

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is believed to be complex and heterogeneous, not a simple and homogeneous disorder. The varied pathological features of COPD lead to recognition of patient subgroups that have different characteristics and may have distinct responses to treatment (1). Thus, clinical responses to bronchodilators and inhaled corticosteroids (ICS) may vary among individuals (2). Therapeutic response is an important component of improved health-related quality of life and influences the clinical outcomes of the disease (3).
Many recent studies support the effectiveness of bronchodilator and anti-inflammation therapy to improve lung function in specific subgroups of COPD patients (1, 4). Several studies have found a significant relationship between the decline in lung function and poor clinical outcomes in COPD patients (5, 6, 7, 8, 9), but few have shown that improved lung function translates into improved clinical outcomes, including decreased exacerbation (10, 11).
The ability to predict whether COPD patients with improved lung function in response to bronchodilator and anti-inflammatory treatment are likely to have better clinical outcomes, including a reduction in exacerbations, is important. Treatment response to a short-acting bronchodilator like salbutamol has been used to diagnose bronchodilator reversibility (BDR). However, there is evidence that BDR does not distinguish among clinically relevant outcomes (12, 13).
A standardized therapeutic response indicator that can be used to predict the clinical benefit of long-term bronchodilator treatment is needed. This study examined whether the response of COPD patients to a 3 months treatment with a bronchodilator and anti-inflammatory agent could predict exacerbation. A cohort of 137 patients was evaluated over a 1 yr period. After 3 months of treatment, the patients were divided into two subgroups based on improvement of Forced Expiratory Volume 1 second (FEV1), and the occurrence of exacerbations in the two subgroups was compared.
MATERIALS AND METHODS
Subjects
This study was a post hoc analysis of 133 male and four female COPD patients who were selected from the Korean Obstructive Lung Disease (KOLD) cohort. All had stable COPD and were prospectively recruited from the pulmonary clinics of 14 hospitals in Korea between June 2005 and December 2012. The inclusion criteria for the KOLD cohort have been described elsewhere (14, 15). COPD was diagnosed based on the presence of airflow limitation that was not fully reversible (post-bronchodilator FEV1/forced vital capacity (FVC)<0.70) and more than 10-pack-years of smoking history.
Three-month treatment response and classification of subgroups
For all patients, the use of respiratory medicine was restricted for 2 weeks before enrollment. Baseline clinical data included demographic information, smoking history, past exacerbation history, a 6 min walk distance (6MWD) test, body mass index (BMI), pulmonary function tests and chest radiography. The modified Medical Research Council (mMRC) dyspnea scale was administered to assess the degree of dyspnea.
FEV1 was measured by spirometry after 12 weeks of treatment and expressed as a percentage compared to the predicted value for healthy Korean subjects (16). The COPD patients were classified as responders or nonresponders based on FEV1 improvement after 3 months of combined treatment with a long-acting beta-agonist and inhaled corticosteroid (LABA/ICS) (salmeterol/fluticasone, 50 µg/500 µg or formoterol/budesonide, 9 µg/320 µg). Responders were defined as having a minimal clinically important difference (MCID) (3, 17) of 120 mL or greater improvement in FEV1 after treatment, and nonresponders were defined as having an FEV1 improvement of <120 mL.
Obligatory study visits were scheduled every 3 months for 1 yr. Trained research coordinators recorded medical history, smoking history and status, information on previous treatments, and compliance with inhaler use. The investigators were not included in the interview process. Patients were asked to bring their inhalation device to each study visit so that medication use could be measured. Ninety percent of subjects answered that they used more than 80% of the recommended medication doses. We educated patients about the method of using inhaler devices at the enrollment. Also we had checked that patients properly used the inhaler at the visit of 3 months.
Pulmonary function tests
Spirometry was performed as recommended by the American Thoracic Society using a Vmax 22 instrument (Sensor-Medics, Yorba Linda, CA, USA) or a PFDx machine (MedGraphics, St. Paul, MN, USA) (18). To assess short-acting BDR, FEV1, FVC, and FEV1/FVC were evaluated before and 15 min after inhalation of salbutamol (400 µg) using a metered-dose inhaler (MDI) fitted with a spacer. The predicted values of FEV1, FVC, and FEV1/FVC were calculated from equations formulated using data from a population of healthy nonsmoking Koreans (16, 19).
