

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute lymphoblastic leukemia (ALL) is the most common childhood malignancy, and its cases show favourable outcomes with a 5-yr event-free survival of about 80% (1). To attain a good prognosis, central nervous system (CNS)-directed therapy is an essential component (2). CNS-directed therapies mainly comprise of cranial irradiation, intravenous methotrexate, intrathecal chemotherapy, or a combination of these modalities. Among these CNS-directed therapies, it is reported that cranial irradiation has detrimental effects on neurocognitive outcome (3, 4). However, neurocognitive outcomes after chemotherapy without cranial irradiation are inconsistent. Although some investigators have shown similar declines in intelligence after treatment without cranial irradiation (5, 6), most studies suggested that children treated without cranial irradiation fare better than children treated with cranial irradiation (7, 8). A young age at diagnosis (9) and being female (10) appear to be risk factors for poor intelligence after cranial irradiation. Detrimental effects on intelligence quotient often progress as survival time increases (11). Specific neurocognitive domains like academic performance (12), memory and learning (13), attention and concentration (14), information processing speed (15), visuospatial skills (16), psychomotor functioning (17), and executive functioning (18) were reported to be impaired.
Long-term neurocognitive outcomes of ALL survivors have been conducted mainly in Western population. There have been few studies in Asian populations (19, 20), and only one study on a Korean population performed at 1995 until now (21). Therefore, we investigated long-term neurocognitive outcomes to discover risk factors associated with poor neurocognitive function in a cohort of Korean childhood ALL survivors.
MATERIALS AND METHODS
Enrolment of ALL survivors
Children who had been treated for ALL between January 2003 and December 2006 were recruited from the Department of Pediatrics, Seoul St. Mary's hospital, College of Medicine, the Catholic University of Korea. Criteria for inclusion in this study were: 1) patients whose primary language was Korean; 2) continuous complete remission since the initial diagnosis; 3) no CNS leukemia at diagnosis; and 4) age at time of testing between 5 and 15 yr. Criteria for exclusion were: 1) pre-existing neurologic conditions affecting behavioural development (cerebral palsy, developmental delay or mental retardation, and Down syndrome); 2) acute and chronic neurologic sequelae during treatment (seizures and leukoencephalopathies); 3) ALL relapse; and 4) hematopoietic stem cell transplantation.
Among 200 patients diagnosed with ALL between January 2003 and December 2006, 84 children met these criteria after medical record review. They were invited to this study between July 2011 and February 2012. Of the 84, 42 (50%) consented to enrol (ALL group). Reasons for failure to enrol included the following: 1) Thirty four families declined participation, and 2) eight families withdrew consent during assessment. The study participants did not differ from the 42 non-participants in gender, age at diagnosis, or treatment.
As a control group, 42 age- and sex-matched healthy children were selected. They were selected at random from the local population registry. The demographic and clinical characteristics of each participant are shown in Table 1.
Treatment of ALL
The patients diagnosed with ALL between 2003 and 2004 had been enrolled into CMCPL2001 (Catholic Medical Centre Protocol ALL 2001) protocol (n=21), and between 2003 and 2004 into CMCPL2005 protocol (n=21). Patients were stratified into 4 risk groups based on age at diagnosis, initial peripheral white blood cell counts, initial steroid response, leukemic cell type, CNS involvement, and specific chromosomal translocation. The patients were assigned to different prophylactic CNS regimens, according to protocol and a defined risk factor. In CMCPL2001 protocol, CNS-directed treatment consisted of cranial irradiation, intrathecal chemotherapy and systemic methotrexate. If patients were older than 2 yr at diagnosis, cranial irradiation was administered (1,800 cGy). Patients younger than 2 yr were treated with high dose methotrexate (5.0 g/m2) with triple intrathecal chemotherapy instead of cranial irradiation. Age-adjusted intrathecal chemotherapy was administered 6 or 8 times according to risk group. A total cumulative dose of intravenous methotrexate of 19 g/m2 to 24 g/m2 was also administered according to risk group. In CMCPL2005 protocol, CNS-directed treatment consisted of only intrathecal chemotherapy and systemic methotrexate. Age-adjusted intrathecal chemotherapy was administered 13 to 22 times according to risk group. A total cumulative dose of intravenous methotrexate of 37 g/m2 to 47 g/m2 was administered according to risk group.
Battery of neurocognitive tests
Neurocognitive function assessments were performed in a quiet room by a single trained examiner between July 2011 and February 2012. The test battery consisted of the Korean Educational Development Institute-Wechsler Intelligence Scale (KEDI-WISC), Children's Colour Trails Test™ (CCTT), Stroop Colour and Word Test: Children's Version (STROOP), and Attention Deficit Hyperactivity Disorder Diagnostic System (ADS). The examiners were unaware of a given child's primary diagnosis and treatment status at all times. Total time for assessment was about 2.5 hr. All tests were performed without cost to patient families.
