

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Late-onset hyponatremia (LOH), hyponatremia occurring after two weeks of age with the achievement of full feeding in preterm infants, is the result of a negative sodium balance caused by a combination of inadequate sodium intake and renal or intestinal salt wasting. The incidence, severity, and duration of LOH are influenced by the maturity of the neonate's kidneys; there is a higher fractional excretion of sodium at lower gestational ages, and feeding protocols control the amount of sodium supplied to the premature baby (1, 2, 3). Because breast milk has relatively low sodium content, feeding breast milk without a fortifier can result in LOH in premature infants. Hypoxia, medications and respiratory distress can also aggravate LOH associated with kidney tubular damage. However, few studies have addressed the incidence and risk factors for hyponatremia after full feeding is achieved.
The influences of LOH on neonatal outcomes in growing preterm infants are also not well studied. Growth restriction has been observed in animals (4) and humans (5) with hyponatremia. Associations with impaired brain growth, poor neurodevelopmental outcomes (6), and sensory neural hearing loss have also been suggested (7). However, all of the above reports have focused on the relationship between LOH and overall hyponatremia, rather than hyponatremia after the achievement of full feeding. Very little is known about the influence of LOH on neonatal outcomes in preterm infants.
The goals of our study were to identify the risk factors for LOH in preterm infants and to assess the influence of LOH on neonatal outcomes.
MATERIALS AND METHODS
Subjects and definitions
Our retrospective cohort was composed of 196 preterm infants born before 34 weeks of gestation and admitted to the neonatal intensive care unit of Seoul National University Children's Hospital between June 30, 2009 and December 31, 2010. Thirty-five infants were excluded (20 died, 5 underwent ileostomies, 6 had congenital anomalies, and 4 had missing data), leaving 161 infants who were enrolled as the study population. The data were collected via a retrospective chart review. The collected data included the infants' perinatal histories, clinical characteristics (including LOH), and neonatal outcomes. The neonatal outcomes included the duration of hospitalization and the occurrence of bronchopulmonary dysplasia (BPD), periventricular leukomalacia, extrauterine growth retardation, osteopenia of prematurity, and retinopathy of prematurity requiring surgery.
LOH was defined as hyponatremia that occurred more than two weeks after birth or after oral feeding had reached 120 mL/kg/day. Hyponatremia was defined as a sodium level ≤132 mEq/L or between 133 and 135 mEq/L with oral sodium supplementation. According to our nutritional policy, total parenteral nutrition was started from birth and also protein and lipid supplementation was started at day 1. Sodium supplementation was started after diuresis begins according to the capillary or serum sodium level. We accepted sodium levels checked by capillary sample via i-STAT® Portable Clinical Analyzer (PCA, Abbott, Princeton, NJ, USA) as a guideline for sodium supplementation to avoid too many blood samplings in infants, however, we tried to check serum sodium level if possible. Trophic feeding is started as soon as feeding is tolerable and breast milk fortifier is added from the time when feeding reached 50 mL/kg/d. We added 1 pack of fortifier in 50 mL of breast milk. The amount of fortifier was not adjusted individually and Similac® or Enfamil® human milk fortifier was used (15-16 mg of sodium/4 package). In our unit, oral sodium supplementation is sometimes provided during the conversion from partial parenteral nutrition to full enteral feeding if the parenteral nutrition included high amounts of sodium. If there is a hyponatremia, we routinely checked sodium level every 1-3 days to assess whether hyponatremia is relieved. Three patients (1.8%) who had received supplementation with oral sodium chloride (NaCl) powder whose sodium levels between 133 and 135 mEq/L were included in the study population because we thought those level is low normal range and it can be a concealed case of true hyponatremia with treatment. We used the serum sodium level to define hyponatremia; however, if only a capillary sodium level measured with an i-STAT® Analyzer was available, we used that level in the analysis. The duration of hyponatremia was defined as the length of time when the sodium level was ≤132 mEq/L.
