

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Retinal vein occlusion (RVO) is a common, sight-threatening retinal vascular disorder that mostly affects middle and old aged people (1). The clinical characteristics, prognosis, and response to treatment are influenced by the location of the occlusion and by the extent of retinal nonperfusion (1, 2, 3). To treat secondary macular edema (ME), the common cause of visual impairment in RVO, several treatment modalities including anti-VEGF agent, steroids, laser photocoagulation are currently used (4, 5, 6, 7, 8). The visual outcomes in patients with branch RVO (BRVO) and central RVO (CRVO) are variable between studies depending on severity of disease, systemic factors, treatment methods, etc.
Baseline predictors of visual outcome are important for determining treatment plan and understanding the nature of the disease. Baseline predictors of visual prognosis and anatomical outcomes in RVO have been investigated in a few studies. Several factors such as younger age and shorter duration of macular edema have been suggested to be predictive of better visual and anatomical outcome (9). However, only limited studies on visual outcomes and anatomical outcomes of RVO in Asian populations have been performed.
Korean RVO Study is a nationwide study performed by the Korean Retina Society. The study enrolled 557 consecutive patients with new-onset RVO from 41 clinical sites, which might be representative of the clinical features of Korean RVO patients. The baseline characteristics of enrolled patients revealed a significant association of BRVO with hypertension and CRVO with diabetes mellitus (10). In addition, female gender and old age in BRVO, and large area of intraretinal hemorrhage and macular ischemia in both RVO were significant factors related to poor baseline visual acuity.
The present study aimed to investigate baseline factors associated with visual acuity and central retinal thickness (CRT) at 6 months in patients with ME secondary to RVO in the Korean RVO Study.
MATERIALS AND METHODS
This retrospective, multicenter, interventional case series from 41 clinical sites was performed as a nationwide study from January 2010 through January 2012. The Korean RVO Study design and methods have been described previously in detail (10).
Subjects
Treatment-naïve RVO patients with new-onset (≤6 months) were initially enrolled. RVO due to other causes, RVO accompanied by arterial occlusion, and RVO accompanied by ocular ischemic syndrome were excluded. Among the 557 patients who were initially enrolled, patients with follow-up period of 6 months or more were included in the analysis.
Evaluation of the systemic factors
Detailed baseline data on demographic information, past medical history including medication, and smoking were collected. Also, each patient's complete systemic medical history related to RVO was examined for hypertension, diabetes mellitus (DM), heart disease, cerebrovascular accident, renal disease, and hyperlipidemia.
Ocular examination
Ocular findings including fundus photography, fundus fluorescein angiography and optical coherence tomography (OCT) at baseline and 6 months were retrieved. Snellen best-corrected visual acuity (BCVA), refractive error, and intraocular pressure were recorded at each examination. The fundus findings were recorded in terms of the type of RVO (CRVO or BRVO), optic disc abnormalities, involvement of macular edema, presence of neovascularization at the disc or elsewhere, extent of retinal hemorrhage, and other abnormal findings such as vitreous hemorrhage. Using early- and peak-phase fluorescein angiography (FA), abnormalities in the optic disc area, the presence of macular ischemia (eg, foveal avascular zone disruption, leakage, and intraretinal cystoids spaces), extent of capillary nonperfusion, and the presence of neovascularization in the parafoveal area were examined at baseline and 6 months. Using the horizontal and vertical OCT images, CRT, photoreceptor inner segment/outer segment (IS/OS) disruption, intraretinal cyst, and the presence of subretinal fluid, were assessed. Fundus photography, fundus fluorescein angiography and OCT were evaluated independently by two retina specialists with subsequent senior reader arbitration. Differences in CRT, depending on the OCT machine used, were corrected by manual correction of the outer retinal boundary to a standardised reference location as previously described (10, 11, 12).
Treatment
Data on treatment modalities and number of treatment were reviewed. Treatment methods, timing, and retreatment criteria were determined by each of the 53 retina specialists in 41 clinical sites. To treat ME secondary to RVO, they performed intravitreal anti-VEGF agent, intravitreal triamcinolone injection, laser treatment, and combined treatments at their own discretion.
Outcome measures
The primary purpose of this study is to predict outcomes for change from baseline in visual acuity and CRT at 6 months. Outcome measures of best corrected visual acuity (logMAR) included absolute change from baseline, a gain of ≥0.3 from baseline, and a loss of ≥0.3 from baseline. Outcome measures of CRT included absolute change from baseline, a measurement of ≤250 µm, and a measurement of ≥400 µm.