Exacerbation identification
Patients were interviewed at the clinic every 3 months for 1 yr of follow-up. Exacerbations were identified according to previously accepted criteria of moderate or severe exacerbation in which the patients visited a clinic or an emergency department, or were hospitalized (17, 20, 21). Visit or admission to hospitals that are involved in research was traced by medical record. If patients visit other clinics other than the participating institutes, we checked exacerbation occurrence using pre-structured interview sheet including the following sentence. 'In the past three months, did you visit other clinic or emergency room due to increased sputum amount or purulent sputum or deterioration of dyspnea?' Also, we use pre-structured interview sheet for checking other clinic name, reason for visit, visit date and frequency.
Statistical analysis
Categorical data were analyzed using chi-square or Fisher's exact tests. The primary outcome was time to occurrence of the first exacerbation within the year of follow-up. Hazard ratios (HRs) and confidence intervals (CIs) were calculated by Cox proportional hazards regression. Univariate regression analyses were done to explore potential risk factors. Multivariate regression analyses were also done to examine risk factors adjusted for potential confounding covariates. All statistical analyses were performed using the SPSS statistical package (version 18.0, SPSS Inc, Chicago, IL, USA); P<0.05 was considered statistically significant.
RESULTS
Baseline characteristics of patients
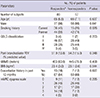
Table 1 shows the baseline characteristics of the 137 COPD patients. Patients were classified into two subgroups according to the MCID of FEV1 change before and after the 3-month treatment. Eighty patients (58.4%) were classified as responders and 57 (41.6%) as nonresponders.
There were no significant differences in age, sex proportion, BMI, post-bronchodilator FEV1, 6MWD, exacerbation in previous 12 months, patient distribution of GOLD stage, or dyspnea scale scores between the two subgroups. But, current smokers are more in responder group than in nonresponder group.
Exacerbation occurrence
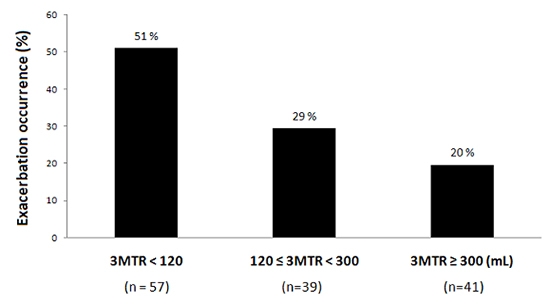
Acute exacerbations occurred in 25 patients (31.3%) in the responder group and 26 patients (45.6%) in the nonresponder group. Although it was not significant difference in exacerbation occurrence between the groups, responder group tended to show the low incidence of exacerbation occurrence (P=0.086). We further classified the responder group into two categories based on the change in FEV1, with a cut-off of 300 mL. The other cut-off of 300 mL was defined as it was near the upper tertile value. The exacerbation occurrence decreased significantly with an incremental change of the FEV1 after treatment (P=0.035, Fig. 1A). We reanalyzed relationship exacerbation occurrence with 3-month treatment response using the change of FEV1 in % of the predicted reference value. According to MCID, the responder group was defined when FEV1 improvement was 4% or more of the predicted value after 3-month treatment. The result was compared to the earlier result using absolute volume change of FEV1 (Fig. 1B). In the univariate analyses, BMI was the only other factor that was significantly related with exacerbation occurrence (Fig. 2).
Relationship of exacerbation occurrence with 3-month treatment response and other factors
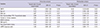
The multivariate Cox proportional hazard model adjusted for age, sex, FEV1, smoking history, 6MWD, BMI, 12-month exacerbation history, and dyspnea scale revealed that the 3-month treatment response was the only significant risk factor for exacerbation (Table 2). In this model, BDR was not independently related to occurrence of exacerbation.
DISCUSSION
We have shown that the 3-month treatment response to LABA/ICS was associated with decreased occurrence of acute exacerbations in COPD patients. Several previous studies have shown that the decline in lung function or deterioration of COPD-associated symptoms was related to a worse clinical outcome. However, this study found that lung function improvement following pharmacological intervention was related to a better clinical outcome. The results support a 3-month treatment response as a prognostic factor for exacerbation. The occurrence of exacerbation was significantly lower among responders than among nonresponders during the 1-yr follow-up period.
