

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
As Abraham Jacobi quoted "Children should not be treated as miniature men and women", the dynamic process of maturation and substantial changes in growth and development in physiology and pharmacology make the difference between children and adults (1). Characteristics in pharmacokinetics and pharmacodynamics as well as proportions of body fat, protein and extracellular water content differ greatly in different age groups, causing different drug safety profiles between pediatric and adult systems.
In the US, the Pediatric Exclusivity Provision of the Food and Drug Administration Modernization Act (FDAMA) passed initially in 1997 and became law under the Best Pharmaceuticals for Children Act (BPCA) in 2002. BPCA gives the pharmaceutical companies an incentive of an additional 6 months of marketing exclusivity if the pediatric clinical trials that the FDA determines to be useful for children are conducted (2). However, there are challenges to facilitate clinical research in children, legally and ethically (3). Lack of clinical trials in pediatrics and uncertainty in effects in pediatric population from animal studies make the off-label use of adult medicines unavoidable and the post-marketing monitoring of drug safety even more essential (4).
Adverse drug events (ADEs) include any injury caused by the drug, which includes adverse drug reactions (ADRs) and medication errors (MEs). And MEs are probably found to be the most common type of ME. When the Institute of Medicine report, "To Err is Human: Building a Safer Health System" was published, the awareness of importance of patient safety during medical intervention was increased (5). The National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) in the US defines a "medication error" as any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in control of the health care professional, patient or consumer (6). The FDA announced that MEs caused one death daily and injured about 1.3 million people annually in the US. Official ME statistics are not estimated in Korea yet, but the magnitude of the problem is assumed to be similar with or even worse than the situation of the US.
According to Korea Consumer Agency press release, out of 551 incidents of accidental poisoning among children between 0 and 14 yr reported to Korea Consumer Injury Surveillance System in 2009-2011, the leading cause of accidental poisoning was medicines (n=111, 20.1%) and the frequency has increased every year. In the US, according to the report by Safe Kids Worldwide, approximately 67,000 children were treated in emergency room for medicine poisoning in 2011 (7). MEs in children are not uncommon either. The ME rate in children was found to be 1 in 6.4 orders according to one study using the hospital medication system (8). One study using the United States Pharmacopeia (USP)'s voluntary medication error reporting system (MEDMARX®) database from 1999 to 2003 showed that out of 580,761 MEs records, 19,350 pediatric ME records (3.3%) were found and three common types of error were improper dose/quantity, omission error and prescribing error (9).
Children stand distinctively to the risk of MEs. They have fewer internal reservoir to buffer any MEs which can make them at greater risk (10). Off-label use is common among pediatricians and complicated dosage calculations are usually required for pediatric dose regimen based on individual body weight and body surface area due to lack of pediatric formulations and dosing information from the manufacturer. This eventually causes higher risks of dosing error. Several reports have shown that MEs are common in pediatric population and even three times more likely than adults (11).
To describe the characteristics of pediatric MEs in Korea, we analyzed the data of pediatric MEs by year, types of MEs and therapeutic groups, and compared with adult MEs using Korea Adverse Event Reporting System (KAERS) database from 1989 to 2012.
MATERIALS AND METHODS
Setting
The spontaneous ADE reporting system in Korea was introduced in 1988 and the online reporting system was started in 2000 which were regulated by Korea Food and Drug Administration (KFDA). In 2012, the pharmacovigilance activities were transferred to Korea Institute of Drug Safety & Risk Management (KIDS), which developed KAERS database. KAERS database includes a database that contains information on ADE and ME reports submitted to KFDA before September 30, 2012 and to KIDS after October 1, 2012. For many years, only pharmaceutical companies and health care professionals have been able to submit reports since the system was introduced. Direct reports by patients were allowed in 2000. ADE reports including ME reports are submitted to KAERS database via paper forms, the telephone, FAX, or electronically on KIDS website.
Classification of age-group
A classification of the pediatric population was according to the internationally agreed standard by WHO which was up to 18 yr of age. Nineteen years old and older was classified as adult population.
Classification of ME
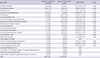
Each report in KAERS database contains information including, but not limited to, identifiable reporter and patient, report date, date of event, products involved, type of ADEs or MEs, health conditions and causality assessments. ADEs and MEs in KAERS database were coded to terms in Korean translations of World Health Organization Adverse Reactions Terminology (WHO-ART). WHO-ART consists of hierarchical structures at four different levels; System of Organ (SOC, 1st level), High level term (HLT, 2nd level), Preferred term (PT, 3rd level), Included term (IT, 4th level). HLT on "ME-related problem" included 38 ITs. Except 9 terms regarding drug quality problem and error related to medical device and drug interaction, 29 ME-related terms were selected for this analysis. The terms related to ME are listed in Table 1.