Statistical analysis
The 25 baseline variables considered in the prediction analyses for the BRVO and CRVO analyses include age, gender, diabetes, hypertension, systolic and diastolic blood pressure (BP), smoking, body-mass index (BMI), cerebrovascular accident, renal disease, use of anti-platelet agent, baseline BCVA, IOP, baseline OCT findings including central retinal thickness, external limiting membrane (ELM) disruption, intraretinal cyst, photoreceptor inner segment/outer segment (IS/OS) junction disruption, presence of subretinal fluid, treatment, number of treatment, duration of symptom, foveal hemorrhage, nonperfusion in foveal avascular zone, area of retinal hemorrhage within the ETDRS grid, and area of nonperfusion within the ETDRS grid.
Univariate analysis included descriptive summary statistics and linear regression. Paired t-test for means was used to evaluate changes in BCVA and CRT from baseline to 6 months. Chi-square test was used to evaluate associations between baseline variables and a gain or loss of BCVA ≥0.3 from baseline, and a measurement of CRT ≤250 µm or ≥400 µm. Multiple step-wise regression analysis was used to identify prognostic factors for visual outcome and CRT at 6 months.
RESULTS
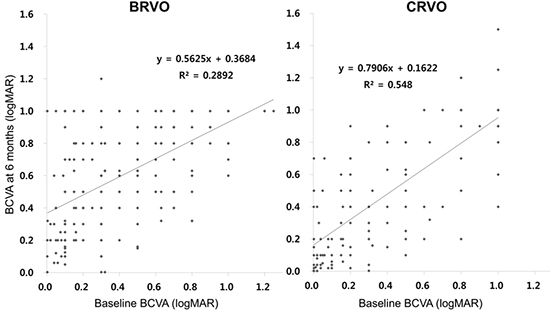
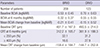
In total, 208 patients with BRVO and 123 patients with CRVO were included in the analysis. Baseline demographic, systemic, and ocular characteristics of included patients are shown in Table 1. Mean age of included patients was 57.9±10.3 yr in BRVO and 58.5±12.3 yr in CRVO. Mean CRT at baseline was 451.7±167.0 µm and 493.5±214.0 µm in BRVO and CRVO, respectively. Among the included patients, 67.3% and 71.5% of patients with BRVO and CRVO, respectively, were treated with anti-VEGF agents (Table 1). Table 2, Fig. 1, and Fig. 2 provide summary of BCVA and CRT change during the 6 months. Mean BCVA change from baseline was -0.21±0.41 and -0.15±0.52 in BRVO and CRVO, respectively (Table 2). At 6 months, 37.0% and 32.5% of patients with BRVO and CRVO, respectively, showed a BCVA gain of ≥0.3 from baseline (Fig. 1B). At 6 months, mean CRT was 312.2±105.7 µm and 361.9±188.3 µm in BRVO and CRVO, respectively (Table 2).
The number of participants at 6 months follow-up visits is less than the number of enrolled eyes because of participant drop-out. Whether the drop-out patients show different clinical features from analyzed patients, major systemic and ocular factors were compared between the two patient groups. In patients with BRVO, there are no differences in age, gender, smoking, hypertension, BMI, baseline BCVA, baseline CRT, and duration of symptoms. In patients with CRVO, patients with hypertension were more common and duration of symptoms was shorter in the drop-out patients.
Univariate analysis for BCVA at 6 months in patients with BRVO and CRVO were performed. Univariate analysis in patients with BRVO revealed that BMI, baseline BCVA, baseline CRT, foveal hemorrhage, anatomic abnormal findings on OCT including intraretinal cyst, ELM disruption, subretinal fluid, and duration of symptom were significantly associated with BCVA change from baseline. Higher BMI, male, worse baseline visual acuity, higher CRT, larger area of hemorrhage, presence of intraretinal cyst, ELM disruption, presence of SRF on OCT, and shorter duration of symptom were associated with a BCVA gain of ≥0.3 from baseline. On the contrary, larger area of nonperfusion on FA was associated with a loss of ≥0.3 from baseline. In CRVO, worse baseline BCVA was associated with BCVA improvement from baseline. Higher BMI, worse baseline visual acuity, higher CRT, and presence of intraretinal cyst and SRF on OCT were associated with a BCVA gain of ≥0.3 from baseline.
