=0.001). However, there was no significant difference between CAD groups among diabetic patients (P=0.069) (Fig. 1).
Serum FGF-21 levels were significantly correlated with GS (r=0.358, P<0.001) and ES (r=0.324, P<0.001) in all patients (Table 2). In non-diabetic patients, serum FGF-21 levels was significantly correlated with GS (r=0.337, P=0.008), but lost significant correlation with ES (r=0.250, P=0.054). In diabetic patients, serum FGF-21 had significant correlation with both GS (r=0.384, P=0.002) and ES (r=0.381, P=0.003).
After adjusting for age, sex, BMI, history of antihypertensive, lipid-lowering and anti-platelet agents, and significant clinical parameters, both GS and ES were significantly associated with serum FGF-21 in all patients (r=0.271, P=0.014; r=0.217, P=0.041, respectively). In non-diabetic patients, serum FGF-21 levels significantly correlated with only GS in final model (r=0.262, P=0.043). However, serum FGF-21 lost significant correlation with both GS and ES (r=0.332, P=0.055; r=0.296, P=0.084, respectively) with diabetic patients in the final model (Table 2).
DISCUSSION
In the present study, serum FGF-21, which is a regulator of carbohydrate and lipid metabolism, was elevated in patients with CAD and type 2 diabetes mellitus. Despite limited role in patients with type 2 diabetes mellitus, serum FGF-21 showed significant correlation with the extent and severity of CAD in all patients.
FGF-21 was known to have unique role in the regulation of carbohydrate and lipid metabolism in the liver, adipocyte and pancreas (12). There were relatively large evidence of the role of FGF-21 in animal studies. FGF-21 is expressed in the murine liver during fasting and induces gluconeogenesis, fatty acid oxidation and ketogenesis as an adaptive response through a peroxisome proliferator-activated receptor α (13, 14, 15). Kharitonenkov et al. (5) reported that FGF-21 is a potent stimulator of glucose uptake in mouse 3T3-L1 adipocytes and therapeutic administration of FGF-21 reduced glucose and triglycerides in both ob/ob and db/db mice.
Our study showed that serum FGF-21 levels were elevated in patients with type 2 diabetes mellitus. The high levels of serum FGF-21 levels were associated with adverse lipid profile, obesity, and metabolic syndrome in other human studies (4, 9, 10). The cause of paradoxical increase of serum FGF-21 is not explained clearly. It is suggested the possibility of a compensatory response or resistance to FGF-21 (4).
Recently, An et al. (16) demonstrated that serum FGF-21 was elevated in patients with type 2 diabetes mellitus. The study also evaluated presence of diabetic complication including carotid plaque using carotid artery ultrasonography. Elevated serum FGF-21 was an independent risk factor of carotid intima-media thickness in Chinese subjects (17). This result is consistent with our report. However, we performed coronary angiography to evaluate directly the severity and extent of atheroma.
In diabetic patients, serum FGF-21 showed loss of correlation with the extent and severity of CAD in final model. However, in another study, patients with type 2 diabetes mellitus were divided according to serum FGF-21 median value of 240.7 pg/mL (18). Patients with the above level of median value were associated with a increased combined cardiovascular morbidity and mortality during a follow-up of 24 months (HR, 4.7; 95% CI, 1.67-13.24).
There were some limitations in this study. First, the present study was a cross sectional design, which had cautious interpretation about direction of causality. Second, the relatively small numbers of patients were enrolled in this study. Our study showed that loss of correlation between serum FGF-21 and extent and severity of CAD in type 2 diabetes mellitus patients after adjusting clinical parameters. A large sample size may be required for more comprehensive results with sufficient statistical power. Third, the blood samples for this study were obtained during a coronary angiography. We excluded patients with a history of heart failure, acute myocardial infarction, and other coronary artery disease. However, acute event such as chest pain could affect serum FGF-21 levels. Despite these limitations, it is notable that this is the first study using the GS and ES to evaluate atherosclerotic burden. The severity and extent of coronary atheroma was evaluated by quantitative methods.
In conclusion, the patients with type 2 diabetes mellitus and CAD feature elevated serum FGF-21 levels. Despite a limited role in diabetic patients, serum FGF-21 levels are independently associated with angiographic severity and extent of CAD. Serum FGF-21 level is a predictor of the presence or severity of CAD at high risk patients including type 2 diabetes mellitus. Future long-term follow-up studies are required to evaluate if seserum FGF-21 level is a marker as predictor of progression or death of CAD patients.


 XML Download
XML Download