Oligohydramnios was defined as the single deepest pocket of less than 2.0 cm. Maternal pregnancy induced hypertension, preeclampsia, and eclampsia were all categorized as maternal hypertensive disorders. Respiratory distress syndrome was defined when there was any requirement of more than 40% of supplemental oxygen to maintain oxygen saturation over 85% with characteristic chest radiographic appearing within the first 24 hr of life. Patent ductus arteriosus was defined as receiving either medical or surgical treatment. Necrotizing enterocolitis was defined as higher than grade 2 according to modified Bell's staging criteria. BPD was identified using a definition suggested by Jobe and Bancalari (8) in a National Institute of Child Health and Human Development workshop. The use of antibiotics was limited to aminoglycoside and vancomycin because these medications were known to cause nephrotoxicity. Osteopenia of prematurity was defined as a serum alkaline phosphatase level over 800 IU/L or evidence of radiologic abnormality such as cupping, fraying or decreased bone density. Extrauterine growth retardation was defined as a body weight below the 10th percentile at a gestational age of 35 weeks. Metabolic acidosis was defined as base deficit of more than 6 or a bicarbonate level of less than 18 mM/L.
Statistical analysis
All the numerical data are expressed as the means±standard deviation. The t-test or the Mann-Whitney test was used for continuous variables. The chi-square test or Fisher's exact test was used for the analysis of categorical variables.
To evaluate the risk factors for LOH, we compared the perinatal factors of the LOH and non-LOH groups during the study period. A multiple logistic regression using a stepwise selection was employed, and we included significant variables (those with P values below 0.05) in a univariate analysis.
To assess the influence of LOH on neonatal outcomes, the relationships between perinatal factors and neonatal outcomes were first analyzed with a simple linear regression or a simple logistic regression due to the possibility of multicollinearity among the prenatal risk factors (explanatory variables) and the measures of neonatal outcomes (outcome variables). Each explanatory variable that was correlated with the outcome variables was also analyzed using multiple linear regressions or multiple logistic regressions. Because gestational age can influence the entire perinatal outcome, we applied a statistical correction for this factor. We also assessed the influence of LOH that persisted for at least 7 days on neonatal outcomes when compared to the group of no LOH or LOH lasting less than 7 days using the same statistical methods. The statistical analysis was conducted using SPSS Statistics version 20 and R version 2.15.1.
RESULTS
Clinical characteristics of the LOH group
There were 49 infants who had LOH, accounting for 30.4% of the infants enrolled in the study. The mean gestational age of the LOH group was 28.0±2.6 weeks (minimum-maximum; 23.4-33.3 weeks), and their mean birth weight was 989.3±362.7 g (420-2,050 g). The mean onset of LOH was 24.3±10.2 days after birth (14-51 days), and the mean duration of LOH was 5.31±3.89 days (1-17 days). Of the 49 infants with LOH, 17 (34.7%) experienced a LOH duration of at least 7 days. Oral sodium chloride supplementation was provided to 37 of the hyponatremic patients (75.5%), including 14 of the 17 neonates whose LOH persisted at least seven days. The mean replacement duration was 16.8±11.9 days (3-45 days). There were no infants with serious neurologic complications associated with hyponatremia.
Risk factors for LOH
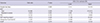
The LOH group had a lower gestational age and a lower birth weight than did the non-LOH group (P<0.01). Premature rupture of the membranes occurring more than 18 hr before the delivery, the use of prenatal antibiotics, respiratory distress syndrome, patent ductus arteriosus requiring medical or surgical treatment, postnatal culture-proven sepsis, and the use of postnatal antibiotics or furosemide within two weeks after birth occurred significantly more frequently in the LOH group (P<0.05). Feeding with breast milk was more common, and the mean duration of parenteral nutrition was longer in the LOH group (P<0.05) (Table 1).
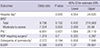
According to the multiple logistic regression analysis, a shorter gestation, a shorter duration of parenteral nutrition, the presence of respiratory distress syndrome, the use of furosemide, and feeding with breast milk were independently associated with the development of LOH (Table 2).
LOH and neonatal outcomes
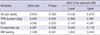
BPD, retinopathy of prematurity, osteopenia of prematurity, and a longer hospitalization occurred more frequently in the LOH group, according to the univariate analyses (Table 1). After the multiple linear or multiple logistic regression was performed, including all the perinatal factors found to be significantly associated with each neonatal outcome, LOH was found to be independently associated with a longer hospitalization (beta=8.279, P=0.009, 95% confidence interval, 2.140-14.418) and with increased rates of BPD (odds ratio 16.9, P=0.029, 95% confidence interval, 1.329-214.873) and retinopathy of prematurity (odds ratio, 4.9, P=0.028, 95% confidence interval, 1.186-20.053, Table 3).