Classification of Medicines
Medicines involved with pediatric MEs were classified according to the Anatomical Therapeutic Chemical (ATC) classification system (12). Medicines are classified in groups at five different levels; anatomical main groups (1st level), pharmacological/therapeutic subgroups (2nd level), chemical/pharmacological/ therapeutic subgroups (3rd and 4th level) and chemical substance (5th level). In this study, the number of reports in total pediatric MEs by ATC code at 2nd level was analyzed.
Analysis method of ME reports in pediatrics
ME reports in pediatrics and adults was retrieved from KAERS database. Reports with missing their age information were excluded for the analysis. Initial and follow-up reports of one patient were counted only once (Fig. 1). To determine the characteristics of pediatric ME reports, types of MEs were presented and the significance test for comparison with adult population was carried out using a chi-square tests. Differences were tested using an α level of 0.05. All analysis was performed using SAS 9.3 software. The narratives of the reports were reviewed to determine the severity of harm and outcomes. Study process of pediatric MEs is presented in Fig. 2.
RESULTS
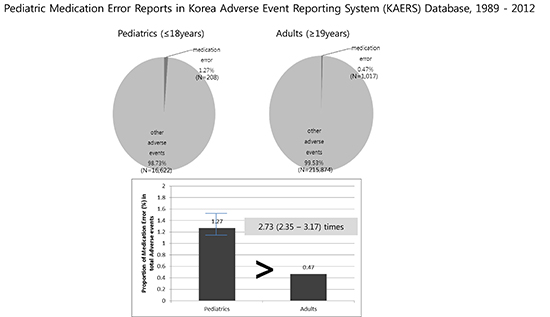
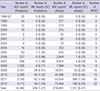
We collected 1,225 ME reports in pediatrics (208 reports) and adults (1,017 reports) from 1989 to 2012 (Table 2). The proportion of pediatric ME in ADE reports was 1.27% compared with 0.47% in adult, it was 2.73 times (95% confidential interval [CI], 2.35-3.17) higher than Adult ME (Table 3).
Multiple medicines and ME terms could be entered in 1 reports. The number of ME-term code in KAERS database was 236 and the most common type of ME reported in terms coded in KAERS database was "accidental overdose", followed by "drug maladministration" and "medication error" (Fig. 3). "Accidental overdose" in pediatrics was 8.01 times (95% CI, 5.24-12.25) higher than adults. In addition, "drug maladministration" and "medication error" in pediatrics were 4.08 times (95% CI, 2.74-6.07) and 1.50 times (95% CI, 1.03-2.20) higher than adults (Table 4).
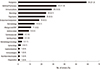
The number of medicines involved in 208 pediatric ME reports was 237 and 17 therapeutic groups; and the most frequently reported therapeutic group was "analgesics", followed by "drugs for obstructive airway disease" and "vaccines" which were commonly used in pediatrics (Fig. 4).
After the narratives of all 208 reports were reviewed, most of them did no harm to patients, but some cases were resulting in harm which was needed for medical treatment. In cases of 5-yr child's hypersensitivity reaction caused by drug dispensing error and 28-month infant's unconsciousness caused by accidental drug intake on mistaking drug for candy, the patients were hospitalized and recovered with no sequella.
We identified that there was no specific code of "omission" in the KAERS database, so the two cases regarding "omission" reports were coded as "Incorrect Drug Administration Duration" and "Inappropriate Schedule of Drug Administration", respectively. Additionally, 10 reports were false ME reports. They were ADRs, not MEs.
DISCUSSION
The safe drug use movement has grown rapidly in the past decade in Korea. However, this study showed that the total number of pediatric ADE reports and ME reports has not increased throughout the years compared to the rapid increase in total number of ADE reports during the recent years. The increased number of ADE reports contributes to establishment of regional pharmacovigilance centers (RPVCs) across the country after 2006: 3 RPVCs in 2006, 6 in 2007, 9 in 2008, 15 in 2009, 20 in 2011 and 22 RPVCs in 2012. However, the effective system to detect and analyze the causality and risk factors contributing to ME to prevent future errors is lacking. Furthermore, the impact of ME occurred in pediatrics are much more serious. One study of USP Medication Errors Reporting Program showed that there was a significantly increased rate of ME resulting in harm or death in pediatrics (31%) compared to adults (13%) (13).
