

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The leading cause of death in Korea is cancer, and especially lung cancer. According to the annual report on causes of death statistics from the Korea National Statistics Office (KNSO), the rate of lung cancer death increased from 26.1 per 100,000 people in 2002 to 33.1 per 100,000 people in 2012 (1).
Although smoking is a known major risk factor for lung cancer, several cohort studies conducted in the USA, Europe, and China, have revealed that chronic exposure to radon also contributes to the occurrence of lung cancer (2). Indeed, the World Health Organization (WHO) reported that radon was the second most common cause after smoking (2). Based on the accumulated evidence, the International Agency for Research on Cancer (IARC) classified radon as a carcinogen in 1988 (3).
For that reason, USA and European nations, through national surveys, have reported concentrations of radon and its daughter species. Radon is a radioactive gas of natural origin, produced from uranium and radium. Various levels of radon exposure occur naturally across the population. Since 1989, the Republic of Korea has also reported indoor radon concentrations (4). However, there has been no report on the health risks of lung cancer due to radon exposure. Although investigations on the risk of lung cancer due to individual radon exposure are difficult, indirectly, an 'ecological approach' is possible. In this way, many countries have estimated the health risks due to radon exposure (5, 6, 7, 8). Such quantification of health risks is helpful in public health policy making and the allocation of resources.
MATERIALS AND METHODS
Radon concentration by region
In the Republic of Korea, national radon surveys were conducted in 1989, 2000, 2002-2005, and 2008-2009 to estimate the dose to the public. Kim et al. (4) reported the average distribution of indoor radon from these four surveys. Briefly, the sample sizes for each survey were 530, 2,953, and 970 dwellings, and 1,100 public buildings, respectively. The fourth survey was conducted in schools and local governmental offices. There were distinct differences by region, and the range of average exposures was 37.5 to 95.0 Bq/m3. The regional distribution of indoor radon concentrations is presented in Fig. 1. The arithmetic means of the indoor radon concentrations across the 16 administrative districts for the total survey were obtained from Kim et al. (4).
Lung cancer death data
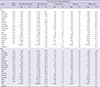
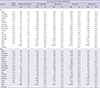
Absolute numbers of lung cancer death by gender, age, and the 16 administrative districts from the years 2000 to 2012, were obtained from the Korea National Statistical Office (1). Lung cancer deaths in those aged over 30 yr were included. During that period, 181,510 deaths due to lung cancer occurred, 73.6% of which were males (n=133,582). Thus, lung cancer was responsible for 13,962 deaths per year (Table 1).
Risk assessment of the relationship between lung cancer and radon
To estimate the lung cancer risk due to radon, models developed by the BEIR-VI Committee (9) and the European Pooling Study (10) were used. Published risk assessment studies commonly use the relationship between lung cancer and radon derived from the miners' cohort study in the US; this was published by the BEIR-VI Committee. Darby et al. (10) reported residential radon exposure risk for lung cancer using 13 general European population case control studies (7,148 cases of lung cancer and 14,208 controls). Later results were used in the global burden of disease study in 2010 (11).
Risk assessment based on evidence from BEIR-VI
The two linear excess relative risk models for lung cancer due to radon, developed by the BEIR-VI Committee, were used to estimate excess risk. These were based on extrapolations of risk models derived from 11 cohort studies of underground miners to the general population. These models are presented as linear functions of cumulative exposure, by either exposure-age-duration (the EAD model) or exposure-age-concentration (the EAC model).
To apply the BEIR-VI risk models, we assumed that all individuals in the same district were exposed equally and that the exposure concentrations were unchanged over their lifetime. The excess relative risk model developed by BEIR-VI was as follows: where β indicates the risk coefficient of the exposure-response relationship, w indicates the exposure windows, w5-14, w15-24, and w25+, the parameter θ is the relative contributions to risk, θ15-24 and θ25+, and γz represents either exposure duration or concentration, which is basically the age of the person divided by the time window 5-14, 15-24, and 25+ yr before the person's current age. Details regarding these models have been presented elsewhere (9).
As proposed by the BEIR-VI Committee, the value of β was adjusted two-fold for non smokers and 0.9 times for smokers versus the general population. To consider the risk attributable to smoking, we used the calculation methods described by Veloso et al. (8). Information about the proportion of lung cancer attributable to smoking was obtained from a large prospective Korean cohort study. In that study, Jee et al. (12) reported that the rate of death due to lung cancer among smokers was 94% for males who were current smokers, and 32% for females.
