

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cor pulmonale is defined as structural changes and functional deterioration of the right ventricle (RV) resulting from pulmonary hypertension (PH), which is associated with various lung, upper airway, and chest wall diseases (1). The main pathophysiology of PH is chronic alveolar hypoxia, resulting in vasoconstriction and vascular remodeling (1). Chronic obstructive pulmonary disease (COPD) is the most common cause of cor pulmonale, and lung diseases complicated by cor pulmonale are associated with frequent hospitalizations and poor survival (2,3,4). However, data on cor pulmonale in Korea are very limited.
Brain natriuretic peptide (BNP), a cardiac hormone secreted by the cardiac ventricles, is frequently used as a noninvasive marker of left ventricular dysfunction (5). However, its levels also increase in proportion to the degree of RV dysfunction, and it is also a non-invasive marker for PH (6). In a study by Nagaya et al., a high BNP level was an independent factor associated with mortality in patients with idiopathic pulmonary arterial hypertension (IPAH) (7). Song et al. also demonstrated that BNP levels were a prognostic factor in patients with idiopathic pulmonary fibrosis (IPF) (4). In a large-scale, observational United States registry study of IPAH, BNP levels were also a significant predictor for 1-yr mortality (8). However, data are limited on the role of BNP levels in patients with cor pulmonale whose RV functions were decompensated. Therefore, in this study, we hypothesized that as in acute decompensated left-heart failure, BNP could also play a role in patients with chronic cor pulmonale whose dyspnea was acutely aggravated.
In this retrospective analysis, we compared the 1-yr outcomes among different underlying etiologies of cor pulmonale and also evaluated the association of admission BNP levels with outcomes in patients with chronic cor pulmonale who were admitted for dyspnea aggravation.
MATERIALS AND METHODS
Study population
This was a retrospective study conducted at three university hospitals (Kangdong Sacred Heart Hospital, Hallym University Sacred Heart Hospital, and Chuncheon Sacred Heart Hospital). Adult patients (age≥18 yr) with cor pulmonale who were admitted for aggravating dyspnea (between January 2007 and September 2011) were enrolled. All patients had an underlying chronic lung disease, and the diagnosis of chronic cor pulmonale was based on both clinical evidences and echocardiography data. Clinical evidences were as followings: physical evidence of peripheral edema, increased intensity of pulmonary component of the second heart sound or tricuspid regurgitation murmur; chest radiography demonstrating an increased width of right descending pulmonary artery or RV enlargement; electrocardiogram demonstrating p-pulmonale, right axis deviation or RV hypertrophy (9). With regard to echocardiography, RV hypertrophy or dilation accompanying PH (RV systolic pressure> 35 mmHg) were required for the enrollment (9,10,11). However, only patients with follow-up data available for 1 yr after hospital discharge were finally enrolled.
Exclusion criteria were as follows: the presence of left ventricular dysfunction (ejection fraction<50 mmHg on echocardiography or electrocardiographic evidence of ischemic change) or a history of coronary heart disease; admission due to other causes, including active infections; no follow-up data for the subsequent 1 yr; end-stage renal disease; immunocompromised or uncontrolled cancer; cardiopulmonary resuscitation; cardiac shunt (right to left shunt); or a do-not-resuscitate state.
Data collection and analysis
For all of the patients, we collected demographic and clinical data on admission, including age, gender, smoking history, dyspnea grade (as described by the New York Heart Association [NYHA]), home O2 therapy, and underlying lung diseases as the cause of cor pulmonale. The diagnosis of underlying lung diseases was based on laboratory and radiological data, as well as clinical diagnosis by physicians. For a diagnosis of COPD, patients had to satisfy the spirometric criteria for airflow obstruction (i.e., a post-bronchodilator forced expiratory volume in 1 s [FEV1]/forced vital capacity [FVC] ratio of less than 70% of the predicted value) (12); and the diagnosis of tuberculosis-destroyed lung (TDL) was based on a clear history of past tuberculosis with a finding of parenchymal destruction (i.e., volume loss) (13). For a diagnosis of bronchiectasis, bilaterally dominant bronchial dilation and wall thickening on chest computerized tomography (CT) were needed.