This is the first study to analyze the MEs in pediatrics using the national spontaneous ADE reporting system database accumulated since the system was introduced in Korea in 1988. The proportion of pediatric MEs in ADE reports was significantly higher than Adult MEs, therefore, it is necessary to aware the problem in MEs in pediatrics. The data from this study may be used as resources for medication safety tools. For example, appropriate storage of medicines away from the pediatrics would be a good starting point since the most common type of error reported was "accidental overdose" and the therapeutic group of medicines most frequently associated with the error reports was "analgesics" from this study. The second and third most common types of error were "drug maladministration" and "medication error" in this study. The causes and factors contributing to this error could not be identified for all reports, however, many of the reports showed that misunderstanding of the drug labels and lack of pediatric formulations led to the MEs. One systematic review showed that 11 out of 16 reviewed articles demonstrated that the most common cause of ME was dosing error (14). One US study using the national medication error reporting system database showed that 47% of the MEs identified in pediatrics was improper dose/quantity (13). Dosing calculations are frequently done based on child's body weight and body surface area; and mistakes can be easily made in the process. The dosing error in pediatrics can result in even greater risk for potent drugs when they require small dosing amount. However, only 26.3% of pediatric ME reports in this study were identified as dosing error. We assume that there may be more MEs including dosing error which had not been reported.
This study demonstrated that ADE terminologies coded in KAERS database could not be completely translated into the type of medication error after reviewing the descriptive contents of the reports. Many reporters chose "drug maladministration" and "medication error" which were overall terms for all medication error. A total of 91 terms out of total 236 ME terms was reported as "drug maladministration" and "medication error". The term of "omission" had not been coded in KAERS database. There should be a review of adding the appropriate reporting terms to KAERS database for these types of errors. Ten reports regarding false medication errors were found which were identified as reports by patient where they were unable to distinguish between the MEs and ADRs. This study showed that the terminology to describe MEs and ADRs can cause confusion. Many patients have difficulty in understanding the definition and relationship between MEs and ADRs. User-friendly educational and training programs to aid in ADE reporting process need to be developed and application of standardized terminology to describe the medication errors should be made.
We found several limitations to be improved. First, the ME report rate in pediatrics was very low in contrast to dramatically increased overall ADE reporting rate during the study period. Low reporting rate of ME does not imply that the ME has not occurred. Second, the ME events reported to KAERS database are lacking the information on cause of the error as well as the outcome of the error. And lastly it is hard to know at which step of the medication-use process (e.g. prescribing, documenting, dispensing, administering or monitoring) the error occurred.
Institute for Safe Medication Practice Medication Errors Reporting Program (ISMP MERP) is a good example of a well-operated national ME reporting system. The reviewed ME reports are analyzed and used for early warning, prevention, regulatory change and standards involving drug packaging, labeling and nomenclature changes. ISMP makes ongoing collaboration and relationship with various associations including the FDA and NCC MERP.
Trial and error is not acceptable among pediatrics. However, mistakes can always happen. To reduce and help prevent MEs in pediatrics the following efforts should be made: Education and training on medication error prevention should be provided to health care professionals regularly. This will help increase the awareness on error prevention. One study showed that well-trained physicians on ME were the ones least likely to make errors (15). Hospitals and health care organizations can reduce the ME by adapting new technology with computerized system. Scared to get the punishments, hospitals and health-care professionals are reluctant to make reports of the errors. Making a blame-free environment is very important so that the MEs can be studied and preventive measures can be implemented (16).
Many drugs are available in adult formulations and the appropriate pediatric products have to be prepared extemporaneously in the pharmacy or hospital. These practices increase additional risk of making MEs in the process. Lack of safety information due to lack of pediatric clinical studies results in off-label use of medicines. Pharmaceutical companies and government should work together to develop pediatric medications with approved safety profiles through well designed clinical trials (17).
For consumers, knowing which medications have been prescribed and are being taken should be emphasized. Understanding the concept of medical error, which includes ME showed a significant impact on patient's knowledge for preventing errors in one study (18). And when in doubt, they should ask questions to appropriate persons. ME in pediatrics can also happen at home which can lead to harm. Accidental poisoning due to wrong storage of medicines is one type of ME which cannot be ignored. This study showed 26% of the pediatric medication error reports were related to accidental drug intake by the child. These are 100% preventable accidents by putting the medicines away from children or using the child-resistant packaging.
Lastly, it should be urgently needed to develop an effective and reliable national ME reporting system apart from the current ADE reporting system. Many hospitals in Korea have their own ME reporting system, however each hospital system operates separately and the error statistics are not shared for future prevention. The new reporting system at national level should be able to identify the cause, type, outcome of the error and also identify "near misses" where no harm has occurred or the incident has been prevented. Also it should be able to analyze the nature of the ME to prevent the future mistakes. For a successful development of ME reporting system, it should be promoted the enviroment that health professionals, maufacturers and consumers report not only the ME arrived patients, but also near-miss. The confidentiality and protection of the information reported and the reporters should be guaranteed.
In conclusion, this study shows that MEs in pediatrics would not be negligible in Korea and we expect that this study would increase the awareness of the problem in MEs in pediatrics and need for development of an effective national ME preventing system in Korea.





 XML Download
XML Download