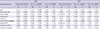
The results of multiple step-wise regression analysis revealed that worse baseline BCVA was associated with a positive visual acuity change in patients with BRVO (Table 3). For BRVO, younger age, worse baseline visual acuity, and shorter duration of symptom were significantly associated with a BCVA gain of ≥0.3 from baseline. For CRVO, only one factor, worse baseline visual acuity, was associated with positive visual acuity change and a BCVA gain of ≥0.3 from baseline.
Univariate analysis for CRT at 6 months in patients with BRVO and CRVO were performed. Univariate analysis in patients with BRVO revealed that baseline BCVA, baseline CRT, anatomic abnormal findings on OCT including intraretinal cyst, ELM disruption, IS/OS disruption, subretinal fluid, and treatment were significantly associated with CRT change from baseline. Smoking and number of treatment were associated with a CRT ≤250 µm at 6 months. On the contrary, higher baseline CRT, absence of intraretinal cyst on OCT, and number of treatment were associated with an increased likelihood of a CRT ≥400 µm at 6 months. Univariate analysis in patients with CRVO revealed that systolic BP, BMI, baseline BCVA, baseline CRT, and IOP were significantly associated with CRT change from baseline. Smoking and lower baseline CRT were associated with a CRT ≤250 µm at 6 months. On the contrary, DM, non-smoking, and higher baseline CRT were associated with an increased likelihood of a CRT ≥400 µm at 6 months.
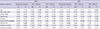
For central retinal thickness outcomes, the results of multiple step-wise regression analysis revealed that higher baseline CRT predicted greater decrease at 6 months in both BRVO and CRVO (Table 4). For BRVO, younger age was associated with an increased likelihood of measurement of a ≤250 µm outcome. For CRVO, higher baseline visual acuity was associated with an increased likelihood of measurement of a ≤250 µm outcome. Smoking was associated with greater decrease from baseline and decreased likelihood of measurement of a CRT ≥400 µm at 6 months.
DISCUSSION
This study investigated baseline factors associated with visual acuity and CRT at 6 months in 331 Korean patients with RVO. At 6 months, about one-third of patients with RVO showed a BCVA gain of ≥0.3 from baseline. For BRVO, younger age, worse baseline BCVA, and shorter duration of symptom were predictive of more gain in BCVA at 6 months. For CRVO, only worse baseline visual acuity was associated with more gain in BCVA at 6 months. In terms of CRT, higher baseline CRT predicted greater decrease at 6 months in both BRVO and CRVO. For BRVO, younger age was associated with an increased likelihood of measurement of a ≤250 µm outcome. For CRVO, higher baseline visual acuity was associated with an increased likelihood of measurement of a ≤250 µm outcome.
In patients with BRVO, younger age was associated with a BCVA gain of ≥0.3 at 6 months. This finding is consistent with the results of the Standard Care versus Corticosteroid for Retinal Vein Occlusion (SCORE)-BRVO study, but the Branch Vein Occlusion Study (BVOS) did not reveal the association of age with visual acuity outcome in patients with BRVO (9, 13). Moreover, in BRVO, younger age was also associated with an increased likelihood of measurement of a CRT ≤250 µm. In younger patients, retinal tissue might be less vulnerable to acute vascular compromise with higher likelihood for both functional and anatomical recovery. In patients with CRVO, however, age was not associated with visual acuity outcome. On the contrary, in the SCORE-CRVO study, there was a significant association between treatment effect and age, although the odds ratio was only 0.96 (9).
In patients with BRVO, shorter duration of symptom was also significantly associated with a BCVA gain of ≥0.3 at 6 months. However, shorter duration of symptom was not predictive of less CRT at 6 months. On the contrary, SCORE-BRVO study showed that shorter duration of macular edema was associated with improvement in center point thickness, but not with functional outcome. Shorter duration of macular edema in our study (mean 32±33 days) compared to SCORE-BRVO study (mean 4.4±3.8 months) may explain, at least in part, the difference (14). This finding suggests that, to achieve functional recovery, prompt treatment may be beneficial in BRVO. Also, this might imply that prolonged ME is associated with irreversible damage of neuronal cells in retina, even after anatomic recovery is achieved. Association of shorter duration of macular edema and improved functional recovery was also demonstrated in the ranibizumab for the treatment of macular edema following Branch Retinal Vein Occlusion (BRAVO) study and the Ozurdex-GENEVA study (4, 6).