The multiple linear or logistic regression analyses of the influence of LOH lasting at least 7 days on neonatal outcomes when compared to the group of no LOH or LOH lasting less than 7 days revealed correlations with a longer hospital stay (beta=14.595, P=0.005, 95% confidence interval, 4.554-24.635) and with higher rates of periventricular leukomalacia (odds ratio 6.881, P=0.007, 95% confidence interval, 1.684-28.119), moderate to severe BPD (odds ratio 7.224, P=0.002, 95% confidence interval, 2.008-25.990), and extrauterine growth retardation (odds ratio, 6.395, P=0.018, 95% confidence interval, 1.370-29.851) (Tables 4 and 5).
DISCUSSION
In our study, 30.4% of preterm infants born before 34 weeks of gestation were affected by LOH. Despite the relatively small sample size and limitation of a retrospective study, this is, to our knowledge, the first description of the incidence of late-onset hyponatremia. The significant risk factors for LOH were a lower gestational age at birth, a shorter duration of total parenteral nutrition, the presence of respiratory distress syndrome, furosemide use, and feeding with breast milk. LOH was also significantly associated with a longer hospital stay and the development of BPD and retinopathy of prematurity. In addition, LOH lasting for at least 7 days was significantly associated with a longer hospital stay and the development of moderate to severe BPD, periventricular leukomalacia, and extrauterine growth retardation when compared to no LOH or LOH lasting less than 7 days.
Some of the suggested pathophysiological causes of LOH in premature babies are inadequate sodium intake and increased natriuresis, which can cause increased vasopressin. Our risk factor analysis supports these pathophysiological factors as causes of LOH. In preterm infants, the immaturity of the proximal renal tubule can cause the decreased reabsorption of sodium. Numerous factors affecting the proximal tubule can aggravate hyponatremia, including hypoxia, respiratory distress, and the administration of drugs with tubular toxicity. Our study showed that the infants' gestational age at birth and birth weight tended to be lower in the LOH group and that respiratory distress syndrome was a significant risk factor for LOH. Another significant risk factor was furosemide, a well-known diuretic that affects kidney tubules, causing massive natriuresis. Regarding inadequate sodium supplementation, a shorter duration of parenteral nutrition and feeding with breast milk were significant risk factors. Although the mean total parenteral nutrition duration was longer in the LOH group, the multiple logistic regressions showed that a shorter duration of total parenteral nutrition was a risk factor for LOH. In our unit, the amount of sodium supplementation in parenteral nutrition is decided based on the serum sodium level, and it sometimes increases by up to 8-9 mEq/kg/day. However, when oral feeding without sodium supplementation begins, the amount of sodium intake suddenly decreases to 2-3 mEq/kg/day during the conversion from parenteral nutrition to enteral feeding. A shorter duration of parenteral nutrition can therefore lead to less sodium administration, which can initiate LOH. Although we used fortified breast milk, feeding with breast milk was found to be associated with the development of LOH. This finding may suggest that the current commercial fortification of breast milk is not sufficient for the sodium intake needs of preterm infants.
In the present study, the incidence of LOH was as high as 30.4%. It will therefore be of great importance to clarify the clinical consequences of a low serum sodium level in premature babies. Some preliminary data have already indicated that neonatal sodium deficiency may have unfavorable consequences for later cognitive functions (6, 9). Furthermore, hyponatremia has been documented to be a risk factor for cerebral palsy in extremely premature babies (10). In our data, there was no significant association between the presence of LOH and periventricular leukomalacia during hospitalization. However, in infants with LOH that lasted longer than 7 days, LOH was significantly associated with the development of periventricular leukomalacia.