In turn, to estimate the number of lung cancer deaths attributable to radon, we used the following formula: where Nr, a, d, s indicates the number of lung cancer deaths due to radon exposure r, at age a, in district d, and for gender s. Na, d, s is the total number of lung cancer deaths at age a, in district d, and for gender s, and ERRr,a is the excess relative risk for radon exposure r and for age a.
Risk assessment based on evidence from the European Pooling Study
The risk of lung cancer from radon derived from the European Pooling Study was expressed as a linear model. Its risk coefficient was adjusted for age, gender, region of residence, and smoking status. Thus, we estimated the excess relative risk with the following formula: where β indicates the risk coefficient of the exposure-response relationship, and X is the mean radon concentration by district. The PAF and number of lung cancer deaths attributable to radon were estimated as recommended by WHO (13).
RESULTS
The average indoor radon concentration across the 16 administrative districts is presented in Fig. 1. The average indoor radon level was 62.1 Bq/m3 and it was differed by district. The concentrations was highest in Chungbuk (95 Bq/m3) and lowest in Busan (37.5 Bq/m3). During the period 2000-2010, the adjusted lung cancer mortality rate was highest in Gyeongbuk for both genders (Table 1).
Table 2 provides the estimated regional risk of lung cancer due to radon by applying exposure-response relationships. Regardless of smoking status, indoor radon accounted for 13.5%-19.5% and 20.4%-28.2% of lung cancer deaths in males and females, respectively, from the EAD and EAC models. Additionally, PAF for lung cancer was 8.3%, with reference to the European Pooling Study model; use of this model produced the fewest attributable deaths.
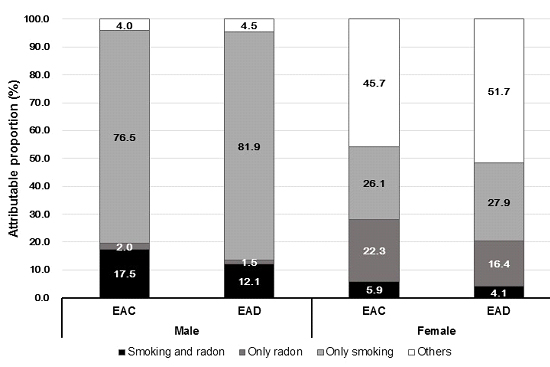
Tables 3 and 4 show the numbers of lung cancer deaths according to smoking status. In males, smoking alone produced the most attributable deaths, and radon alone, the fewest. However, in females, issues other than smoking and radon produced the most attributable deaths, and joint effects of smoking and radon, the fewest. Overall, the proportion of lung cancer deaths was higher among smokers than non-smokers in males. However, deaths attributable to lung cancer in females were higher among non-smokers than smokers; approximately twice as many deaths occurred among female non-smokers than smokers. The summary of joint effect between smoking and radon on lung cancer by gender represents in Fig. 2.
DISCUSSION
Using the exposure-response relationships from BEIR-VI and the European Pooling Study, we estimated the proportion of lung cancer deaths attributable to radon. Radon accounted for 8% to 28% of deaths, depending on lung cancer, gender, and smoking status. Overall, in the results of the BEIR-VI models, the EAC model gave higher estimates than the EAD model and the estimated proportion attributable to radon in non-smokers was higher than that in smokers. These results are consistent with previous studies conducted in various countries (5, 7, 8).
Radon is a colorless, odorless, and tasteless gas, to which humans are exposed from natural sources. Risks due to radon have come to the fore during the last two decades, but in Korea there is a lack of public concern regarding the risks posed by radon. Generally, indoor radon concentrations are higher than those of other sources of exposure, such as air and drinking water. Indoor radon concentrations depend on factors such as the soil, building materials, house type, and ventilation. Kim et al. reported that the radon distribution was correlated with the geological distribution of granite, and that the concentration in traditional Korean houses was higher than that in apartments (4).