Laboratory parameters, such as complete blood cell counts, arterial blood gas analysis, cardiac troponin I, and routine chemistry were investigated. Regarding BNP levels and echocardiographic findings, admission data were collected, and if available, their follow-up data were also collected; we calculated the differences between admission and follow-up data for BNP levels and RV systolic pressure (i.e., delta BNP and delta RV systolic pressure, respectively). However, regarding pulmonary function tests (i.e., FVC% and FEV1%), those performed within 1 yr prior to the admission were used. For patients' 1-yr outcomes, data were collected based on a thorough chart review; for patients whose outcome data were uncertain (n=3), we contacted them or their family by telephone.
We compared 1-yr mortality rates among different etiologies of cor pulmonale, and also investigated the associations of admission BNP levels with subsequent readmission (due to dyspnea aggravation) and mortality rates at the 1-yr follow up. For secondary outcomes, correlations between BNP levels at admission and other parameters (e.g., troponin I levels, RV systolic pressure, PaO2, and PaCO2) were evaluated, and the role of BNP levels in predicting subsequent readmissions (i.e., cut-off value, sensitivity and specificity) was also investigated.
Plasma BNP levels
At all three hospitals, the plasma BNP levels were determined in EDTA-plasma using a microparticle enzyme immunoassay (BNP, Abbott Diagnostics, TX, USA, ARCHITECT i200SR) with intra-assay and inter-assay coefficients of variation of 2.81% and 4.40%, respectively. The measurement for the Archetect BNP assay ranges from 10 pg/mL to 5,000 pg/mL, with a total imprecision≤5.3% (14). In this study, all BNP levels were obtained within 1 hr after presentation to the emergency room or after admission.
Troponin I levels
For the measurement of troponin I levels, ARCHITECT i2000SR immunoassay analyzer (Abbott Diagnostics, TX, USA; measurement range, 0.00-50.0 ng/mL; Hallym University Sacred Heart Hospital), ADVIA Centaur XP immunoassay system (Siemens Medical Solutions Diagnostics, Tarrytown, NY, USA; measurement range, 0.006-50.0 ng/mL; Chuncheon Sacred Heart Hospital), and UniCel DxI 800 immunoassay analyzer (Beckman Coulter, Villepinte, France; measurement range, 0.03-80.0 ng/mL; Kangdong Sacred Heart Hospital) were used. In this study, all troponin I levels were also obtained within 1 hr after presentation to the emergency room or after admission.
Echocardiography
Echocardiography (Hallym University Sacred Hospital, Vivid i, GE Ultrasound System, Tirat Carmel, Israel; Kangdong Sacred Heart and Chuncheon Sacred Heart Hospitals, Vivid E9, GE Ultrasound System, Horten, Norway) was performed using standard transthoracic windows with a 2.5-MHz transducer. Tricuspid regurgitant flow was identified by color-flow Doppler techniques and the maximum jet velocity was measured by continuous-wave Doppler in all patients. Right atrial pressure was estimated as 5 mmHg, 10 mmHg or 15 mmHg on the basis of the size and respiratory change of the inferior vena cava (complete collapse, 5 mmHg; partial collapse, 10 mmHg; no collapse, 15 mmHg) (15). RV systolic pressure was estimated based on the modified Bernoulli equation.
The diagnosis of RV dilatation was determined if the end-diastolic RV diameter was>26 mm in the parasternal long-axis view or a ratio of right-to-left end-diastolic ventricular diameter was>1 in the apical four chamber view. RV hypertrophy was determined when the thickness of RV free wall was≥7 mm in the subcostal view (10, 16).