For BRVO and CRVO, worse baseline BCVA was associated with a BCVA gain of ≥0.3 and more gain in BCVA at 6 months. This is consistent with the results from the SCORE-BRVO study (9). This finding should be interpreted with caution, in that worse baseline BCVA did not predict better BCVA at 6 months. The finding may partially be explained by a greater opportunity for visual acuity improvement in patients who start out with poorer visual acuity. Because worse baseline BCVA was closely correlated with BCVA at 6 months, those with worse baseline BCVA were at greatest risk of continued poor vision in both BRVO and CRVO.
Results of univariate analysis for BCVA at 6 months in patients with BRVO and CRVO also suggest the possible associations of baseline factors with visual acuity at 6 months. In both BRVO and CRVO, intraretinal cyst and SRF on OCT were associated with a BCVA gain of ≥0.3 at 6 months. This might imply that intraretinal and subretinal fluid significantly affect visual acuity, but the visual deterioration are reversible to some extent. In BRVO, foveal hemorrhage and area of hemorrhage within the ETDRS grid were associated with positive visual acuity change. This finding may be explained by the results from SCORE-BRVO study showing that dense macular hemorrhage was associated with a lower center point thickness (9).
For OCT outcomes, higher baseline CRT predicted greater decrease at 6 months in both BRVO and CRVO, which is consistent with the results from the SCORE-BRVO and SCORE-CRVO studies (9). This finding, as mentioned above for BCVA change, may partially be explained by a greater opportunity for CRT improvement in patients who start out with thicker CRT. Thicker baseline CRT was not significantly associated with an increased likelihood of measurement of a ≥400 µm or a decreased likelihood of measurement of a ≤250 µm outcome by multiple regression analysis. This suggests that high CRT at baseline does not necessarily mean high risk of continued retinal thickness.
In patients with CRVO, higher baseline visual acuity was associated with an increased likelihood of measurement of a ≤250 µm outcome. The finding may partially be explained by the possibility that patients with higher baseline visual acuity may have less severe vascular compromise with subsequent more likelihood of anatomical restoration in the retina. For CRVO, smoking, which was not included in the baseline variables in the prediction analyses in SCORE study, was associated with greater decrease from baseline and decreased likelihood of measurement of a CRT ≥400 µm at 6 months (9). Smoking was shown to be associated with the development of BRVO, diabetic macular edema, and uveitic macular edema (15, 16, 17). However, the association of smoking with visual outcome of macular edema has not been investigated. The exact role of smoking in CRVO with macular edema is further to be investigated.
This study has several limitations. First, the treatments were not randomized and the treatment methods were not uniform. Because the treatment modality and timing solely depended on the discretion of each of the 53 retina specialists, differences in treatment modality might affect visual outcome. However, most patients were treated with anti-VEGF agents and each of the physicians adopted methods that were effective for RVO with ME. This may minimize the effect of inter-physician variability on visual outcome. Second, at 6 months, 208 (58.8%) and 124 (61.1%) of initially-enrolled patients with BRVO and CRVO, respectively, were followed-up. Therefore, these high drop-out rates may cause selection bias. However, baseline characteristics of patients who completed 6 months of follow-up compared to patients who were lost to follow-up were not significantly different in patients with BRVO. In CRVO, hypertension was less common and symptom duration was longer in patients who completed 6 months of follow-up. Although these differences may cause selection bias, the degree may not be great, because the two parameters were not shown to be predictive of visual acuity at 6 months from both univariate and multivariate analysis.
Despite several limitations of our study described above, this study provides useful clinical information on visual and anatomical outcome of RVO and baseline predictors of visual acuity and CRT at 6 months, in a real world clinical setting. Moreover, because our study enrolled treatment-naïve, consecutive patients as a nation-wide study, the results may clearly reflect the current practices in Korea.
In conclusion, several baseline factors are associated with visual acuity and CRT outcomes at 6 months in patients with ME secondary to BRVO and CRVO. The baseline factors include baseline visual acuity, baseline CRT, age, and duration of symptom. These factors may help to predict disease course for patients with RVO.



 XML Download
XML Download