As the second leading cause of lung cancer, after smoking, accumulated evidence supports the carcinogenicity of radon and its decay products (3). The biological mechanism of the link between radon and lung cancer is explained by deposition of decay products formed after the inhalation of radon in the lung epithelium. Although no domestic evidence regarding individual radon exposure and lung cancer is available, arbitrary quantity estimations seem to be meaningful in public health and policy decision-making. However, there has been controversy as to whether extrapolation of evidence from occupational exposure to the general population is reasonable. The fourth BEIR report recommended a correcting factor of 0.7, meaning that residential exposures were about 30% lower than those in mines, but the BEIR-VI report revised that to 1.0 (14). Additionally, several lines of evidence originating from the general population suggest that chronic low exposure to radon is a cause of lung cancer (10, 15). The American Cancer Society Cancer Prevention Study reported a 15% increase in lung cancer deaths for each 100 Bq/m3 increase in residential radon concentration (15). This is similar to the results of 13 European case-control studies (10).
Although the findings are unclear, indoor radon concentrations were not lower than the average of OECD countries. The mean radon concentrations for the Republic of Korea are 62.1 Bq/m3 (arithmetic mean) and 49.0 Bq/m3 (geometric mean) (4). These are higher than Japan and the United Kingdom, and similar to Portugal and France (2). According to a recent study on the environmental burden of disease in six European countries, the burden of radon was highest in France and lowest in the Netherlands (6). A study in the north of Portugal reported that of the total number of lung cancer cases, 18 to 28% (8) could be associated with indoor radon exposure compared with 8.3% in Switzerland, 5% in Germany (16), and 14%-16% in Canada (7, 17).
The prevalence of smoking in Korean females was relatively low compared with that in other countries (18), although it has increased gradually in recent years. Several studies estimated the risk of lung cancer attributable to radon taking into consideration joint effects with smoking (5, 8). In reports from the BEIR-VI Committee and United States Environmental Protection Agency (US EPA), smokers comprised almost 95% and 90% of lung cancer deaths in males and females, respectively (9, 14). In a study conducted in Portugal, the values were 85% in males and 21% in females (8). Compared with a large-scale prospective Korean cohort study (12), this was similar in males and higher in females. A later study in Portugal reported slightly lower numbers for both males and females. Using the values recommended by the BEIR-VI Committee, in the present study, the proportion attributable to radon was approximately 33.0% in non-smokers and 19.0% in smokers of both genders using EAC (male: 33.2% in non-smokers and 18.6% in smokers, female: 32.8% in non-smokers and 18.5% in smokers). Similarly, 40.0% in non-smokers and 24.7% in smokers were estimated to be attributable to radon in the north of Portugal (8), and 50.3% in non-smokers and 10.9% in smokers in a study conducted in France (5). With the exception of lung cancer, the American Cancer Society Cancer Prevention Study also reported a positive linear trend and 13% increase in chronic obstructive pulmonary disease mortality for each 100 Bq/m3 increase in radon concentration (19). However, no evidence of an association between radon and non respiratory deaths (20) is available.
Regarding national efforts to reduce the health risks due to radon, the Korean Ministry of the Environment has recommended that the indoor radon concentration be less than 4 pCi/L (picocuries per liter of air, equal to 148 Bq/m3), the same value as the United States Environmental Protection Agency (21). Moreover, the Korean Ministry of the Environment (KME) has suggested guidelines for reducing the radon risk, such as encouraging construction of radon-resistant buildings and improvements in ventilation systems (22). To reduce the health risk associated with radon, education of residents of high-level regions and provision of information regarding radon-related health risks are necessary.
The use of average concentrations during the fourth survey, instead of one measure, might have reduced the variation due to measurement error. However, limitations in the available data on the distribution of radon make this difficult to determine. In addition, there was also limitation in interpreting results due to study design. Using summarized data through ecological study might lead to under- or overestimation in real exposure. In estimation of the PAF, it was calculated by several risk models not based on domestic evidence, thus it has to be interpreted carefully except for international comparison under same risk models. However, this is the first reported study to quantify lung cancer deaths attributable to indoor radon exposure across the 16 administrative districts of the Republic of Korea. Furthermore, risk assessment in personal level based on national data is required.
In this study, we estimated the regional-level risk of radon-induced lung cancer deaths. These data will assist in making decisions regarding action plans for public health and the allocation of resources across the regions of Korea.

 XML Download
XML Download