Statistical analysis
Data are expressed as medians and interquartile ranges (IQRs) for continuous data and as percentages for categorical data. Student's t-test or the Mann-Whitney U-test was used for the comparisons of continuous data; however, for the comparisons among three groups, Kruskal-Wallis test was used. For categorical data, the chi-square or Fisher's exact tests were used. With regard to correlations of BNP levels with other parameters, Spearman's correlation was used. For multivariate analysis, a Cox proportional regression analysis was performed using variables with a P value of<0.05 in univariate analysis. A receiver operating characteristic (ROC) curve was performed for admission BNP levels for predicting subsequent readmission, and an optimal cut-off value was estimated. In addition, Kaplan-Meier survival curve was also performed to compare the intervals to subsequent readmissions between two groups. All reported P values were two-sided, and a P value of<0.05 was considered to indicate statistical significance. All analyses were conducted using the SPSS statistical software package (IBM SPSS Statistics version 21, Standard for Medical Network).
Ethics statement
The protocol of this study was approved by the institutional review board of Hallym University Sacred Heart Hospital (IRB No. 2014-I083) and each hospital. The authors assert that all procedures contributing to this work comply with the Helsinki Declaration of 1975 and its later amendments.
RESULTS
Demographics and clinical data
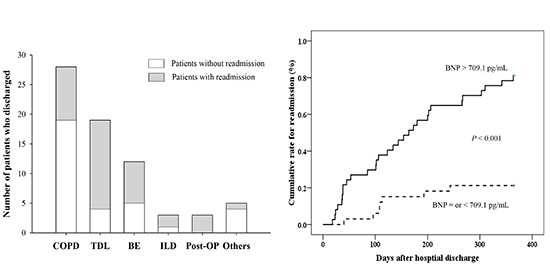
During the study period, 99 patients with chronic cor pulmonale were initially screened from three hospitals; among these patients, 69 were finally enrolled (Fig. 1). The median age was 70.0 (interquartile range, 58.5-76.0) yr, and 50.7% of the patients were female. Among the underlying lung diseases, COPD (40.6%), TDL (27.5%), and bronchiectasis (15.9%) were the most common. Among the interstitial lung diseases (ILD) were tuberous sclerosis (n=1), systemic lupus erythematosus-associated ILD (n=1), and IPF (n=2) (Table 1). Among all of the enrolled patients, 52 (75.4%) had dyspnea of NYHA grade IV, and 73.9% had hypercapnia (PaCO2>45 mmHg) on admission. The median values of admission BNP levels and RV systolic pressures were 986.5 pg/mL (449.5-1,489.0 pg/mL) and 60.0 mmHg (49.5-70.3 mmHg), respectively.
Pulmonary function tests were collected from 56 patients (median time interval to the admissions, 3.0 months [1.0-6.8 months]), and among the three common etiologic groups, patients with TDL had the lowest FVC% and FEV1% values (46.0% [35.0%-57.5%] and 32.0% [28.0%-37.5%], respectively); those for patients with COPD were 65.0% (54.0%-74.3%) and 39.0% (31.5%-50.5%); those for patients with bronchiectasis were 55.0% (39.0%-77.0%) and 41.0% (31.5%-54.0%), respectively (P=0.007 and P=0.130, respectively for all). However, admission BNP levels were not different among these three groups (data not shown). Regarding the treatments, 58.0% of patients were admitted to the intensive care unit, and 14.5% received vasopressors.
Correlations between admission BNP levels and other parameters
As shown in Table 2, admission BNP levels showed no correlation with FVC%, FEV1%, PaO2, or PaCO2. However, admission BNP levels showed a significant correlation with bilirubin levels (r=0.279 and P=0.020) and cardiac troponin I levels (r=0.558 and P<0.001; Fig. 2A). In addition, among 25 patients with both follow-up BNP and echocardiography data available (median time interval, 61.0 days [33.0-92.0 days]), delta BNP showed a good correlation with delta RV systolic pressure (r=0.562, and P=0.003; Fig. 2B).
