

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
West Nile encephalitis is a mosquito-borne disease endemic to Africa, Asia, Australia, and Europe and the West Nile virus is a single-stranded RNA virus which belongs to the Japanese encephalitis serogroup of flaviviruses (1). It could be accompanied with various neurologic symptoms and signs including headache, mental confusion, optic neuritis, and muscle weakness (2, 3, 4). After the first two cases of West Nile encephalitis were diagnosed in 1999 in New York (5), many neurological abnormalities were noted in patients of West Nile encephalitis, and the flaccid muscle weakness is a distinctive feature of this disease (2, 3, 6). Until now, West Nile encephalitis was never diagnosed in Korea, and it is the first report of West Nile encephalitis in Korea.
CASE DESCRIPTION
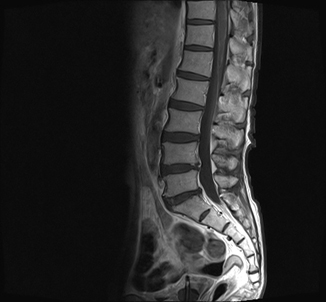
A 58-yr-old man was admitted with headache for 2 months in June 2012. The patient had been on a business trip in Guinea, West Africa since 7 months ago. The headache was described as throbbing and dullness of diffuse area. He denied other symptoms such as nausea, vomiting, neck stiffness, and dizziness. He presented mild memory disturbance, cognitive impairment and slow speech. The headache and cognitive impairment had been worsening and accompanied general weakness and weight loss 10 kg for 2 months. The patient's past medical history was significant for diabetes mellitus. He had no hypertension, cardiac diseases, chronic renal disease, and liver disease. He denied previous infectious disease such as upper respiratory infection or diarrhea. There was no history of trauma. He had a 20 pack-year history of smoking and no recent alcohol intake. The patient denied using any medications except for antimalarial drug (sulfadoxine 500 mg, pyrimethamine 25 mg, artemether 80mg/mL) and analgesics in Africa. At admission to our hospital, he was afebrile (36.4℃) and his vital signs were blood pressure 121/78 mmHg, heart rate 97/min, and respiratory rate 20/min with normal findings of physical examinations. Findings on initial neurologic examinations were normal except minimental state examination (MMSE) with score 20. He was incorrect on time orientation, serial 7 and delayed recall tests. Admission complete blood count revealed hemoglobin of 12.7 g/dL, leukocyte count of 16.2 × 109/L with 79% neutrophils, and a platelet count of 388 × 109/L. The patient's calcium level, chemistries, and liver function tests were normal and CRP was slightly increased. Electrocardiogram and chest X-ray study were normal. Analysis of cerebrospinal fluid (CSF) demonstrated 0 RBC/µL, 214 WBCs/µL (with 80% lymphocytes and 12% neutrophils), a protein level of 161.9 mg/dL, a glucose level of 93 mg/dL and ADA level of 4.8. Treatment with acyclovir was initiated. A brain magnetic resonance imaging (MRI) revealed multifocal patchy T2 high signal lesions in both temporal lobes, basal ganglia, internal capsule posterior limb, and corona radiata, which suggested encephalitis. Electroencephalogram showed frequent semirrhythmic medium amplitude delta slowing on both hemispheres, with frontal dominancy. On hospital day 1, his body temperature was 38.0℃ and malaria test was negative. He presented urinary difficulty on hospital day 3. Follow up CSF tapping was done on hospital day 3 and 6 RBC/µL, 340 WBCs/µL (with 67% neutrophils and 28% lymphocytes), a protein level of 164.6 mg/dL, a glucose level of 70 mg/dL and ADA level of 6.0. TB medication added on hospital day 6. The patient complained of both leg weakness and the motor strength of bilateral lower extremity was 4+/4+. He also complained of both leg pain and paresthesia, deep tendon reflex on both lower extremities were areflexia. There was no remarkable finding on nerve conduction study (NCS) and needle electromyogram (EMG), but arachnoiditis and myelitis were observed on lumbar spine MRI (Fig. 1). Blood and CSF cultures were negative. Polymerase chain reactions (PCR) for HSV, VZV, EBV, CMV, enterovirus, tuberculosis, and Mycoplasma pneumonia were negative in CSF. Serological test for brucellosis, Lyme disease, leptospirosis, Hantann virus and Tsutsugamuchi disease were negative at admission. Antibody test of Japanese B encephalitis was negative in serum. Antibody test for West Nile virus was positive by indirect immunofluorescence assay. An additional serological study for specific antibody for West Nile virus was done, the total antibody titer of West Nile virus was 1:337, and follow up titer after 2 weeks was 1:1,632 in serum by plaque reduction neutralization test. He was diagnosed with West Nile encephalitis in July 2012. Treatment with interferon-α 3mu was started and maintained for 2 weeks. Follow up CSF tapping was done after one month later and 9 RBC/µL, 9 WBCs/µL (with 16% neutrophils and 67% lymphocytes), a protein level of 99.9 mg/dL and a glucose level of 66 mg/dL. His weakness and pain at the leg was completely recovered after 3 months.
DISCUSSION
The case was the first identified West Nile encephalitis in Korea. Encephalitis with severe muscle weakness is a common symptom and may provide a diagnostic clue. To confirm a diagnosis, it needs identification of West Nile virus in serum or CSF. Viral RNA of West Nile can be identified by reverse transcription PCR. But the patient has already passed two months after symptom onset. IgM antibody is usually detectable only during a few days of illness (7). Another method is the identification of a change by a factor of four or more in the antibody titer or virus-neutralization tests (7), the case was positive for the virus-neutralization tests. Serological test and PCR for other infectious agents were all negative and autoimmune encephalitis such as NMDA receptor encephalitis was excluded by clinical symptoms (8). So we can confirm a diagnosis.
West Nile encephalitis is a unusual encephalitis associated with muscle weakness. Many studies indicated that the weakness was probably caused by infection and inflammation in the anterior horn cells of the spinal cord and brainstem like poliomyelitis (6, 9, 10). Electrophysiologic studies showed reduced compound muscle action potentials, and normal sensory nerve action potentials, which is distinguished from Guillain-Barre syndrome (3, 6, 9, 10). A few autopsy studies demonstrated that the inflammatory changes with severe leukocytic inflammation of the anterior horns with striking loss of motor neurons (4, 11). But this case did not present any abnormalities in the electrophysiologic study. He complained about severe sensory symptoms with leg pain and arachnoiditis was observed in lumbar MRI. Only a few reports noted a caudal equine enhancement (4) and weakness due to acute radiculitis (12). It's hard to say that his weakness was caused by only radiculopathy, because paralysis of the West Nile encephalitis generally results from anterior horn cell damage. But in this case, radiculopathy also contributes the motor weakness of the West Nile encephalitis.
At present there is no established treatment for West Nile encephalitis and basic treatment is a supportive care. But because it's a fatal disease, sometimes it was treated with plasmapheresis or administration of IV immunoglobulin (5). Interferon-α has been reported to inhibit West Nile virus replication, and some successful cases were reported using of interferon-α to treat West Nile encephalitis (13). Our patient was treated with interferon-α properly, and was recovered.
It was the first case of West Nile encephalitis in Korea. Korea is not an endemic area of West Nile virus, but an increasing overseas trip poses a risk of the influx of overseas diseases and may contribute to the global spread of infectious diseases. So an understanding of overseas infectious disease will help us diagnose a precise disease.
 XML Download
XML Download