Recent evidence shows that COPD phenotypes cannot be classified as chronic bronchitis or emphysema, but should be seen as a complex and heterogeneous disorder. The different pathological processes of COPD make it difficult to choose medications and predict therapeutic response. An important area in COPD research is the development of more powerful, multivariate methods for predicting clinical outcomes, and responsiveness of individual patients to particular therapies, using clinical, laboratory and radiographic characteristics. Kitaguchi et al. (22) classified COPD subgroups based on bronchial wall thickening on high-resolution CT (HRCT). Similarly, Lee et al. (1) classified COPD patients based on the emphysema index on HRCT and pre-bronchodilator FEV1. They demonstrated that airway obstruction-dominant or mixed-subtype COPD patients showed significant reversibility of airflow limitation in response to short-acting bronchodilator or combined LABA/ICS treatment compared with emphysema-dominant patients. Thus, recent work has attempted to divide COPD patients into subgroups and to analyze their clinical differences.
The current COPD treatment guidelines are based on markers of disease severity such as FEV1, symptom severity, quality of life, and the frequency of exacerbation. The guidelines do not accurately predict treatment response nor do they allow for specific therapy of various COPD characteristics or personalized medicine. Therefore, it is possible to apply therapeutic strategies that are similarly effective for all patients. According to recent reports, COPD patients were classified into their categories based on their response to the specific bronchodilators; however they could not find the relation between the categories and clinical outcome (4, 12, 13, 15). For example, Albert et al. (12) evaluated BDR as a potential COPD phenotype and indicator of therapeutic response, but found that BDR was not related to any particular clinical outcome.
This study showed an improvement of FEV1 in COPD patients after 3 months of LABA/ICS treatment, which was associated with a decrease of acute exacerbation. In addition to previous studies that also reported a treatment response, our result demonstrated that the therapeutic response was related to an improved outcome, i.e., decrease of acute exacerbation.
The BODE index, which has been related to the survival rate of COPD patients, is a scoring system composed of BMI, FEV1, dyspnea, and exercise capacity, and is correctable with the appropriate treatment or the effort of the patients (23). The potential of the 3-month treatment response as a prognostic factor, together with the improvement in the BODE index, requires further evaluation. Because it is difficult to predict the appropriate therapeutic approach for individual COPD patients before beginning treatment, comparing the drug responses of individual patients is the only way to find the effective bronchodilator. We supposed the possible relation between the treatment response and the clinical outcome of the COPD patients.
Some methodological limitations of this study should be noted. First, the use of the MCID criterion and its relation to clinical outcome is subject to expert debate, and these results may assist in resolving some of the questions about the relevance of the MCID. Second, our study design was based on a post hoc analysis of the prospective cohort. In order to compensate the weakness of post hoc analysis, we analyzed multivariate model including known risk factors and probable risk factors related to exacerbation occurrence. Furthermore, a prospective study with larger sample size may be needed to confirm the relationship between the 3-month treatment response and the clinical prognosis. Third, in our study, a past history of exacerbations known as an important risk factor for exacerbation occurrence was not statistically significant. Our study excluded severe symptomatic patients who could not tolerate a washout period of 2 weeks before enrollment. Consequently, only 2% of GOLD stage IV patients were included in the study. This difference in subjects' inclusion may affect the characteristics of the study population which were different to that of the other studies. Although it was not statistically significant, it had a weak trend that the known risk factors be positive predictors to future exacerbation in our result. We believe that our findings would be more significant if such patients had been included in our study. Fourth, responder group included more current smokers than nonresponder group. We analyzed multivariate model including smoking history. It was not a significant risk factor for acute exacerbation. In recent studies, it is controversial whether current smoking is a risk factor for exacerbation or not (7, 24, 25). Fifth, the enrolled COPD patients were consistently confirmed the airflow limitation on the registration and the 3-month follow up. However, eleven patients who have possibility of asthma COPD overlap syndrome (ACOS) depend on the BDR results were included (26). Nevertheless, 3MTR was confirmed as the prognosis factor of acute exacerbation significantly on multivariate Cox proportional hazard model which excluded the potential ACOS patients (P=0.047). Finally, history of acute exacerbation was relied on patient memory, only when patients visited other clinics other than the participating institutes. Considering that the patients were elderly, this could have been underestimated. However, in our study, there were no significant differences in the baseline characteristics of the two subgroups, including age. Although patients were old, we supposed that memory of visiting hospital was hard to forget. We prevented the loss of information including exacerbation occurrence by using pre-structured interview sheet.
In conclusion, acute exacerbation occurs significantly less often among the 3-month treatment responders than among nonresponders. Further studies are needed to confirm the relationship between treatment response and additional clinical outcomes such as hospitalization or mortality.


 XML Download
XML Download