One-year outcomes and BNP levels
At the 1-yr follow-up, 11 (15.9%) patients died (aggravating RV failure, n=6; pneumonia, n=5), including two hospital deaths. Among the enrolled patients, patients with TDL showed a higher mortality rate than those with non-TDL diseases (31.6% vs. 10.0%, respectively; P=0.059); additionally, patients with TDL showed the highest mortality rate among the three common etiologic groups (vs. 3.6% and 9.1% in patients with COPD and bronchiectasis, respectively; P=0.021). Among 67 patients who were discharged, 36 (53.7%) were readmitted to the hospitals at the 1-yr follow-up. Although all three patients with pneumonectomy experienced readmissions, those with TDL had a higher readmission rate than those with non-TDL diseases (78.9% vs. 43.8%, respectively; P=0.009); the readmission rate was also the highest in patients with TDL among the three common etiologic groups (vs. 33.3% and 63.6% of patients with COPD and bronchiectasis, respectively; P=0.007).
Admission BNP levels did not differ between survivors and non-survivors (data not shown), but the levels were significantly higher in patients who had readmissions than in those who did not (1,380.0 pg/mL [986.5-1,928.7 pg/mL] vs. 462.0 pg/mL [295.9-938.8 pg/mL], respectively; P=0.001).
Receiver operating characteristic (ROC) curves and cut-off value
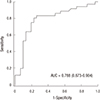
When we performed ROC curve analysis (Fig. 3), the value of the area under the curve (AUC) for admission BNP levels to predict readmission was 0.788 (95% confidence interval [CI], 0.673-0.904). The cut-off value was 709.1 pg/mL, and the sensitivity, specificity, positive predictive value, and negative predictive value were 80.6%, 77.4%, 80.6%, and 77.4%, respectively. The odds ratio was 11.3 (95% CI, 3.3-39.2). In addition, patients with an admission BNP level>709.1 pg/mL had a higher frequency of readmissions (per patient) than did their counterparts (means±standard deviations; 1.3±1.5 vs. 0.3±0.5, respectively; P<0.001).
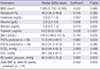
Multivariate analysis for predicting readmission
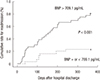
In the univariate analysis (Table 3), age, TDL disease, troponin I, hyponatremia (i.e., [Na+]), and admission BNP levels had a P value less than 0.05. In the multivariate analysis, admission BNP levels (HR, 1.049; 95% CI, 1.005-1.094) and TDL disease (HR, 2.176; 95% CI, 1.028-4.609) were significant predictors of subsequent readmission at the 1-yr follow up. In addition, patients with high BNP levels (greater than the cut-off value) had a shorter time interval before subsequent readmission than those with low BNP levels (log-rank test; P<0.001; Fig. 4).
DISCUSSION
This study revealed several interesting findings. First, the common causes of chronic cor pulmonale were COPD, TDL, and bronchiectasis, and patients with TDL had higher mortality and readmission rates than those with non-TDL diseases. Second, 53.7% of patients had readmission within 1 yr, and admission BNP levels were a significant risk factor for subsequent admission after hospital discharge. Finally, admission BNP levels were well correlated with cardiac troponin I, and delta BNP also correlated with delta RV systolic pressure.
Similar to data in Western countries, the most common cause of cor pulmonale was COPD in the present study. However, we found that TDL, which is a secondary complication after the healing of tuberculosis lesions, was also among the common causes of the condition. Previously, several Asian authors demonstrated the importance of tuberculosis in the development of cor pulmonale (17, 18), and our result is consistent with the fact that Korea was once an area where tuberculosis was endemic (19, 20). However, we also found that patients with TDL had the highest mortality rate among the three common etiologic groups. In previous studies, Park et al. (13) showed a high mortality rate in patients with TDL (i.e., 60.5%), and Bishop and Cross (21) reported that high PH was associated with mortality in patients with chronic respiratory diseases due to tuberculosis. Therefore, these results suggest that among the underlying lung diseases for cor pulmonale, TDL may be one of the common causes and might be associated with poor survival.
Regarding the readmission rate, more than half of the patients had readmissions within 1 yr after hospital discharge. In particular, TDL disease was a significant risk factor and showed the highest readmission rate (78.9%) among the three common etiologic groups. Although data concerning the readmission rate were very limited, in a study by Almagro et al., patients with acute exacerbation of COPD showed readmission rates of 38.5% and 58.5% at the 90-day and 1-yr follow ups, respectively (22). However, hospitalizations in patients with chronic lung disease are usually associated with a long hospital stay, high complication rate, and high hospital cost (23,24,25,26). Therefore, physicians should attempt to decrease the rate of hospital admissions of patients with chronic respiratory insufficiency through thorough patient monitoring and effective treatments.