Assessment of intelligence: KEDI-WISC
KEDI-WISC is the Korean version of the Wechsler Intelligence test based on the Wechsler Intelligence Scale for Children-Revised 1974 edition. The test is comprised of two subscales, the Verbal IQ (VIQ) and the Performance IQ (PIQ), which combined to yield the Full Scale IQ (FSIQ) that has a mean of 100 and a standard deviation (SD) of 15 points.
Assessment of executive function: CCTT and STROOP
The CCTT is the Korean version of the Colour Trails Test. CCTT is an individually administered, orthographic (paper and pencil), neuropsychological instrument designed to provide an objectively scored measure of sustained visual attention, sequencing, psychomotor speed, and cognitive flexibility (22). All data are presented as T-scores adjusted for age and gender. Higher T-scores indicate better function.
The STROOP is the Korean version of the Stroop Colour-Word Test. This test measures selective attention and cognitive flexibility (23). All data are presented as T-scores adjusted for age and gender. Higher T-scores indicate better function.
Assessment of attention: ADS
The ADS is a Korean version of the Test of Variables of Attention standardized to Korean cultural background. The ADS is a computerized test to diagnose and evaluate treatment effect of attention deficit hyperactivity disorder (24). Lower T-scores indicate better attention and response inhibition ability.
Statistical analysis
Demographic variables were compared with either chi-square tests or Student t-tests depending on whether the variables were categorical or continuous. Statistical analyses of long-term neurocognitive outcomes were conducted to answer 2 questions:
1) How does the ALL group perform relative to the control group?
2) How do the scores for the cranial irradiation, sex, age at diagnosis of ALL, elapsed time from diagnosis to assessment, and ALL risk group effect long-term neurocognitive outcomes?
For the first step, the ALL group was compared with the control group using independent t-tests. Additionally, the ALL group was separated into 2 groups according to patients whose treatment protocol included cranial irradiation (irradiation group) or did not (non-irradiation group). Each group was also compared using independent t-tests. The ratio of children who performed poorly on neurocognitive tests (lower than -1 SD from mean score) was compared between ALL and control groups using a chi-square test.
For the second step, to assess possible effects of the 5 potentially relevant variables (cranial irradiation, sex, age at diagnosis of ALL, elapsed time from diagnosis to assessment, and ALL risk group) on each neurocognitive test score, a linear multiple regression analysis was calculated.
All statistical analyses were two-tailed, and P<0.05 was taken to indicate statistical significant. All analyses were performed using SPSS (version 19.0, SPSS Inc., Chicago, IL, USA).
RESULTS
Comparison between groups
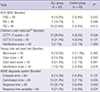
Forty-two children with ALL, 25 males and 17 females, were entered in this study. Mean age±SD at diagnosis was 3.8±2.3 yr, at assessment was 10.5±2.4 yr, and elapsed time from diagnosis to assessment was 6.6±1.3 yr. Forty-two healthy controls with the same male-to-female ratio and 10.5±2.2 yr of age were assessed (Table 1).
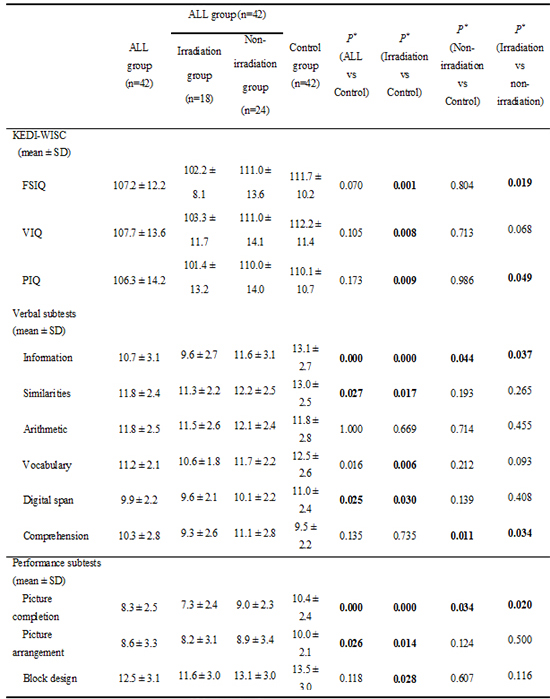
Patients with ALL had lower FSIQ, VIQ, and PIQ than healthy controls; nevertheless, none of these comparisons were statistically significant. However, the irradiation group showed a statistically significantly lower score in FSIQ (irradiation, 102.2±8.1 vs. non-irradiation, 111.0±13.6, P=0.019; vs. control, 111.7±10.2, P=0.001), VIQ (irradiation, 103.3±11.7 vs. non-irradiation, 111.0±14.1, P=0.068; vs. control, 107.7±13.6, P=0.008), and PIQ (irradiation, 101.4±13.2 vs. non-irradiation, 111.0±14.0, P=0.049; vs. control, 110.1±10.7, P=0.009) than non-irradiation and control groups. The irradiation group also performed significantly worse on several KEDI-WISC subtests (information, comprehension, and picture completion) than the non-irradiation group (Table 2).