In our study, LOH influenced the development of BPD and retinopathy of prematurity. There have been reports that excessive fluid and water balance with hyponatremia within one week after birth were associated with the development of BPD (11), and restricted water intake tended to reduce the risk of BPD (12). In preterm infants, increased natriuresis due to renal tubular immaturity can lead to protracted volume contraction, which can stimulate aldosterone and arginine vasopressin (AVP) release, allowing further water retention and the progression of late hyponatremia (1, 13, 14). The elevation of plasma AVP levels in BPD infants both during the fourth week of life and as a chronic condition has also been reported (15, 16). Although an impaired renal response to AVP in hyponatremic patients prevents the further worsening of hyponatremia (1), elevated AVP levels in BPD patients can cause pulmonary fluid to accumulate, increasing pulmonary edema; therefore, LOH may be a significant risk factor for BPD. According to our results, LOH lasting at least 7 days was significantly associated with only moderate to severe BPD. This result may indicate that a longer duration of LOH is associated with the development of more severe BPD.
Postnatal growth retardation related to hyponatremia has also been reported (5). Sodium is a significant growth factor that stimulates cell proliferation and plays a significant role in protein turnover (17). NaCl deprivation inhibits growth, which is manifested in reductions in body weight, brain weight, body length, muscle and brain protein and RNA content, and brain lipid content (compared with controls). Subsequent NaCl supplementation restores the growth velocity; however, it does not induce catch-up growth (17). In our study, extrauterine growth retardation was not related to LOH, with a marginally significant P value. However, in infants with LOH lasting at least seven days, LOH was significantly associated with the development of extrauterine growth retardation.
We performed an outcome analysis to examine the influence on neonatal outcomes of not only LOH in general but also LOH lasting for more than 7 days because we hypothesing that the duration of hyponatremia is a highly critical factor that can affect neonatal outcomes. Among the infants who had experienced LOH for at least 7 days, 14 (14/17, 82.4%) infants were supplemented with oral sodium. Although it may be a mild form of hyponatremia, a longer duration of LOH can affect many neonatal outcomes, including the development of moderate to severe BPD, periventricular leukomalacia, and extrauterine growth retardation.
This was a retrospective, observational study; therefore, it had several limitations. First, our unit has a relatively general policy of sodium supplementation and the treatment of hyponatremia, rather than a strict, uniform protocol. We therefore had to include in the LOH group some neonates with sodium levels that were not below 132 mEq/L with oral sodium supplementation; three such patients were included in the study population. We thought that these patients would have a higher chance of mild hyponatremia corrected with sodium supplementation; however, there is still a very slight possibility that those patients included infants with a normal sodium level. Second, because we usually provided sodium supplementation if there was any chance of hyponatremia, we could not determine the natural course of untreated hyponatremia. The median nadir sodium level of the LOH group was 131±2 mEq/L (range 126-134 mEq/L), and there was no patient with a nadir sodium level less than 125 mEq/L. As a result, there was no direct serious neurologic complications such as seizure or cerebral edema due to hyponatremia. Third, we included ten infants with only a capillary sample to confirm hyponatremia in the LOH group. Although this is a limitation of a retrospective study, there are many reports of a good correlation between conventional laboratory testing (serum blood) and the i-STAT® portable analyzer (capillary blood) (18, 19). Fourth, because this was a retrospective study, we could not checked the sodium level at regular intervals like randomized, controlled trials, so the duration of hyponatremia can be somewhat influenced according to the interval of blood sampling. However, the study was performed only in one hospital, and we consistently checked sodium level every 1-3 days according to the same protocol of clinical management about hyponatremia, we can assume that there will be no big difference from the real duration of hyponatremia. Fifth, only 161 patients were included in the analysis, which could influence the statistical outcome. Indeed, the confidence interval for the BPD analysis was wide, which may have been influenced by our small sample size. Therefore, the possibility remains that LOH may be only a marker of disease severity in preterm infants, although we attempted to correct for all of the possible confounding factors in the analysis.
In summary, LOH occurred at a relatively high frequency. LOH may be a risk factor for BPD and ROP; LOH lasting longer than 7 days was associated with the development of periventricular leukomalacia, moderate to severe BPD, and extrauterine growth retardation. This result exemplifies the importance of serum sodium monitoring and supplementation for the correction of hyponatremia, especially if the LOH persists for long periods despite a lack of acute symptoms. Nonetheless, as this was a retrospective study, LOH might be only a marker of disease severity rather than an etiologic factor. Thus, further large cohort studies are needed in this area.


 XML Download
XML Download