In previous studies, patients with COPD or pulmonary embolism had increased BNP levels when the condition was complicated by PH or right heart failure (27, 28). In patients with IPAH and IPF (with or without PH), increased BNP levels were a prognostic factor (4, 7, 8). By contrast, in this study, the admission BNP levels were not associated with the 1-yr mortality. In a study of patients with acute exacerbation of COPD, Stolz et al. also showed that BNP levels did not predict short- or long-term mortality (29). However, higher BNP levels were an independent risk factor for subsequent readmissions in this study. The levels were also associated with a short time interval before subsequent readmission and a higher mean frequency of readmissions at the 1-yr follow-up. One of the drawbacks of our study was that we could not investigate patient compliance and serial changes in BNP levels after hospital discharge. We also could not clearly differentiate patients with acute exacerbation of COPD from those with aggravating RV failure. However, our results suggest that admission BNP levels might be helpful for predicting future events after hospital discharge.
Regarding cardiac troponins, many studies have shown that they are also a good prognostic marker in patients with PH (30,31,32). However, we did not find that troponin I was associated with patient outcomes in the multivariate analysis. The causes might be that our study was small-sized or that we excluded all of the patients with left ventricular dysfunction or a history of coronary heart disease. However, we found that BNP levels were well correlated with cardiac troponin I levels in the present study, a finding that was consistent with the results in a study by Heresi et al. (32). In addition, a good correlation existed between delta BNP and delta RV systolic pressure in 25 patients (P<0.001). To date, although several small-sized studies showed that high BNP levels could be an indicator for the presence of cor pulmonale, the correlation of pulmonary artery pressure with laboratory parameters still remain conflicting (9, 33,34,35). However, our results suggest that BNP levels might represent the extent of RV dysfunction, and their changes could reflect changes in RV function at the follow up. This result should be further evaluated in a future large-scaled study.
In the present study, we failed to demonstrate any associations of FVC% or FEV1% with RV systolic pressure and patient outcomes. Although it is well known that PH is a good prognostic factor in various chronic lung diseases, the associations between pulmonary function tests and patient outcomes in cor pulmonale have rarely been studied. In fact, early studies indicated that pulmonary function tests were even poor predictors of the severity of PH in COPD or IPF (36, 37). Therefore, factors other than pulmonary function measurements might play an important role in PH and patient outcomes in cor pulmonale. However, there was a variable time period between pulmonary function measurements and the time of study enrollment, and the study population was heterogeneous in terms of pulmonary function physiology (i.e., obstructive and restrictive patterns) in the present study. Therefore, we cannot draw any firm conclusions in this regard.
This study had several limitations. First, although this was a three-center study, it had a small sample size and was retrospective in nature. Therefore, there is a possibility of unintended bias. Second, we did not perform right-heart catheterization to diagnose pulmonary hypertension. Although several studies have demonstrated discrepancies between echocardiography and right-heart catheterization in measuring the systolic pulmonary artery pressure, we could not perform right-heart catheterization due to acute aggravation of our patients' conditions (15, 38). Third, we could not collect serial BNP data, including discharge BNP levels. As mentioned above, obtaining follow-up data and investigating serial changes will facilitate elucidation of the real implications of BNP levels. However, few current studies have addressed the usefulness of BNP levels in chronic cor pulmonale. We believe that the results of our study will be very meaningful for physicians who are treating patients with chronic cor pulmonale.
In conclusion, among patients with chronic cor pulmonale who were admitted for dyspnea aggravation, 53.7% had readmissions after hospital discharge. In particular, patients with TDL showed the highest mortality and readmission rates. Finally, admission BNP levels are a significant factor for predicting subsequent readmissions. Therefore, intensive treatment and close follow-ups will be needed in patients with high BNP levels.




 XML Download
XML Download