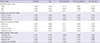
The ALL group showed worse CCTT1 time, CCTT2 time, STROOP word score, ADS commission error, and response time compared to the control group. There was no statistical difference in CCTT, STROOP, and ADS test scores between irradiation and non-irradiation groups. However, the irradiation group showed worse CCTT1, CCTT2, ADS commission error, and response time compared to the control group. In contrast, the non-irradiation group showed worse scores only in CCTT1 and response time compared to the control group (Table 3).
Compared to the control group, more children from the ALL group performed poorly on neurocognitive tests (lower than -1 SD from mean score) such as FSIQ, VIQ, PIQ, CCTT1, ADS commission error, and response time (Table 4).
Risk factors analysis of long-term neurocognitive outcomes
In multiple linear regression analysis, there was a statistically significant effect of irradiation on FSIQ (beta=0.360, P=0.019); irradiation correlated with a lower FSIQ. There was a statistically significant effect of sex on PIQ (beta=0.430, P=0.009); being male was correlated with a significantly lower PIQ. There also was a statistically significant effect of age at diagnosis on omission error (beta=-0.386, P=0.028), and response time variability (beta=-0.353, P=0.045); a younger age at diagnosis with ALL correlated with a high score in omission error and response time variability (Table 5).
DISCUSSION
In this study, we found that although survivors of ALL were similar to controls on all neurocognitive tests, we found that irradiation made the key difference; patients who had undergone irradiation treatment had lower FSIQ, VIQ, and PIQ than the non-irradiation group and controls. These results are consistent with most other reports that demonstrate the deleterious effects of cranial irradiation on the developing brain in ALL survivors (3, 4, 7, 8, 9, 25, 26, 27). Decline in overall IQ scores in ALL patients treated with cranial irradiation is clinically significant because these patients often require special accommodations to their academic programming. Because of the negative association between cranial irradiation and cognition, many ALL treatment protocols now exclude cranial irradiation. If cranial irradiation is used for the worst cases, close monitoring of neurocognitive function and efforts toward early remediation should be offered.
Although one report showed that irradiated male survivors with ALL have lower FSIQ (26), most other investigations reported greater risk for females than males in relation to cognitive outcome (20, 25, 28). Therefore, it was assumed that females are more vulnerable to cranial irradiation and CNS-directed chemotherapy. Gender differences in brain maturation, such as the smaller white matter increase in girls during childhood (29), may explain divergent vulnerabilities between males and females. As the rates of myelination of various brain regions during childhood development differ between sexes, cranial irradiation and CNS-directed chemotherapy interference with myelination may have different results (30). In our study, male survivors had lower PIQ that may result from a larger proportion of males (52.0%) than females (29.5%) exposed to cranial irradiation.
Patients diagnosed with ALL at a younger age suffer greater cognitive deficits than patient diagnosed at an older age, especially patients treated with cranial irradiation (9, 20, 30, 31). Nevertheless, in our study, we could not establish any relationship between age at ALL diagnosis and degree of deficit. Our treatment protocol excluded cranial irradiation if patient age at ALL diagnosis was under 24 months. As a result, all 5 patients who were under 24 months showed fairly good full-scale IQ (107.2±12.5), potentially accounting for the lack of age affect.
As patients with ALL treated with cranial irradiation age, they show progressively worsening neuropsychological test results (11, 32, 33). In our study, elapsed time from diagnosis to assessment did not show any effects on neurocognitive outcomes, likely because our study employed a cross-sectional design and a relatively short elapsed time from diagnosis to assessment (4-9 yr). Therefore, to clarify cumulative age-dependent effects of ALL treatment on neurocognitive function, longitudinal studies in a Korean population are needed.
In our study, there was no statistically significant difference in executive function and attention between irradiation and non-irradiation groups. However, the ALL group also showed poor executive function (measured by CCTT and STROOP test) and attention (measured by ADS) than the control group. Specifically, ALL patients showed poor simple attention (measured by STROOP word), sequential information processing (measured by CCTT1), active selective attention (measured by CCTT2), impulsiveness (measured by ADS commission error), and sustained attention and concentration (measured by ADS response time). Our findings are consistent with the reports that many ALL survivors experience post-treatment deficiencies in attention, concentration, and executive functioning (25, 34, 35). The survivors of pediatric cancer demonstrate improvement on measures of attentional functioning with pharmacological interventions used traditionally for the treatment of attention deficit hyperactivity disorder (36, 37, 38). However, childhood cancer survivors may experience more adverse side effects to stimulant medications relative to their healthy peers (39, 40). Therefore, it might be beneficial to ALL survivors that; 1) appropriate screening for executive function, attention, and concentration; 2) judicious selection for potentially remediable ALL survivors with stimulant medication; and 3) careful monitoring of stimulant side effects.
We conclude that ALL survivors have subtle long-term neurocognitive issues. In particular, cranial irradiation has significant deleterious effects on global intellectual function. Although ALL survivors treated without cranial irradiation did not show global intellectual functional deficits, they (together with ALL survivors with cranial irradiation) had specific neurocognitive deficits impacting attention, concentration, and executive function. Irradiation and being male and younger are weakly associated with poor neurocognitive function. Thus, the possible delayed cognitive effects of ALL treatment and its impact on quality of life requires continuous monitoring and management.
 XML Download
XML Download